Palliative and Hospice Care
Health care professionals are generally not as comfortable dealing with issues related to death and dying as they are with supporting the patient through curative treatment. Knowledge and skill in providing physical and emotional comfort to dying patients and their families is essential to providing optimum care to persons with advanced, progressive diseases. Palliative care is a relatively new specialty that focuses on promoting the best possible quality of life for patients facing serious life-threatening illness through optimal management of physical, psychosocial, emotional, and spiritual symptoms. This specialty grew out of the hospice movement and is continuing to evolve as more palliative care teams are integrated into health care systems, more palliative care content is taught in schools of medicine and nursing, and more research is conducted to support an evidence base for palliative interventions.
DEFINITION
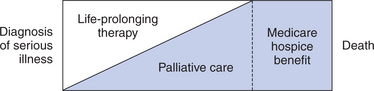
Palliative care can and should be initiated at the diagnosis of a serious life-threatening or chronic, progressive illness and continued throughout the course of the illness across all care settings. As illustrated in the figure on page 438, palliative care is started along with life-prolonging therapies at the initial diagnosis of a life-threatening illness. As the disease progresses, there is a greater and greater emphasis on palliative interventions versus life-prolonging interventions. Hospice care is the part of the palliative care continuum when the emphasis is no longer on life prolongation, but primarily on comfort. In the United States, this is often defined as the last 6 months of life and is based on the eligibility requirements for hospice benefits under Medicare.
• The interdisciplinary approach
• Focus on physical, psychosocial, emotional, and spiritual symptoms
See the box on page 438 for a summary of the practice guidelines outlined by the NCPQCP.
PALLIATIVE CARE IN PERSONS WITH CANCER
In general, the following patient populations are appropriate for palliative care:
• Persons diagnosed with large, poorly differentiated tumors
• Persons with distant metastasis at the time of diagnosis
• Persons whose diseases progress while on treatment or with short progression-free intervals after completing a course of treatment have a worse prognosis.
• Persons with a declining functional status
• Persons with multiple symptoms or those with one or more symptoms that are difficult to manage. Common symptoms include pain, dyspnea, nausea, vomiting, anorexia, constipation, fatigue, anxiety, and confusion.
MODELS OF PALLIATIVE CARE DELIVERY
• Consultation service team, consisting of physician, nurse, or social work evaluations
• Dedicated inpatient unit in an acute or rehabilitation hospital, nursing home, or free-standing inpatient hospice
• Hospital- or private practice–based outpatient palliative care practice or clinic
• Hospice-based palliative care at home
HOSPICE PALLIATIVE CARE
The figure on page 438 illustrates that hospice care is the part of the palliative care continuum when life-prolonging therapies are no longer providing benefit. The focus of care is on comfort and quality of living by affirming life and viewing dying as a normal process. Services provided by the hospice interdisciplinary team include pain and symptom management, psychosocial and spiritual support, assistance and support with direct caregiving, and bereavement care for both the patient and family. The practice guidelines outlined by the NCPQPC (see box on right) also apply to the organized, comprehensive services available through hospice programs.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


