Chapter 41 NEUROLOGICAL HEALTH
THE FUNCTION AND STRUCTURE OF THE NEUROLOGICAL SYSTEM
NERVOUS TISSUE
Neurons
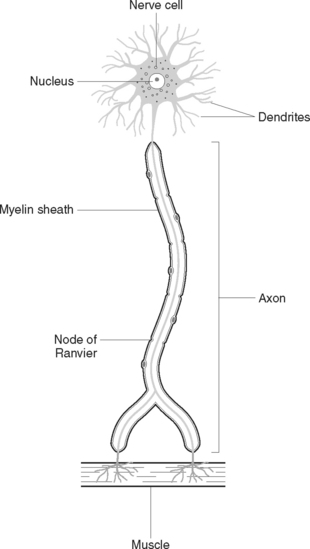
Neurons (Figure 41.1) are the primary components of the nervous system. Functioning alone, or as units, neurons detect internal and external changes and initiate body responses needed to maintain homeostasis. Each neuron is composed of a cell body, with projections forming dendrites, and one long axon. The dendrites are short-branched fibres, which receive impulses and conduct them towards the cell body of a neuron. The axon, which may vary in length from miniscule to over a metre, conducts impulses away from the cell body of a neuron. Generally, a neuron has only one axon but many dendrites. Axons leave the grey matter and become the fibres of the white matter. Each axon has a covering called a neurilemma, and most have a fatty sheath, the myelin sheath. The myelin sheath protects and insulates the axon and increases the transmission rate of nervous impulses. Neurons are bound together by a special type of connective tissue called neuroglia.
THE CENTRAL NERVOUS SYSTEM
The brain
The cerebrum
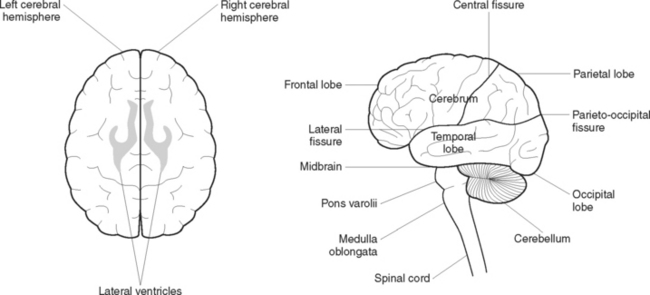
The cerebrum (Figure 41.2) is the largest part of the brain, filling the vault of the cranium from front to back. It is divided by fissures into the left and right hemispheres, and each hemisphere is further divided by fissures into four lobes:
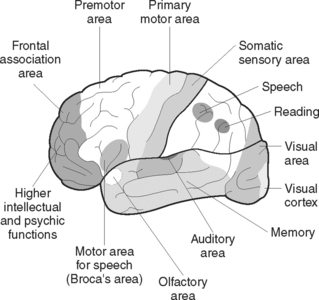
The cerebrum is divided into several areas, some of which are sensory and some of which are motor areas. The sensory areas of each hemisphere receive and interpret sensations from the opposite side of the body, including touch, temperature, pain, pressure and an awareness of the position of the body in its environment. The motor areas of each hemisphere control all voluntary movement on the opposite side of the body. The centres of special sense are located in the various lobes, including the centres for hearing, speech, smell, taste and sight (Figure 41.3).
The diencephalon
The thalami are two oval masses of grey matter that form the lateral walls of the third ventricle. Each thalamus is subdivided into a number of nuclei. Most sensory pathways (except smell) synapse here. The thalamus plays a role in the control of somatic motor activity and also influences mood and strong emotions.
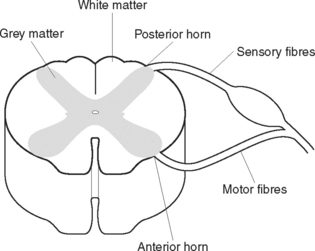
The spinal cord
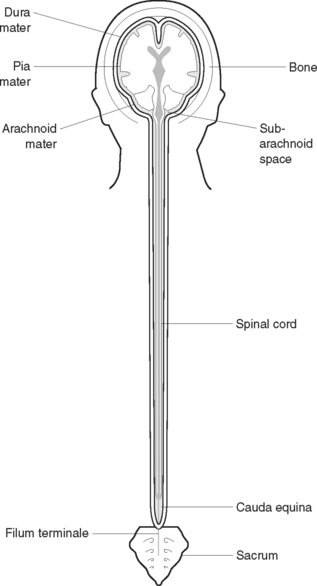
The spinal cord is a cylindrical structure that lies within a canal inside the vertebral column. It extends from an opening on the underside of the skull (the foramen magnum) to the level of the first or second lumbar vertebra. Below this level the vertebral canal is occupied by nerves from the lumbar and sacral segments of the cord; these constitute the cauda equina (‘horse’s tail’). The spinal cord, which is about 46 cm in length, consists of nervous tissue, with the white matter on the outside and the grey matter arranged roughly in an ‘H’ formation in the centre (Figures 41.4 and 41.5). The two anterior projections of grey matter are called the anterior horns, and the posterior projections are called the posterior horns. Sensory nerve fibres enter the posterior horns, and motor nerve fibres leave the anterior horns.
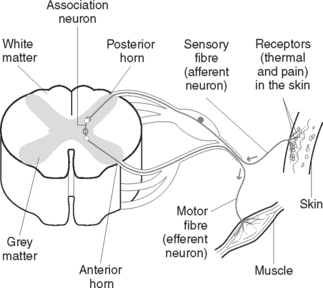
A reflex action, or arc, is an automatic motor response to a sensory stimulus without conscious involvement (Figure 41.6). Most reflex actions are protective in nature and take place more quickly than voluntary actions. The structures involved in a reflex action are:
The meninges
THE PERIPHERAL NERVOUS SYSTEM
The cranial nerves
THE AUTONOMIC NERVOUS SYSTEM
Functions of the autonomic nervous system
The parasympathetic nerves are called cholinergic fibres and release the neurotransmitter acetylcholine. These nerves tend to slow down body processes, so that the end result of the antagonistic action of each division of the autonomic nervous system is a balance between acceleration and retardation. After the ‘fright’ or stressful situation is over, the parasympathetic nervous system returns things to normal. The digestive organs receive more blood, the glands increase their secretions, the heartbeat is decreased and the blood pressure falls. The effects of sympathetic and parasympathetic stimulation on various body organs are compared in Table 41.1.
TABLE 41.1 EFFECTS OF SYMPATHETIC AND PARASYMPATHETIC STIMULATION
| Organ | Sympathetic stimulation | Parasympathetic stimulation |
|---|---|---|
| Heart | Increases rate/strength of heartbeat | Decreases rate/strength of heartbeat |
| Dilates coronary arteries to increase blood supply to the heart muscle | Constricts coronary arteries to decrease supply of blood to the heart muscle | |
| Bronchi | Dilates bronchi, allowing more air to enter the lungs | Constricts bronchi, limiting air intake |
| Digestive system | ||
| Urinary bladder | Relaxes bladder wall. Contracts internal sphincter muscle | Contracts bladder wall. Relaxes internal sphincter muscle |
| Eye | Dilates the pupil. Retracts the eyelids | Constricts the pupil. Closes the eyelids |
| Skin |
PATHOPHYSIOLOGICAL INFLUENCES AND EFFECTS OF DISORDERS OF THE NERVOUS SYSTEM
AETIOLOGY OF NERVOUS SYSTEM DISORDERS
Inflammatory and infectious conditions
Bacterial or viral infective processes affecting the central nervous system may result in the destruction of nervous tissue through the action of toxins released by the living microorganisms and from the material released from dead microorganisms, which stimulates the inflammatory process. Infection and inflammation of nervous tissue may result in altered behaviour, altered consciousness, and sensory or motor deficits.
Metabolic and endocrine disorders
Nervous system dysfunction may result from the effects of certain metabolic and endocrine disorders. Some nutritional deficiencies may affect nerve cells, resulting in their damage or death. For example, degeneration of the posterior and lateral columns of the spinal cord may occur from the vitamin B12 deficiency of pernicious anaemia. Disorders of cortical function, leading to confusion or coma, may result from a deficiency of thiamine (vitamin B1).
MAJOR MANIFESTATIONS OF NERVOUS SYSTEM DISORDERS
Motor changes
Symptoms of ataxia, a condition characterised by impaired ability to coordinate movement, may be caused by a lesion in the spinal cord or cerebellum. Dizziness or vertigo, when the individual is unable to maintain normal balance in a standing or seated position, may also be related to a disorder of the nervous system. Unusual gait or stance may result from motor or sensory deficits caused by a disorder of the nervous system, such as Parkinson’s disease. Paralysis, a symptom of motor disturbances, can occur in varying degrees with many nervous system disorders. Upper motor neuron lesions, in which the reflex area remains intact, generally cause spastic paralysis. Flaccid paralysis generally occurs in lower motor neuron lesions, which disrupt the reflex area.
SPECIFIC DISORDERS OF THE NERVOUS SYSTEM
CONGENITAL DISORDERS
Structural congenital abnormalities include anencephaly, spinal cord defects and hydrocephalus.
GENETIC DISORDERS
Hereditary genetic defects include muscular dystrophy, Huntington’s chorea and neurofibromatosis.
Muscular dystrophy
Muscular dystrophy is a group of congenital disorders characterised by progressive wasting and weakness of muscles. Duchenne muscular dystrophy, which begins to manifest between the ages of 3 and 5 years, is the most common and severe form. Initially it affects the leg and pelvic muscles but there is progressive involvement of all voluntary muscles. Later in the disease, progressive weakening of cardiac and respiratory muscles results in heart or respiratory failure. Early manifestations of Duchenne’s muscular dystrophy include a waddling gait, lordosis (increased curvature of the lumbar spine) and marked difficulty rising from a supine to a standing position. As the disease progresses, facial, oropharyngeal and respiratory muscles become involved.
DISORDERS OF MULTIPLE CAUSE
Intellectual disability
SEIZURE DISORDERS
Although seizures may result from a nervous system disorder, they may be caused by many other factors and are often idiopathic. The international classification of seizures is given in Table 41.2.
TABLE 41.2 THE INTERNATIONAL CLASSIFICATION OF SEIZURES
| I | Focal or partial seizures |
| Simple (general, without an impairment of level of consciousness): | |
| II | Generalised seizures (without a local onset, bilateral, symmetric) |
| III | Unilateral seizures |
| IV | Unclassified seizures (when complete data are not available) |
| V | Classification of paroxysmal forms |
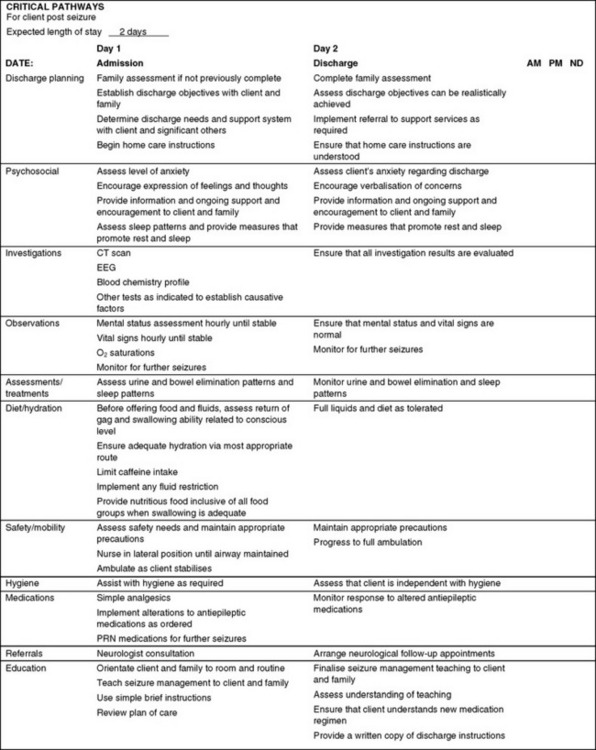
Figure 41.7 shows a sample nursing critical pathway for managing a client after a seizure, and Clinical Interest Box 41.1 provides an outline of teaching for home care of clients in relation to seizures.
CLINICAL INTEREST BOX 41.1 Teaching for home care of clients affected by generalised seizures
DEGENERATIVE DISORDERS
Parkinson’s disease
Manifestations of Parkinson’s disease are related to disturbances of movement: tremor, muscle rigidity and dyskinesia. The most common initial symptom is tremor; for example, ‘pill-rolling’ movements of the fingers, and to-and-fro head tremors. Tremors are aggravated by fatigue and stress, and decrease when the individual performs a purposeful activity or is asleep. The person experiences difficulty in initiating voluntary movement and loss of posture control, so that walking is with the body bent forwards. The gait consists of short shuffling steps that are slowly initiated. Facial expression becomes mask-like, and the voice is commonly high-pitched and monotone. The person’s intelligence is not affected.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


