http://evolve.elsevier.com/Wong/clinical • The Child with Sickle Cell Disease • The Child with Elevated Body Temperature • The High-Risk Infant with Respiratory Distress Syndrome (RDS) • The Infant with Bronchiolitis and Respiratory Syncytial Virus (RSV) Infection • The Child with Diabetic Ketoacidosis (DKA) • The Adolescent with an Eating Disorder • The Child with Growth Failure (cause unspecified) • The Child Undergoing Surgery • The Child with Cerebral Palsy • The infant with Bronchopulmonary Dysplasia (BPD) • The Child with Cystic Fibrosis • The Infant with Gastrointestinal Dysfunction, Obstructive • The Child with Cleft Lip and/or Cleft Palate (CL/CP) • The Infant with Esophageal Atresia and Tracheoesophageal Fistula • The Child with Tonsillectomy or Myringotomy • The Child with Rheumatic Fever (RF) • The Child with Myelomeningocele • The Child with Idiopathic Scoliosis 1. Assessment—The analysis and synthesis of data obtained from a comprehensive and focused health history and physical examination of the child and family 2. Problem identification or diagnosis—The determination of actual or potential health problems stated as a nursing diagnosis 3. Plan formulation—A set of nursing interventions planned to prioritize the health care needs of the child and family. Patient-centered outcomes may be formulated in this phase. 4. Implementation—The performance or execution of the plan 5. Evaluation—A measure of the outcome of nursing action(s) that either completes the nursing process or serves as a basis for reassessment The American Nurses Association has established Standards of Practice (use of the nursing process): 1. Assessment—The nurse collects comprehensive data pertinent to the patient’s health or the situation. 2. Diagnosis—The nurse analyzes assessment data to determine the diagnoses or issues. 3. Outcomes identification—The nurse identifies expected outcomes for a plan individualized to the patient or the situation. 4. Planning—The nurse develops a plan of care that prescribes strategies and alternatives to attain expected outcomes. 5. Implementation—The nurse implements the identified plan. 6. Evaluation—The nurse evaluates progress toward attainment of outcomes.* The North American Nursing Diagnosis Associations-International† defines nursing diagnosis as a clinical judgment about individual, family, or community responses to actual and potential health problems. The nursing diagnoses used in this manual are taken from the North American Nursing Diagnosis Association-International (Box 5-1). Nursing diagnoses are suggested for select health system dysfunctions. Included is the Nursing Intervention Classification (NIC) for each nursing diagnosis. The NIC is a standardized list of evidence-based nursing care interventions. In addition, the Nursing Outcomes Classification (NOC) is included to provide standardized patient outcomes. The selected nursing diagnoses and care interventions serve as general guides for the nursing care of children and families. Other nursing diagnoses and care interventions should be added to individualize care as appropriate. Nursing Care Plan The Child in Pain • Physiologic changes: Increased heart rate and blood pressure, increased respirations, crying, sweating, decreased oxygen saturation, dilation of pupils, flushing or pallor, nausea, muscle tension in the early onset of acute pain that subsides in continuing and chronic pain, making these symptoms unreliable indicators of persistent acute and chronic pain Nursing Care Plan The Newborn with Jaundice • Skin jaundice evident within 24 hours of birth • Altered breast-feeding (ineffective latch-on, nurses less than 6 to 8 times in a 24-hour period) • Altered stooling pattern (less than one stool in 24 hours) in first 3 days of life • Total serum bilirubin in high intermediate of high-risk zone on hour-specific nomogram in first 48 to 72 hours of life Nursing Care Plan The Child with Acute Respiratory Infection • Use of accessory muscles to breathe • Assumption of three-point position (tripod) • Respiratory rate is outside normal parameter for child’s age (increased or decreased rate)
Nursing Care Plans

The Process of Nursing Infants and Children
Nursing Diagnoses and the Nursing Process
Nursing Care of Common Problems of Ill and Hospitalized Children
Nursing Diagnosis
Expected Patient Outcomes
Nursing Interventions
Rationale
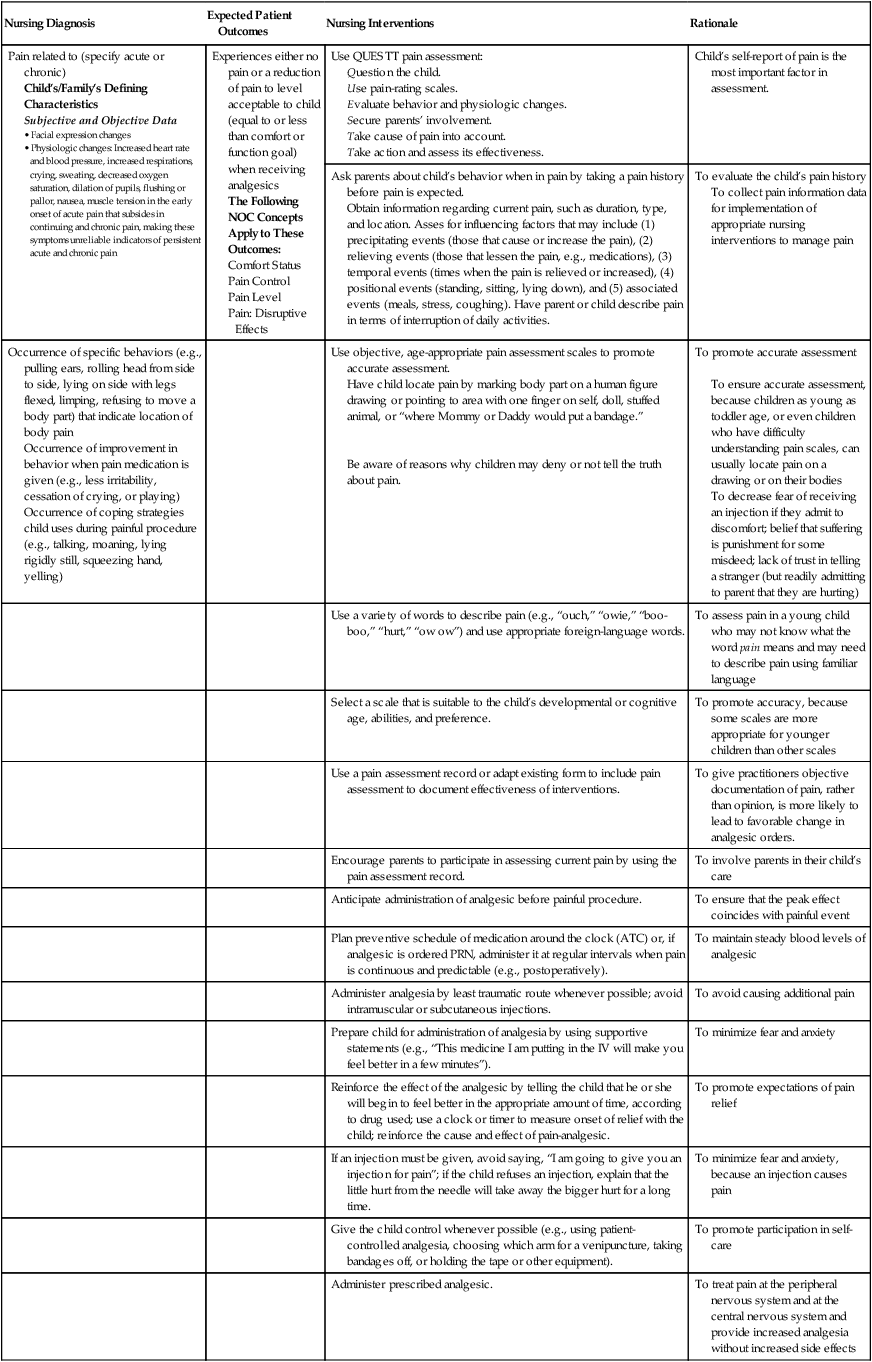
Pain related to (specify acute or chronic)
Child’s/Family’s Defining Characteristics
Subjective and Objective Data
Experiences either no pain or a reduction of pain to level acceptable to child (equal to or less than comfort or function goal) when receiving analgesics
The Following NOC Concepts Apply to These Outcomes:
Use QUESTT pain assessment:
Question the child.
Use pain-rating scales.
Evaluate behavior and physiologic changes.
Secure parents’ involvement.
Take cause of pain into account.
Take action and assess its effectiveness.
Child’s self-report of pain is the most important factor in assessment.
Ask parents about child’s behavior when in pain by taking a pain history before pain is expected.
Obtain information regarding current pain, such as duration, type, and location. Asses for influencing factors that may include (1) precipitating events (those that cause or increase the pain), (2) relieving events (those that lessen the pain, e.g., medications), (3) temporal events (times when the pain is relieved or increased), (4) positional events (standing, sitting, lying down), and (5) associated events (meals, stress, coughing). Have parent or child describe pain in terms of interruption of daily activities.
To evaluate the child’s pain history
To collect pain information data for implementation of appropriate nursing interventions to manage pain
Occurrence of specific behaviors (e.g., pulling ears, rolling head from side to side, lying on side with legs flexed, limping, refusing to move a body part) that indicate location of body pain
Occurrence of improvement in behavior when pain medication is given (e.g., less irritability, cessation of crying, or playing)
Occurrence of coping strategies child uses during painful procedure (e.g., talking, moaning, lying rigidly still, squeezing hand, yelling)
Use objective, age-appropriate pain assessment scales to promote accurate assessment.
Have child locate pain by marking body part on a human figure drawing or pointing to area with one finger on self, doll, stuffed animal, or “where Mommy or Daddy would put a bandage.”
Be aware of reasons why children may deny or not tell the truth about pain.
To promote accurate assessment
To ensure accurate assessment, because children as young as toddler age, or even children who have difficulty understanding pain scales, can usually locate pain on a drawing or on their bodies
To decrease fear of receiving an injection if they admit to discomfort; belief that suffering is punishment for some misdeed; lack of trust in telling a stranger (but readily admitting to parent that they are hurting)
Use a variety of words to describe pain (e.g., “ouch,” “owie,” “boo-boo,” “hurt,” “ow ow”) and use appropriate foreign-language words.
To assess pain in a young child who may not know what the word pain means and may need to describe pain using familiar language
Select a scale that is suitable to the child’s developmental or cognitive age, abilities, and preference.
To promote accuracy, because some scales are more appropriate for younger children than other scales
Use a pain assessment record or adapt existing form to include pain assessment to document effectiveness of interventions.
To give practitioners objective documentation of pain, rather than opinion, is more likely to lead to favorable change in analgesic orders.
Encourage parents to participate in assessing current pain by using the pain assessment record.
To involve parents in their child’s care
Anticipate administration of analgesic before painful procedure.
To ensure that the peak effect coincides with painful event
Plan preventive schedule of medication around the clock (ATC) or, if analgesic is ordered PRN, administer it at regular intervals when pain is continuous and predictable (e.g., postoperatively).
To maintain steady blood levels of analgesic
Administer analgesia by least traumatic route whenever possible; avoid intramuscular or subcutaneous injections.
To avoid causing additional pain
Prepare child for administration of analgesia by using supportive statements (e.g., “This medicine I am putting in the IV will make you feel better in a few minutes”).
To minimize fear and anxiety
Reinforce the effect of the analgesic by telling the child that he or she will begin to feel better in the appropriate amount of time, according to drug used; use a clock or timer to measure onset of relief with the child; reinforce the cause and effect of pain-analgesic.
To promote expectations of pain relief
If an injection must be given, avoid saying, “I am going to give you an injection for pain”; if the child refuses an injection, explain that the little hurt from the needle will take away the bigger hurt for a long time.
To minimize fear and anxiety, because an injection causes pain
Give the child control whenever possible (e.g., using patient-controlled analgesia, choosing which arm for a venipuncture, taking bandages off, or holding the tape or other equipment).
To promote participation in self-care
Administer prescribed analgesic.
To treat pain at the peripheral nervous system and at the central nervous system and provide increased analgesia without increased side effects
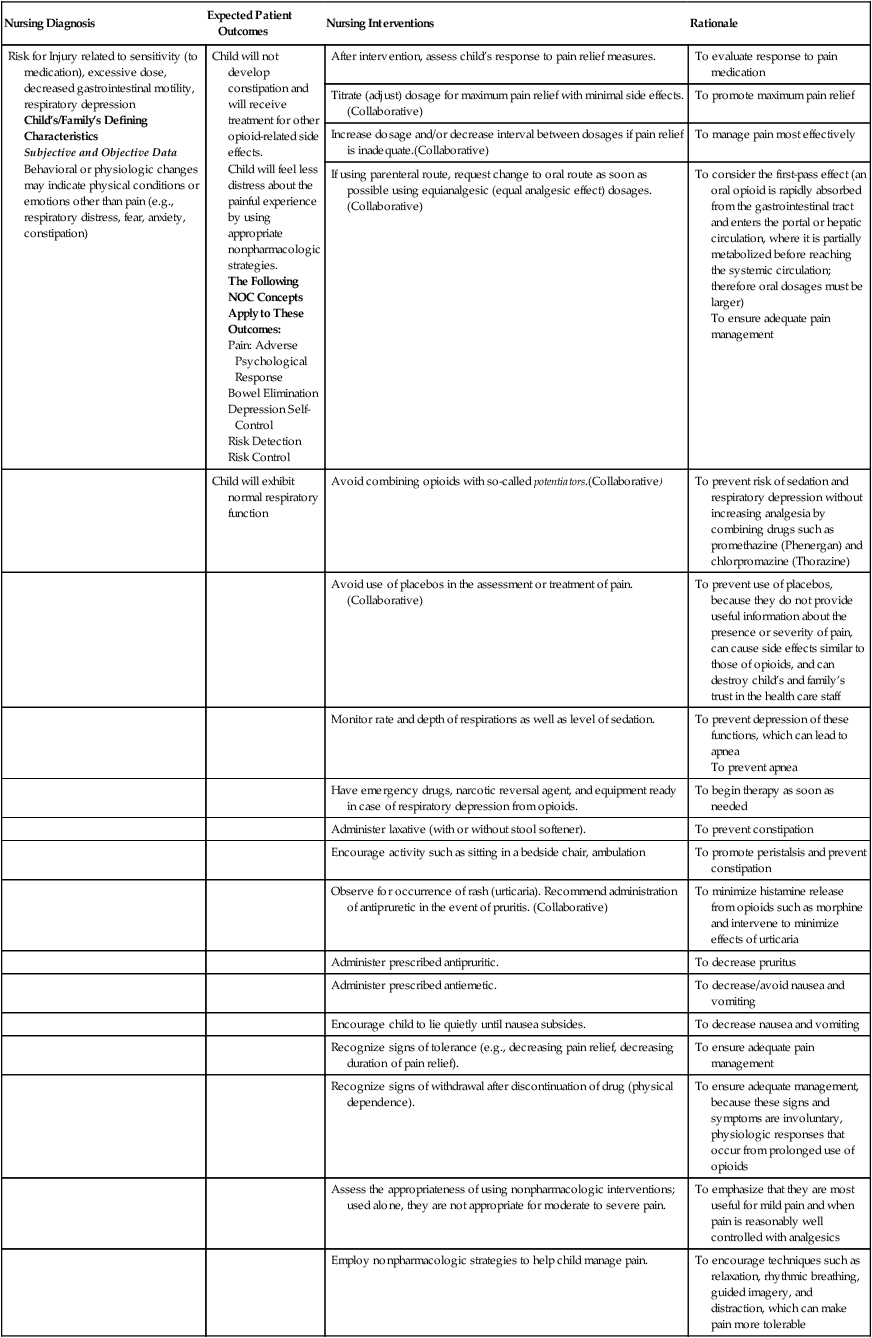
Risk for Injury related to sensitivity (to medication), excessive dose, decreased gastrointestinal motility, respiratory depression
Child’s/Family’s Defining Characteristics
Subjective and Objective Data
Behavioral or physiologic changes may indicate physical conditions or emotions other than pain (e.g., respiratory distress, fear, anxiety, constipation)
Child will not develop constipation and will receive treatment for other opioid-related side effects.
Child will feel less distress about the painful experience by using appropriate nonpharmacologic strategies.
The Following NOC Concepts Apply to These Outcomes:
After intervention, assess child’s response to pain relief measures.
To evaluate response to pain medication
Titrate (adjust) dosage for maximum pain relief with minimal side effects.(Collaborative)
To promote maximum pain relief
Increase dosage and/or decrease interval between dosages if pain relief is inadequate.(Collaborative)
To manage pain most effectively
If using parenteral route, request change to oral route as soon as possible using equianalgesic (equal analgesic effect) dosages. (Collaborative)
To consider the first-pass effect (an oral opioid is rapidly absorbed from the gastrointestinal tract and enters the portal or hepatic circulation, where it is partially metabolized before reaching the systemic circulation; therefore oral dosages must be larger)
To ensure adequate pain management
Child will exhibit normal respiratory function
Avoid combining opioids with so-called potentiators.(Collaborative)
To prevent risk of sedation and respiratory depression without increasing analgesia by combining drugs such as promethazine (Phenergan) and chlorpromazine (Thorazine)
Avoid use of placebos in the assessment or treatment of pain. (Collaborative)
To prevent use of placebos, because they do not provide useful information about the presence or severity of pain, can cause side effects similar to those of opioids, and can destroy child’s and family’s trust in the health care staff
Monitor rate and depth of respirations as well as level of sedation.
To prevent depression of these functions, which can lead to apnea
To prevent apnea
Have emergency drugs, narcotic reversal agent, and equipment ready in case of respiratory depression from opioids.
To begin therapy as soon as needed
Administer laxative (with or without stool softener).
To prevent constipation
Encourage activity such as sitting in a bedside chair, ambulation
To promote peristalsis and prevent constipation
Observe for occurrence of rash (urticaria). Recommend administration of antipruretic in the event of pruritis. (Collaborative)
To minimize histamine release from opioids such as morphine and intervene to minimize effects of urticaria
Administer prescribed antipruritic.
To decrease pruritus
Administer prescribed antiemetic.
To decrease/avoid nausea and vomiting
Encourage child to lie quietly until nausea subsides.
To decrease nausea and vomiting
Recognize signs of tolerance (e.g., decreasing pain relief, decreasing duration of pain relief).
To ensure adequate pain management
Recognize signs of withdrawal after discontinuation of drug (physical dependence).
To ensure adequate management, because these signs and symptoms are involuntary, physiologic responses that occur from prolonged use of opioids
Assess the appropriateness of using nonpharmacologic interventions; used alone, they are not appropriate for moderate to severe pain.
To emphasize that they are most useful for mild pain and when pain is reasonably well controlled with analgesics
Employ nonpharmacologic strategies to help child manage pain.
To encourage techniques such as relaxation, rhythmic breathing, guided imagery, and distraction, which can make pain more tolerable
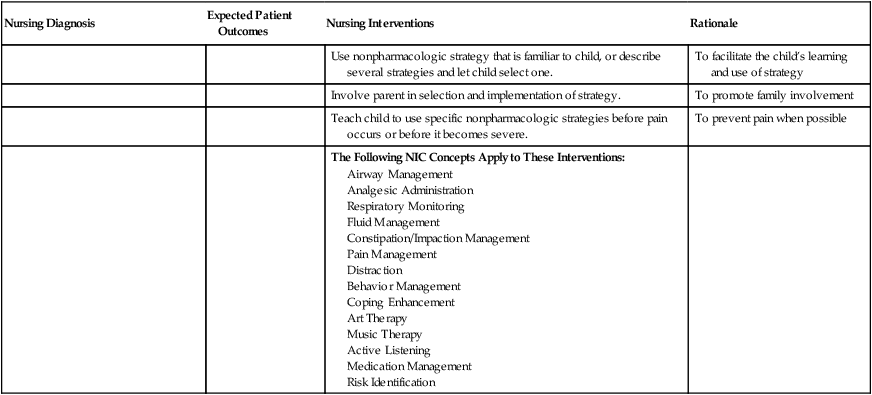
Use nonpharmacologic strategy that is familiar to child, or describe several strategies and let child select one.
To facilitate the child’s learning and use of strategy
Involve parent in selection and implementation of strategy.
To promote family involvement
Teach child to use specific nonpharmacologic strategies before pain occurs or before it becomes severe.
To prevent pain when possible
The Following NIC Concepts Apply to These Interventions:
Nursing Care of the Newborn
Nursing Diagnosis
Expected Patient Outcomes
Nursing Interventions
Rationale
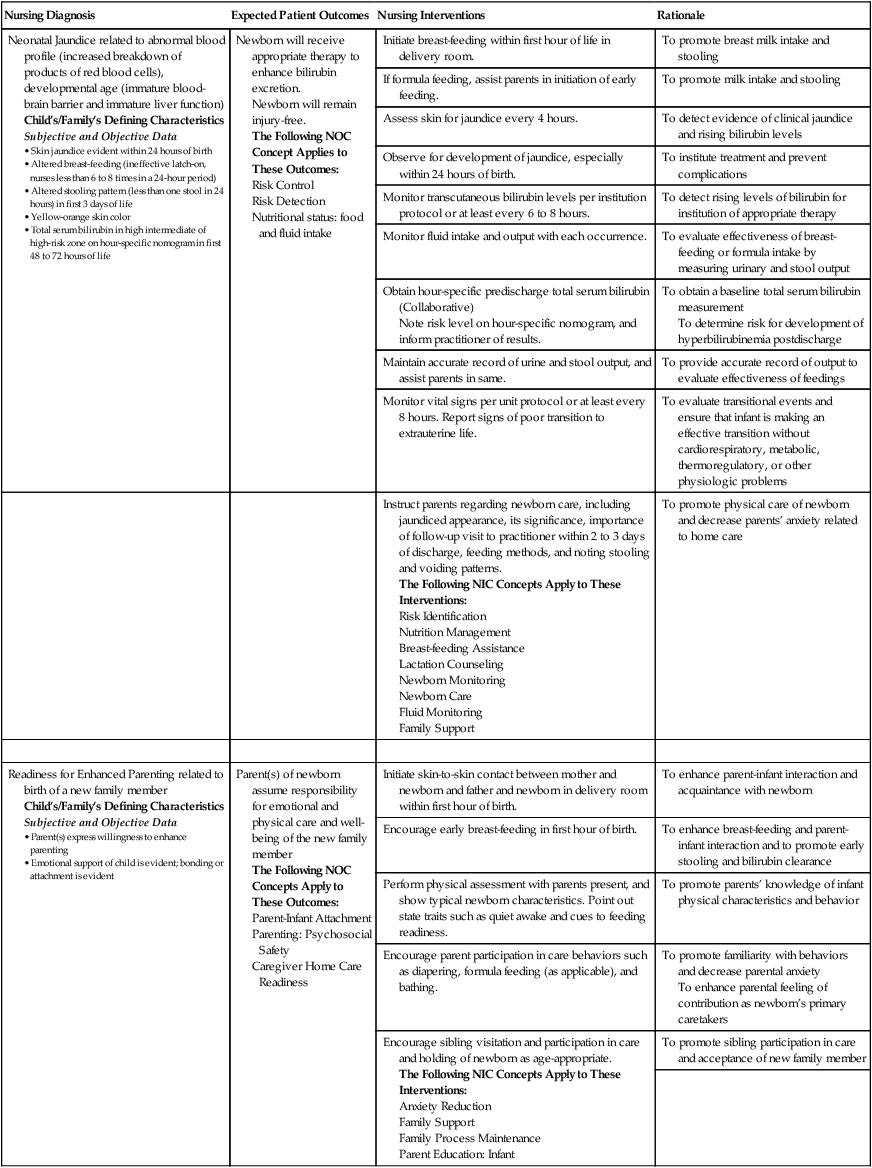
Neonatal Jaundice related to abnormal blood profile (increased breakdown of products of red blood cells), developmental age (immature blood-brain barrier and immature liver function)
Child’s/Family’s Defining Characteristics
Subjective and Objective Data
Newborn will receive appropriate therapy to enhance bilirubin excretion.
Newborn will remain injury-free.
The Following NOC Concept Applies to These Outcomes:
Initiate breast-feeding within first hour of life in delivery room.
To promote breast milk intake and stooling
If formula feeding, assist parents in initiation of early feeding.
To promote milk intake and stooling
Assess skin for jaundice every 4 hours.
To detect evidence of clinical jaundice and rising bilirubin levels
Observe for development of jaundice, especially within 24 hours of birth.
To institute treatment and prevent complications
Monitor transcutaneous bilirubin levels per institution protocol or at least every 6 to 8 hours.
To detect rising levels of bilirubin for institution of appropriate therapy
Monitor fluid intake and output with each occurrence.
To evaluate effectiveness of breast-feeding or formula intake by measuring urinary and stool output
Obtain hour-specific predischarge total serum bilirubin (Collaborative)
Note risk level on hour-specific nomogram, and inform practitioner of results.
To obtain a baseline total serum bilirubin measurement
To determine risk for development of hyperbilirubinemia postdischarge
Maintain accurate record of urine and stool output, and assist parents in same.
To provide accurate record of output to evaluate effectiveness of feedings
Monitor vital signs per unit protocol or at least every 8 hours. Report signs of poor transition to extrauterine life.
To evaluate transitional events and ensure that infant is making an effective transition without cardiorespiratory, metabolic, thermoregulatory, or other physiologic problems
Instruct parents regarding newborn care, including jaundiced appearance, its significance, importance of follow-up visit to practitioner within 2 to 3 days of discharge, feeding methods, and noting stooling and voiding patterns.
The Following NIC Concepts Apply to These Interventions:
To promote physical care of newborn and decrease parents’ anxiety related to home care
Readiness for Enhanced Parenting related to birth of a new family member
Child’s/Family’s Defining Characteristics
Subjective and Objective Data
Parent(s) of newborn assume responsibility for emotional and physical care and well-being of the new family member
The Following NOC Concepts Apply to These Outcomes:
Initiate skin-to-skin contact between mother and newborn and father and newborn in delivery room within first hour of birth.
To enhance parent-infant interaction and acquaintance with newborn
Encourage early breast-feeding in first hour of birth.
To enhance breast-feeding and parent-infant interaction and to promote early stooling and bilirubin clearance
Perform physical assessment with parents present, and show typical newborn characteristics. Point out state traits such as quiet awake and cues to feeding readiness.
To promote parents’ knowledge of infant physical characteristics and behavior
Encourage parent participation in care behaviors such as diapering, formula feeding (as applicable), and bathing.
To promote familiarity with behaviors and decrease parental anxiety
To enhance parental feeling of contribution as newborn’s primary caretakers
Encourage sibling visitation and participation in care and holding of newborn as age-appropriate.
The Following NIC Concepts Apply to These Interventions:
To promote sibling participation in care and acceptance of new family member
Nursing Care of the Child with Respiratory Dysfunction
Nursing Diagnosis
Expected Patient Outcomes
Nursing Interventions
Rationale
Ineffective Breathing Pattern related to inflammatory process
Child’s/Family’s Defining Characteristics
Subjective and Objective Data
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access
