Acute glomerulonephritis is a broad term used to describe several disease processes that result in glomerular injury. The glomerular injury is the result of antigen-antibody deposits within the glomeruli. It occurs most frequently in school-age children, is rare in children younger than age 2, and occurs more frequently in males than in females (2:1).
Pathophysiology and Etiology
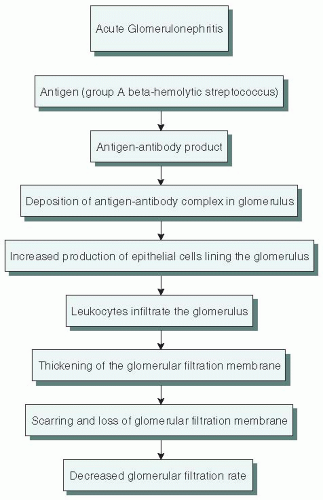
Presumed cause—antigen-antibody reaction secondary to an infection elsewhere in the body (see Figure 49-1).
The initial infection is usually either an upper respiratory infection (URI) or a skin infection.
Most frequent causative agent—nephritogenic strains of group A beta-hemolytic streptococcus.
It is speculated that the streptococcal infection is followed by the release of a membrane-like material from the organism into the circulation.
Antibodies produced to fight the invading organism also react against the glomerular tissue, thus forming immune complexes.
The immune complexes become trapped in the glomerular loop and cause an inflammatory reaction in the affected glomeruli.
Changes in the glomerular capillaries reduce the amount of the glomerular filtrate, allow passage of blood cells and protein into the filtrate, and reduce the amount of sodium and water that is passed to the tubules for reabsorption.
General vascular disturbances, including loss of capillary integrity and spasm of arterioles, are secondary.
Clinical Manifestations
Onset
Usually 7 to 15 days after acute pharyngitis. In streptococcal skin infections, the latency period may be as long as 4 to 6 weeks.
May be abrupt and severe or mild and detected only by laboratory measures.
Signs and Symptoms
Urinary symptoms:
Decreased urine output.
Bloody or brown-colored urine.
Edema.
Present in most patients.
Usually mild.
Commonly manifested by periorbital edema in the morning.
May appear only as rapid weight gain.
May be generalized and influenced by posture.
Hypertension.
Present in up to 70% of those hospitalized with glomerulonephritis.
Usually mild.
Rise in blood pressure (BP) may be sudden.
Usually appears during the first 4 to 5 days of the illness.
Pallor.
Malaise, lethargy.
Low-grade fever.
Mild headache.
GI disturbances, especially anorexia and vomiting.
Figure 49-1. Sequence of events in acute glomerulonephritis.
Diagnostic Evaluation
Urinalysis:
Decreased output (oliguria)—may approach anuria.
Microscopic or gross hematuria (noted in 30% to 70% of all cases).
Specific gravity—moderately elevated.
Proteinuria may be mild to severe.
Microscopic—red blood cells, leukocytes, epithelial cells, and casts.
Low urinary sodium may be noted.
Blood urea nitrogen (BUN) and creatinine—usually mildly to moderately elevated; however, normal in 50% of cases.
Antistreptolysin-O titer—elevated initially.
Anti-DNase B titer—elevated.
Erythrocyte sedimentation rate—elevated.
Complement C3 and complement C4—depressed.
If indicated chest x-ray—may show pulmonary congestion, cardiac enlargement during the edematous phase.
Management
Antibiotic therapy may be initiated if there is any concern that streptococci or other organisms are still present.
Other management is mostly symptomatic; in most patients, spontaneous recovery is expected. Hospitalization is usually not necessary.
Salt and fluid intake should be restricted during the acute phase of the disease.
Diuretics should be administered if significant edema or hypertension develops.
A renal biopsy may be indicated if the child does not recover from apparent acute poststreptococcal glomerulonephritis.
Complications
The following complications occur infrequently.
Circulatory congestion—if severe can lead to pulmonary edema.
Hypertensive encephalopathy.
Acute renal failure.
Anemia.
Nursing Assessment
Obtain history regarding recent streptococcal infection.
Obtain appropriate cultures and assess for current infection.
Measure urine output and degree of hematuria and proteinuria.
Weigh child and document areas and extent of edema.
Obtain baseline BP reading to assess for hypertension.
Nursing Diagnoses
Impaired Urinary Elimination related to glomerular dysfunction.
Excess Fluid Volume related to impaired renal function.
Deficient Diversional Activity related to prolonged illness and restrictions.
Deficient Knowledge regarding acute glomerulonephritis and its management.
Nursing Interventions
Promoting Normal Urine Output
Monitor daily intake and output.
Test and record urine for hematuria and proteinuria, as directed. Note color of urine.
Monitor daily weight.
Reducing Excess Fluid Volume
Provide a no-salt-added diet during the acute phase of the illness. Other restrictions may be indicated if renal function is impaired. Protein intake is not usually restricted because of the possible risk of malnutrition.
Restrict fluids in children with hypertension, edema, heart failure, or renal failure.
Place a sign that indicates dietary restrictions on the child’s bed so that staff and visitors will be aware of special needs.
With fluid restrictions, offer small amounts of fluids spaced at regular intervals throughout the day and evening. Use an appropriate-size cup for the amount of fluid being offered.
Check BP, as ordered or needed, and observe for signs of hypertension. Administer antihypertensive and diuretic drugs, as ordered by health care provider.
Promoting Diversional Activity
Explain fluid restriction at an age-appropriate level and direct the child’s focus away from restrictions.
Provide the child with diversional activity and play therapy.
Encourage activity, as tolerated.
Providing Information
Explain all aspects of the diagnostic tests and treatment in terms the family can understand.
Explain the purpose of all medications and the restricted diet, including a review of high-sodium foods to avoid and sample menus.
Encourage family participation in the child’s care.
Help the family plan for adaptation of the child’s nursing care to the home environment.
Arrange for appointments for continued medical supervision and initiate referrals when appropriate.
Family Education and Health Maintenance
Reinforce medical explanation of the disease process.
Emphasize the need for medical evaluation and culture of all sore throats for all family members.
Alert the family to signs and symptoms of disease recurrence.
Be aware that microscopic hematuria may persist up to 2 years.
Reinforce activity recommendation; usually not restricted.
Advise that tonsillectomy or other oral surgery is not recommended for several months after the acute phase of glomerulonephritis.
If this type of surgery is necessary, penicillin may be recommended before and after the procedure to prevent bacterial infection.
Obtain information regarding drug allergies before administering penicillin.
Evaluation: Expected Outcomes
Output remains adequate.
Weight returns to baseline.
Child does age-appropriate activities, as tolerated, and does not complain of thirst.
Parents and child can state rationale for treatment.
Nephrotic Syndrome
Nephrotic syndrome is characterized by heavy proteinuria, hypoalbuminemia, and edema. The syndrome can be subdivided into congenital, primary (idiopathic), and secondary types. Approximately 85% to 95% of primary cases in preadolescents are classified as minimal-change nephrotic syndrome (MCNS) and are associated with minimal histologic change in the glomeruli. Nephrotic syndrome afflicts approximately 16 per 100,000 children younger than age 16 in the United States annually; in young children, it is slightly more common in males than in females, but it disappears in teenagers and adults. The most common age for presentation is 2 years and 70% to 80% of cases occur in children younger than age 6.
Underlying defect is thought to be caused by the loss of charge selectivity of the glomerular basement membrane, which permits negatively charged proteins, primarily albumin, to pass easily through the capillary walls into the urine.
Excessive urinary loss of protein and catabolization by the kidney of circulating albumin leads to a decrease in serum protein (hypoalbuminemia).
The colloidal osmotic pressure that holds water in the vascular compartments is reduced because of the decrease in the amount of serum albumin. This allows fluid to flow from the capillaries into the interstitial spaces, thus producing edema.
The shift of fluid from the plasma to the interstitial spaces reduces the vascular fluid volume (hypovolemia), which in turn stimulates the renin-angiotensin system and the secretion of antidiuretic hormone and aldosterone.
Tubular reabsorption of sodium and water is increased for intravascular volume.
The loss of proteins, particularly immunoglobulins, predisposes the child to infection.
Clinical Manifestations
Onset is insidious—thought to be caused by immune system disturbances because it commonly occurs after a mild URI.
Edema is typically the presenting symptom.
Edema may be minimal or massive.
Edema is usually first apparent around the eyes.
Dependent edema occurs in areas of the body such as the hands, ankles, feet, and genitalia.
Fluid that accumulates in the body spaces may give rise to ascites and pleural effusions.
Striae may appear on the skin from overstretching.
Profound weight gain caused by edema; the child may actually double normal weight.
Decreased urine output during the edematous phase—urine appears concentrated and frothy.
Pallor, irritability, lethargy, and fatigue.
GI disturbances, including vomiting, diarrhea, abdominal pain, and anorexia caused by edema of intestinal mucosa.
Diagnostic Evaluation
Urinalysis:
Proteinuria (tests for albumin)—2+ (>1.0 g/L) on urine dipstick; should be sent for urine protein to creatinine ratio (first voided or random spot urine) to confirm. Considered nephrotic range if >200 to 250 mg/mmol.
Blood—gross hematuria is not present but microscopic hematuria may be found in about 20% of patients.
Twenty-four-hour urine collection is the gold standard for quantification of urine protein—nephrotic range > 40 mg/m2/hour.
Blood tests.
Total protein—reduced.
Albumin—less than 2.5 g/dL.
Complete blood count may show decreased hematocrit due to hemodilution.
BUN may be elevated, indicating general renal function.
Creatinine—usually normal but may be increased if intravascularly depleted.
Electrolytes—may be sodium, potassium, CO2, and calcium imbalances.
Increased serum cholesterol and triglycerides—due to reactive protein synthesis by the liver in response to hypoproteinemia.
Renal biopsy is indicated to look for other cause of renal dysfunction if patient has persistent proteinuria after 4 to 8 weeks of steroid therapy (median time to remission is 10 days—negative or trace proteinuria for 3 consecutive days). Biopsy also indicated if atypical presentation such as persistent renal failure, age less than 1 year or greater than 10 years, use of nephrotoxic drugs, or persistent hematuria.
Management
Steroid Therapy
Corticosteroid therapy—prednisone or prednisolone are drugs of choice due to lower cost and are less likely to induce salt retention and potassium loss.
No standard program of therapy exists; however, the 2012 Kidney Disease: Improving Global Outcomes guidelines recommend:
Corticosteroid therapy be given for at least 12 weeks.
Oral prednisone be administered as a single daily dose starting at 60 mg/m2/day or 2 mg/kg/day to a maximum 60 mg/day.
Daily oral prednisone be given for 4 to 6 weeks followed by alternate-day medication as a single daily dose starting at 40mg/m2 or 1.5mg/kg (maximum 40mg on alternate days) and continued for 2 to 5 months with tapering of the dose.
Corticosteroid therapy should be discontinued slowly to avoid complications of steroid withdrawal, particularly benign intracranial hypertension.
Children with nephrotic syndrome may respond to steroid therapy in several ways:
Steroid sensitive: achieving remission within 28 days of the start of corticosteroid therapy.
Steroid-dependent: relapses on alternate-day dosing or relapses within 14 days of corticosteroid discontinuation.
Steroid resistant: persistent proteinuria after 8 weeks of corticosteroid therapy.
Children with steroid-responsive MCNS have a favorable long-term prognosis.
Evidence Base
Kidney Disease: Improving Global Outcomes (KDIGO) Work Group. (2012). Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney International, 3(1). 1-150.
Alternative Drug Therapies
Should be considered when children relapse frequently (greater than four relapses in 1 year or two relapses in 6 months), become steroid resistant or steroid dependent, or demonstrate unacceptable adverse effects of steroid therapy (steroid toxicity). The decision to use alternative therapy in conjunction with steroids should be made by an experienced pediatric nephrologist.
Immunosuppressants.
Cyclophosphamide.
Cyclosporin A.
Tacrolimus.
Mycophenolate mofetil.
Rituximab.
Intravenous (IV) Albumin 25%
To shift fluid from interstitial space into the vascular system.
Only a temporary treatment to relieve edema but may be used in severe cases of edema that cause respiratory distress or severe discomfort.
Diuretic therapy is used in combination with IV albumin to help relieve edema. In cases of hypovolemia, diuretics may not be indicated.
Complications
Infections:
Peritonitis, most commonly caused by Streptococcus pneumoniae, but may also be caused by Escherichia coli and Haemophilus influenzae.
Gram-negative septicemia.
Staphylococcal cellulitis.
Thromboembolic events.
Hypertension.
Hyperlipidemia.
Pulmonary edema.
Bone disease secondary to corticosteroid therapy.
Acute renal failure.
Nursing Assessment
Obtain history of onset of illness and symptoms.
Precipitating events.
Recent immunizations.
Recent URIs.
Flulike symptoms.
Time of onset and location of edema.
Urinary pattern changes.
Perform physical examination focusing on vital signs; auscultation of breath sounds to determine adventitious sounds; areas and extent of edema, especially periorbital region, extremities, genitalia, abdomen; and peripheral perfusion, including pulses, color, warmth of extremities.
Nursing Diagnoses
Excess Fluid Volume related to fluid accumulation in tissues.
Risk for Infection related to urinary loss of proteins and chronic steroid use.
Imbalanced Nutrition: Less Than Body Requirements related to loss of proteins through urine and anorexia.
Interrupted Family Processes related to childhood illness.
Nursing Interventions
Relieving Excess Fluid
Administer corticosteroids, as directed.
Observe for adverse effects and complications of therapy such as Cushing’s syndrome—increased body hair (hirsutism), rounding of the face (“moon face”), abdominal distention, striae, increased appetite with weight gain, cataracts, and aggravation of adolescent acne.
Stress that these physical changes are not harmful or permanent and that they will disappear after the steroid treatment is stopped.
Observe for serious adverse effects and uncommon complications of corticosteroids (see page 914).
Administer immunosuppressive drugs, as prescribed.
Make sure that patient and parents understand the desired and adverse effects of therapy.
Observe for complications of therapy, such as decreased white blood cell (WBC) count, increased susceptibility to infection, hair loss or increased hair growth (hirsutism), gingival hyperplasia, hemorrhagic cystitis.
Administer diuretics, as prescribed.
Be aware of those diuretics that may cause potassium depletion.
Offer foods high in potassium, such as orange juice, bananas, and dried fruits (eg, raisins, apricots).
Administer supplemental potassium chloride, as ordered, and if the urine output is adequate.
Encourage activity, as tolerated.
Restrict fluids as ordered (usually only during the extreme edematous phases).
Restriction is carefully calculated at frequent intervals, based on the urine output of the previous day plus estimated insensible losses.
Offer small amounts of fluids spaced at regular intervals throughout the day and evening. Use a cup of appropriate size for the amount of fluid being offered.
Measure fluids accurately in graduated containers. Do not estimate fluid intake or output.
Place a sign on the child’s bed to make sure that no urine is accidentally discarded and that all intake is recorded.
Determine total intake and output every 8 hours. In children who are not toilet trained, a fairly accurate record of output can be obtained by weighing diapers before and after voiding.
Record other causes of fluid loss, such as the number of stools per day, perspiration.
Assist with abdominal paracentesis; this may be required because of marked ascites. During the procedure, fluid is withdrawn from the peritoneal cavity to relieve pressure symptoms and respiratory distress.
Restrict sodium, as ordered (usually done while the child is on corticosteroid therapy). A starting point is 1.5 to 2 g/day.
Use a low-sodium menu when ordering meals from the hospital.
Assist family in making food choices that are low in sodium.
Foods that should be limited include cured, salted, canned, or smoked meats; processed cheese; regular canned or frozen soups and bouillon cubes; salted crackers and other snack foods.
NURSING ALERT
No live vaccinations or immunizations should be given during active episodes of nephrosis or while the child receives immunosuppressive therapy.
DRUG ALERT
Administer cyclophosphamide in the morning, with large volumes of fluid, to prevent concentration of the drug in the urine and increased susceptibility to cystitis.
Preventing Infection
Monitor complete blood count for decreased WBC count and neutropenia.
Closely observe the child who takes corticosteroids for signs of infection. Be aware that fever and other symptoms may be masked.
Provide meticulous skin care to edematous areas of the body.
Bathe the child frequently and apply powder. Areas of concern are moist parts of the body and edematous male genitalia. Support the scrotum with a cotton pad held in place by a T-binder, if necessary, for the child’s comfort.
Position the child so that edematous skin surfaces are not in contact. Place a pillow between the child’s legs when lying on side.
Elevate the child’s head to reduce edema.
If possible, avoid invasive procedures, such as femoral venipunctures and I.M. injections, to decrease the chance of introducing pathogens. Venipuncture of the lower extremities may also predispose the child to thromboembolism because of hypovolemia, stasis, and increased plasma concentration of clotting factors.
Educate parents regarding signs and symptoms of possible infections.
Enhancing Nutritional Status
Assess nutritional intake, growth, and development as appropriate for age.
Provide a diet low in sodium, fat, and sugar. Place a sign on the child’s bed that indicates dietary restrictions so that everyone will be aware of special needs.
Provide food choices that appeal to the child and that are easy to eat according to stage of development.
Provide nutritional supplements, as needed.
Providing Emotional Support
Encourage frequent visiting and allow as much parental participation in the child’s care as possible. Hospitalization, if necessary, is usually brief.
Allow the child as much activity as tolerated.
Balance periods of rest, recreation, and quiet activities during the convalescent phase.
Allow the child to eat meals with family or other children.
Encourage the child and family to verbalize fears, frustrations, and questions.
Be aware that young children frequently fear abandonment by their parents.
Allow parents to express frustrations regarding the uncertainties associated with the cause of the disease, the clinical course, and the prognosis.
Explain the difference between nephritis and nephrosis if parents have questions.
Help the child adjust to changes in body image, such as cushingoid appearance, by explaining changes ahead of time.
Discuss the problems of discipline with the parents. Encourage them to set consistent limits and reasonable expectations of their child’s behavior.
Suggest parents get involved with a support group for families of children with chronic illnesses, as needed.
Family Education and Health Maintenance
Prepare the family for home management of the child’s care plan.
Have the dietitian discuss special diets with the parents.
Teach the parents about the child’s medication—the desired effects and the potential adverse effects.
Demonstrate urine testing for protein.
Initiate a community health nursing referral, if necessary, for reassessment and reinforcement of teaching.
Encourage continued medical follow-up visits.
Emphasize the necessity of taking medication according to the prescribed schedule and for an extended time. Discuss complications encountered with steroid therapy.
Teach prevention and recognition of signs and symptoms of infection.
Advise family on necessary activity restrictions.
Teach signs and symptoms of relapse (proteinuria on urine dipstick at home, increased edema, decreased urine output) and whom and when to call with questions.
Teach signs and symptoms of fluid imbalances (excess or dehydration).
Evaluation: Expected Outcomes
Decreased edema and ascites; adequate urine output.
Exhibits no signs of infection.
Family verbalizes and follows dietary restrictions as demonstrated by appropriate weight gain/loss.
Family verbalizes concerns regarding child’s illness as demonstrated by open communication with staff and other family members.
Urinary Tract Infection
Evidence Base
American Academy of Pediatrics. (2011). Urinary tract infection: Clinical practice guide line for the diagnosis and management of the initial UTI in febrile infants and children 2 to 24 months. Subcommittee on Urinary Tract Infection. Steering Committee on Quality Improvement and Management. Pediatrics, 128, 595-610.
Koyle, M., & Shifrin, D. (2012). Issues in febrile urinary tract infection management. Pediatric Clinics of North America, 59(4), 909-922.
Urinary tract infection (UTI) is defined as bacteria that exists anywhere between the renal cortex and the urethral meatus. Because it is usually difficult to determine the exact location of the infection, the term UTI is used to explain microorganisms anywhere within the urinary tract. UTIs are categorized as cystitis or urethritis (located in the bladder or urethra), upper tract (located in the ureters or collecting system), and pyelonephritis (renal parenchyma). The greatest incidence of UTI in males occurs in the first year of life (most common in uncircumcized males), after which it rapidly declines, remaining low through childhood and adolescence. Incidence in females is also highest in the first year of life and steadily declines through adolescence, but remains higher than the incidence for males at a rate of 10:1.
Pathophysiology—inflammatory changes occur in the affected portions of the urinary tract, including kidneys, ureters, or bladder and urethra.
Clumps of bacteria may be present.
Inflammation results in urine retention and stasis of urine in the bladder.
Backflow of urine into the kidneys may occur through the ureters; this is called vesicoureteral reflux (VUR).
Inflammatory changes in the renal pelvis, and throughout the kidney, occur when the kidney is involved.
Scarring of the kidney parenchyma occurs in chronic infection and interferes with kidney function, particularly with the ability to concentrate urine.
If left untreated, the kidney may become small, tissue may be destroyed, and renal function could fail.
Clinical Manifestations
Onset may be abrupt or gradual; may be asymptomatic.
Failure to thrive in infancy.
Young children: may be nonspecific (vomiting, irritability, poor feeding, diarrhea); fever is often the only presenting complaint.
Older children and adolescents: urinary frequency, urgency or voiding hesitancy, dysuria, suprapubic tenderness, dribbling, and nocturnal enuresis (more common in lower UTI).
Hematuria: often occurs with viral cystitis.
Fever.
May be moderate or severe.
May fluctuate rapidly.
May be accompanied by chills or convulsions.
Anorexia and general malaise.
Foul odor or change in the appearance of urine.
Abdominal or suprapubic pain (more common in upper-tract disease).
Tenderness over one or both kidneys.
Systemic symptoms: flank pain, fever, chills, nausea, vomiting may occur with pyelonephritis.
Table 49-1 Antimicrobial Agents Commonly Used in the Management of Childhood Urinary Tract Infection
DRUG
ADVERSE EFFECTS
NURSING CONSIDERATIONS
Amoxicillin
Occasional nausea, vomiting, diarrhea
Hypersensitivity reactions of skin
Readily absorbed.
May be taken with food.
Ampicillin
Diarrhea, urticaria
Anaphylactic reaction
Contraindicated in penicillin-sensitive children. Package insert should be consulted regarding reconstitution, administration, and storage of I.M. and IV preparations. Absorption of oral preparations may be decreased with food. Dose must be repeated q6h to ensure therapeutic blood levels.
Cephalexin
Diarrhea, nausea, vomiting
May be taken with food. Dose should be reduced if renal function is impaired.
Gentamicin
Renal and auditory toxicity; respiratory paralysis
Toxic effects can be minimized by slow IV infusion (over 1 hour).
Nitrofurantoin
Fever, nausea, vomiting, peripheral neuropathy
Recommended for prolonged use. Give with food or milk to decrease GI adverse effects. May cause urine to be amber or brown in color. Contraindicated in renal failure and in infants younger than 3 months old.
Co-trimoxazole
Nausea, vomiting, fever, rash, photosensitivity
Commonly used if bacterial resistance is anticipated or the child fails to respond to initial therapy.
Diagnostic Evaluation
Urine culture:
Documentation of pathogenic organisms in the urine is the only means of definitive diagnosis.
A urine culture demonstrating more than 100,000 bacteria per mL indicates significant bacteriuria.
A catheterized urine specimen, with growth greater than 10,000 colonies of bacteria per mL, is considered significant.
Urinalysis:
Leukocytes, nitrites suggestive but not indicative.
Casts, especially WBC casts, may be present and are indicative of intrarenal infection.
Hematuria—occurs occasionally.
Decreased specific gravity due to decreased renal concentrating ability.
Urologic and radiologic studies to identify anatomic abnormalities or renal changes that stem from recurrent infections—renal ultrasound, voiding cystourethrogram (VCUG).
Dimercaptosuccinic acid scan—evaluates renal function and scarring.
 Evidence Base
Evidence Base NURSING ALERT
NURSING ALERT DRUG ALERT
DRUG ALERT Evidence Base
Evidence Base



