Chapter 7 Normal labour and delivery
MYOMETRIAL ACTIVITY: PREGNANCY
Towards term a number of processes occur which predispose to activation or preparation of the myometrium for onset of labour. Formation of gap junctions by increases in contraction-associated proteins such as connexin-43 enhance cell to cell coupling. Receptors for oxytocin and stimulatory prostaglandins are also increased. These changes are associated with myometrial stretch when the uterus enlarges and with the higher levels of oestrogens derived partly from placental conversion of fetal dehydroepiandrosterone (DHEAS) where they also exert a local oestrogen effect. In addition to increased DHEAS production, activation of the fetal hypothalamic–pituitary–adrenal axis in late pregnancy results in more fetal cortisol biosynthesis. Fetal cortisol competes to reduce the local progesterone effect and stimulate synthesis of corticotrophin-releasing hormone from placenta and fetal membranes for production of prostaglandins by the latter structures.
MYOMETRIAL ACTIVITY: LABOUR
Uterine work
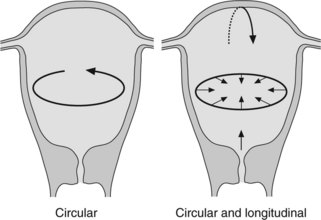
Myometrial contraction exerts a pull in circular and longitudinal directions (Figure 7.1)
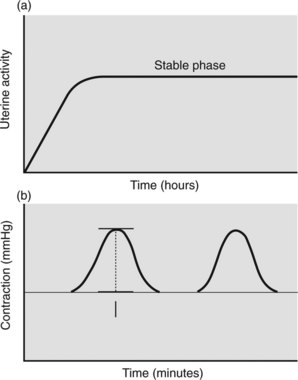
In early labour the uterus is not working at maximum capacity. This may be because the number of myometrial cells contracting is limited or contraction is poorly synchronised or of short duration. As labour progresses contractions becomes more efficient and uterine work increases. Capacity for work cannot, however, increase indefinitely. A stable phase for ability to work results once maximal work output is achieved for the individual mother. When the stable phase is achieved (Figure 7.2a) additional stimulation by oxytocics is of little value and can be harmful. Uterine work has been expressed as: