basic anatomy and physiology of the musculoskeletal system
common diagnostic tests for musculoskeletal problems
orthopedic treatments and procedures
selected musculoskeletal disorders in the pediatric population.
Anatomy and physiology
The musculoskeletal system is one of the most complex systems within the body. The muscles and bones allow the body to move and function. If a problem occurs in the musculoskeletal system, mobility and general activities of daily living may be impaired.
Bones
The body’s form and function are supported by the skeletal system. The mature human skeleton is made up of 206 bones that are shaped according to their function. Newborn infants have over 300 bones, a number of which fuse together by the time a child is around 9 years old. The skeletal system:
enables movement of the body by supporting soft tissues
provides support and allows a person to stand erect
protects underlying organs
serves as a reservoir for storing such minerals as calcium and phosphorus
serves as a site for red blood cell formation.
The long and short of it
Long bones are found in the upper and lower extremities. They’re responsible for carrying the body’s weight and helping make ambulation possible. Short bones are found in the hands and feet and are shaped to provide strength in a compact area. Some bones, such as the ribs and sternum, are flat and thin; they provide structure. Other bones are large and irregularly shaped (for example, the pelvic bone).
Universal coverage
The composition of bone differs depending on the type of bone, but all are covered by a double layer of connective tissue, called the periosteum, which helps provide nourishment to the bone. In children, the periosteum is thick and vascular, so a child’s bone tends to heal faster than that of an adult with the same injury.
Bone growth and formation
The epiphysis is the growth end of the long bones. The epiphyseal plate, or growth plate, is located in the epiphysis.
A plate of cartilage
The epiphyseal plate is composed of cartilage cells that grow and develop, thereby causing the bone to lengthen. The growth plate is gradually replaced by bone until only the epiphyseal line remains. When the plate is completely replaced by bone, the bones can no longer lengthen; they can only increase in breadth. Injury to the growth plate may seriously impede bone growth. Children are particularly susceptible to growth plate injuries.
Cartilage serves as a smooth surface for articulating bones. Because young children have a more cartilaginous skeleton, they may be less prone to severe fractures than adults.
Salty framework
Ossification is the process of developing new bones from tissue. Osteoblasts form bone cells that lay down a framework for the new bone. Calcium and phosphorus combine to form salts, which are then deposited into the framework. The thyroid and parathyroid glands regulate this deposition. (See Bone growth and remodeling.)
Bone bank deposit
To maintain equilibrium, bone is deposited where it’s needed within the skeletal system. If increased stress is placed on a certain bone, more bone is deposited. If there’s no stress on the bone, part of the bone mass is reabsorbed.
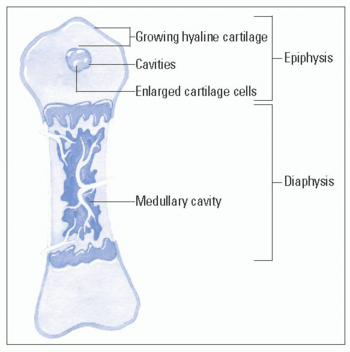
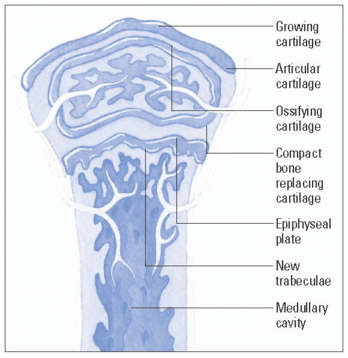
Bone growth and remodeling
The ossification of cartilage into bone, or osteogenesis, begins at about week 9 of fetal development. The diaphyses (shaft) of long bones are formed by birth, and the epiphyses (growth end) begin to ossify around that time. The stages of growth and remodeling of the epiphyses of a long bone are shown in these illustrations.
Creation of an ossification center
At about the ninth month of fetal development, an ossification center develops in the epiphysis. Some cartilage cells enlarge and stimulate ossification of surrounding cells. The enlarged cells die, leaving small cavities. New cartilage continues to develop.
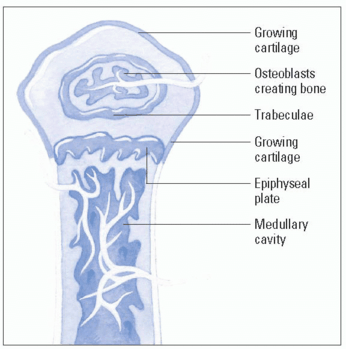
Osteoblasts form bone
Osteoblasts (bone-forming cells) begin to form bone on the remaining cartilage, creating the scaffolding or trabeculae network of cancellous (spongy) bone. Cartilage continues to form on the outer surfaces of the epiphysis and along the upper surface of the epiphyseal plate.
Bone growth
Cartilage is replaced by compact bone near the outer surfaces of the epiphysis. Only cartilage cells on the upper surface of the diaphyseal plate continue to multiply rapidly, pushing the epiphysis away from the diaphysis. This new cartilage ossifies, creating trabeculae on the inner or medullary side of the epiphyseal plate.
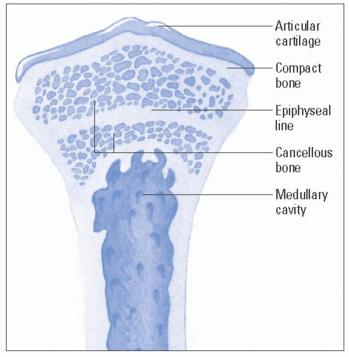
Remodeling
Osteoclasts (cells associated with bone resorption) produce enzymes and acids that reduce trabeculae created by the epiphyseal plate, thus enlarging the medullary (bone marrow) cavity. In the epiphysis, osteoclasts reduce bone, making its calcium available for new osteoblasts that give the epiphysis its adult shape and proportion. In young adults, the epiphyseal plate completely ossifies (closes) and becomes the epiphyseal line; longitudinal growth of bone then ceases.
Resorption is the process by which old bone is dissolved. The bone cells known as osteocytes and osteoclasts are responsible for the resorption of bone in this framework. This process can release calcium into the circulation.
Muscles
Muscles are the major organs that enable movement. They’re fibrous bundles covered with thin connective tissue. They also serve as repositories for some metabolites. Muscles are attached at each end directly to the bone or to a tendon, ligament, or fascia:
Tendons hold muscles to bones and are formed by strong, nonelastic collagen cords.
Ligaments hold bones to other bones; they encircle the joints and add strength and stability.
The fascia is a fibrous membrane of supporting, connective tissue.
Muscles in opposition
The movement enabled by muscles occurs through the contracting and lengthening of opposing muscle groups. As a muscle shortens on contraction, it pulls the bones to which it’s attached, bringing the bones closer together. Most muscles are attached to two bones that articulate (join or work together as a single unit) at an intervening joint.
Taking turns
For the most part, movement happens when one bone moves while the other is held stable. The body of the muscle that produces movement of the extremity usually lies proximal (closest) to the bone that’s moved.
Six hundred volunteers
There are more than 600 voluntary muscles (muscles we control) in the body. These muscles are called striated or skeletal muscles. Other types of muscles include visceral muscles (also called smooth or involuntary muscles) and the cardiac muscle.
Joints
Joints are formed when two surfaces of bones come together and articulate.
Joints on the move
There are three types of joints, classified by the degree of movement:
Synarthrodial (immovable) joints separate bone by a thin layer of cartilage—for example, the skull and various bones of the cranium.
Amphidiarthrodial (semimovable) joints separate bone with cartilage or a fibrocartilaginous disk—for example, the joints between the vertebral bodies.
Diarthrodial (freely movable) joints are commonly called synovial joints. Most joints in the body are synovial joints. They’re lined with a membrane that secretes and lubricates the joint with synovial fluid—for example, the knees, shoulders, and hips. They’re encased by the joint capsule, which is strengthened by ligaments that surround the capsule.
Flex or extend
Muscles are categorized according to the type of joint movement produced when the muscle is contracted. They’re designated as flexor or extensor muscles depending on whether the joint is flexed or extended. Range of motion (ROM) is determined by the degree of movement in a joint. (See Types of joint movement, page 418.)
Diagnostic tests
Tests used to assess the musculoskeletal system and guide treatment include arthroscopy, bone scans, electromyography (EMG), muscle and bone marrow biopsy, and X-rays.
Types of joint movement
There are seven types of joint movement:
Flexion is a bending forward of the joint; this decreases the angle between the bones that are connected.
Extension is an increase of the joint angle that occurs with straightening of the limb.
Abduction is the movement of the limb away from the midline, or central axis, of the body
Adduction is the movement of the limb toward or beyond the midline, or central axis, of the body.
Internal rotation is the turning of the body part inward, toward the midline, or central axis, of the body.
External rotation is the turning of the body part away from the midline, or central axis, of the body.
Circumduction is the movement of the body part in a circular motion.
Arthroscopy
Arthroscopy is a surgical procedure used to visualize, diagnose, and treat problems inside a joint. It involves placing a fiberoptic instrument into the joint and then visualizing the area. Corrective surgery can be done at the same time, which helps eliminate the need for more extensive surgery.
The knee is the most common joint evaluated and treated with arthroscopy. It’s most commonly done under a general anesthetic with younger children but can also be performed with a local or spinal anesthetic depending on the joint and the suspected problem.
Lean on me
There may be some swelling and pain after arthroscopy. With knee arthroscopy, the child may need to use crutches for 2 to 4 weeks after a surgical repair. It’s important for the crutches to be the right size for the child and for the child to be instructed in their use. This instruction is best given by someone from the physical therapy (PT) department. The child can usually return to school within a few days.
Nursing considerations
Prepare the child for the procedure by explaining the general anesthesia or the anesthetic, what the child will experience in the operating room (if he’ll be awake), and how he’ll feel after the procedure. In addition, follow these steps:
Note any allergies because of the anesthesia use.
Tell the child he may feel a thumping sensation as the cannula is inserted into the joint capsule (if he’ll be awake during the procedure).
Cover the site with a small dressing after the procedure.
Bone scans
Bone scans are used to diagnose osteomyelitis and metastatic bone disease. They can also be used to aid diagnosis of joint infections and certain fractures. Special radiographic techniques can help diagnose a musculoskeletal problem. These techniques include computed tomography (CT) scans and magnetic resonance imaging (MRI).
Nursing considerations
The tubelike structures that house the imaging equipment can be frightening to a child. Whenever possible, show the child a picture of the scanning equipment, or the equipment itself, before the procedure. Reassure the child that the parent will be allowed to remain in the room.
Explain the procedure to the parents and child. Tell the child that he’ll be placed in a tube so that pictures may be taken.
Instruct the child to remain still during the procedure; sedation may be necessary. Distraction techniques may help calm the child.
Remove metallic objects.
Electromyography
EMG measures muscle response to nervous stimulation (the electrical activity within the muscle fibers). Needle electrodes are inserted into the muscle to be tested, and electrical activity is recorded when the muscle is at rest and during contraction.
A sign of weakness
EMG is used when there are symptoms of muscle weakness and decreased muscle strength. It can differentiate primary muscle conditions from weakness caused by neurologic disorders or a lack of use of the particular muscle. Conditions that may be diagnosed by EMG include muscular dystrophy, nerve dysfunction, and Guillain-Barré syndrome.
Nursing considerations
EMG can be frightening and uncomfortable for a child. When explaining the procedure to the child and parents, prepare the child for insertion of the needle and the feeling in the muscle when the electrical impulses are sent through (like a hard hit to the “funny bone”). Let them know that residual bruising may occur.
In addition, follow these steps:
Explain that the child may be asked to voluntarily contract the muscle; help him practice the different positions or movements.
Use deep breathing exercises and play preparation to help lessen the fear and anxiety the child may experience. Involving a child life specialist may be helpful.
Reassure the child that his parent may stay with him during the procedure.
Muscle and bone marrow biopsy
Biopsy of the muscles and bones involves the removal of a small specimen of muscle or bone marrow for analysis. It’s usually performed at the bedside and takes about 20 minutes. Local anesthetics or systemic analgesics are used to help alleviate the pain. The puncture site may remain tender for a few weeks. For bone marrow biopsy, the proximal tibia is the most commonly used site in young children. In older children, the vertebral bodies T10 through L4 are preferred.
Nursing considerations
Biopsy can be an extremely frightening procedure for a child (and his parents). Thoroughly prepare the child and his parents. Allowing the child to “perform” the procedure on a doll (using correct positioning, a syringe, and a bandage) will enhance his understanding of the procedure and may help to ease his fears.
In addition, follow these steps:
Clarify the meaning of biopsy in context; many parents (and older children) automatically think of cancer when they hear the word biopsy.
Provide analgesics as ordered.
Assist the child into the desired position depending on the site to be used. If necessary, assist in holding the child still during the procedure. (Allow a parent to be present in a comforting capacity only, leaving the positioning and restraint of the child to the health care professionals.)
When the specimen is obtained, apply direct pressure to the site for 5 to 10 minutes.
Cover the site and make sure the child remains still for approximately 30 minutes after the procedure.
X-rays
Radiography is the most widely used diagnostic test in the assessment of children with bone abnormalities or other conditions affecting the bones. X-rays can show pathology, such as a fracture, and can show bone density and irregularities. X-rays are used not only for initial evaluation but also for monitoring and evaluating the effectiveness of treatment.
Invisible bone
Normally, the calcium deposits in bones will make skeletal structures appear radiopaque, or white, on X-rays. However, in the infant and young child (whose skeleton is composed mostly of growth cartilage), structures are radiolucent and may not appear on X-ray. Thus, X-rays are less reliable in this population. High-resolution ultrasound may provide a more accurate picture.
Nursing considerations
Always explain to the child the reason for obtaining an X-ray. Explain that an X-ray simply takes pictures (of whatever part of the body is being X-rayed). Reassure the child that the X-ray itself doesn’t hurt, but keep in mind that a child with an injury may experience discomfort during positioning for the X-ray.
It’s common to allow the parents to remain with the child during the procedure as long as appropriate precautions are taken. In addition, follow these steps:
Tell the child that it’s his job to remain still during the procedure.
Obtain previous X-rays if possible, which may be useful for comparison.
If an adolescent female is sexually active, assess for possible pregnancy, a contraindication for radiography.
Remove metallic objects, such as jewelry or snaps on gowns, before the X-ray because metallic objects may be mistaken for pathology.
Treatments and procedures
Children may experience dysfunction in any part of the musculoskeletal system. Treatment depends on a thorough assessment and appropriate interventions based on findings. These interventions are typically designed to promote healing and lessen the impact of the condition on mobility. Principles of body mechanics are used to maintain the integrity of the musculoskeletal system.
Prevent and restore
Nursing care of orthopedic conditions involves the correction of alterations in the musculoskeletal system. These preventive and restorative measures include:
casting or splinting and traction, which are used to help correct, maintain, and support the body part in a functional position
surgical repairs such as tendon release
limb amputations, which may be necessary in some circumstances.
Casting or Splints
Casts or splints may be required when a child has a fractured bone, weakness, paralysis, or spasticity. They’re also used following corrective orthopedic surgery.
The cast may be made of plaster or, more commonly, of synthetic material such as fiberglass or plastic. Polyester and cotton impregnated with water-activated polyurethane resin may also be used. (See Types of casts for children.)
Depending on the type of material that’s used, drying time for the cast may be as little as 7 minutes or as much as 48 hours. Weight bearing on the affected part of the body is typically avoided until the cast has dried.
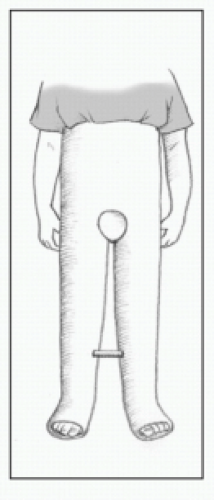
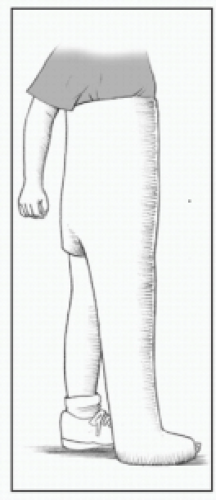
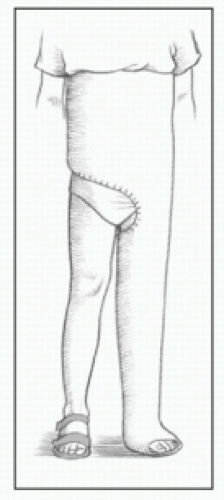
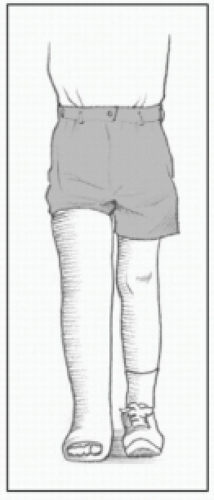
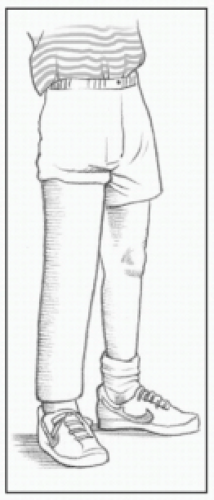
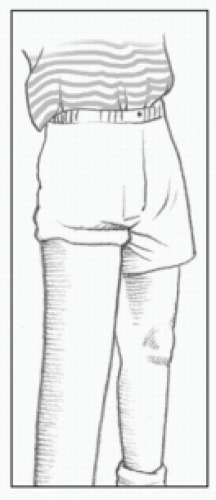
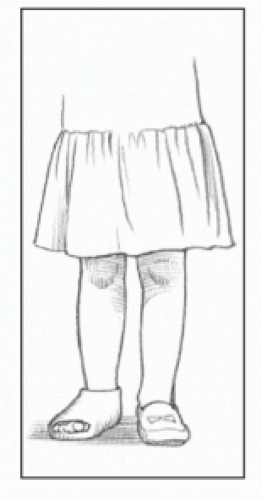
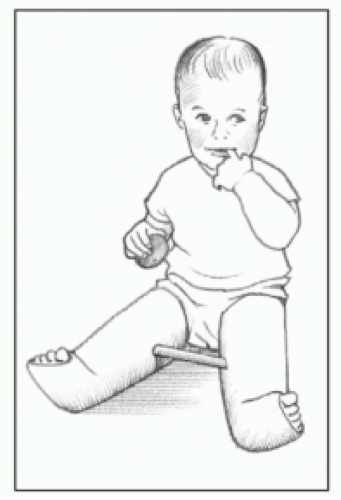
Types of casts for children
These illustrations show the types of casts commonly used for children.
Full spica cast
1½ spica cast
Single spica cast
Long leg cast
Cylinder cast
Short leg cast
Bootie cast
Bilateral long leg cast
Shoulder spica cast
Long arm cast
Short arm cast
Splints
Splints are “half-casts” and offer a bit more flexibility than a standard cast. They also do not offer quite as much support as a cast. Splints may be custom-formed to the child or may be ready-towear. Most splints have Velcro straps to adjust to the child’s body. Instruct the parent and the child to keep the splint on as much as possible and to avoid excess activities that would further compromise the injury.
A wash and a blow-dry
Some synthetic casts may be waterproof. Double check that the inner lining of the cast is waterproof as well before allowing the child to get the cast wet. If appropriate, instruct the patient and family to dry the cast after bathing or immersion by using a blowdryer on a cool setting.
Memory jogger
Remember the five “Ps” when checking for signs of compromised blood supply in a child with a cast.
Pain
Pallor
Paresthesia
Paralysis
Pulselessness
Nursing considerations
Explain each step of the procedure to the child before the procedure and again as the cast is being applied. If plaster will be used, explain that the child will experience a sensation of warmth when it’s first applied. As it dries, the cast—and the child—will feel cold.
In addition, follow these steps:
If a closed reduction is necessary, explain to the child that there will be some pain. Allow the parents to remain close to the child and hold his hand to help lessen anxiety.
Assess the casted area every 30 minutes for the first few hours, then every hour for 24 hours, then every 4 hours for an additional 48 hours. Drainage from a wound under the cast should be noted.
If there are signs and symptoms of compromise in the affected area, notify the doctor immediately. Also notify the doctor if cracks are noted in the cast.
Assess for signs of skin breakdown, a common occurrence. The area around the cast edges will typically become pink and warm and swelling may also occur. (Provide skin care to prevent further breakdown.)
Cast scratch fever
Because cool air can relieve the itchiness that accompanies casting, instruct the parents to blow cool air down into the cast using a blow-dryer on a cool setting. Also advise against putting an object down the cast in an attempt to scratch.
May I have your autograph?
Ask the child if he would like his nurses and doctors to sign his cast to help him cheer up, feel important to the medical staff, and view the staff as friends.
Explain to the child and parents that the cast must be worn as recommended. It shouldn’t be removed and overly rigorous activities should be discouraged (to prevent dislodgment or malalignment of a fracture).
The cut stops here—promise!
When the fracture is healed, prepare the child for cast removal with the cast cutter. Let him hear the noise and feel the vibrations, and show him (on your body) how the cutter stops when it touches skin and won’t, therefore, cut anything except the cast.
Inform the child that his skin will look different after cast removal, especially if it has been in the cast for weeks. Reassure him that this is temporary, and apply baby oil, then gently wash the area to remove the dead skin. (See Cast care.)
Instruct the child and parents in an exercise regimen to help regain muscle strength and function following the injury.
It’s all relative
Cast care
Be sure to include these points in your teaching plan for the child with a cast and his parents:
mechanism of bone healing and necessity for casting
cast care, including air exposure, elevation, and movement
measures to protect the cast
measures for skin care
methods to relieve itching
measures to keep the cast dry
ways to test for sensation, movement, and circulation
measures for coping with swelling
ways to relieve skin irritation
monitoring for wound drainage
exercises for the casted extremity.
Traction
Although it is not as widely used now, traction is still used in some circumstances. Traction can be continuous or intermittent. It’s used to:
stabilize or immobilize a certain body part
reduce muscle spasms
relieve pressure on spinal nerves
realign fractures or joint dislocations.
Just hanging out
Traction uses weights and pulleys to exert a pulling force and maintain the body part in correct alignment. Weights must hang freely and the ropes shouldn’t have knots that could interfere with free movement.
Serial X-rays are taken while the child is in traction in order to monitor progress and determine the need for changes in the direction and amount of traction pull.
Central location
The child should be kept in the center of the bed to maintain countertraction and prevent complications. Traction can cause muscle spasms that may require analgesics or muscle relaxants. The child is in bed for extended periods; therefore, circulatory and skin assessment is vital.
Traction in twos
There are two basic types of traction:
skin
skeletal.
Types of skin traction
This chart describes the various types of skin traction.
Traction
Purpose
Patient positioning
Buck’s extension
Used for a fractured hip to prevent muscle spasms and dislocation
Child lies flat in bed.
Head of the bed is elevated only for activities of daily living.
Cervical traction
Used for neck strain and arthritic or degenerative conditions of the cervical vertebrae
Child lies flat in bed or with the head of the bed elevated 15 to 20 degrees.
Dunlop’s traction
Used for a fractured humerus
Child lies flat in bed.
Arm is suspended horizontally.
Pelvic girdle
Used for muscle spasms, lower back pain, or a herniated disc
Child lies with head and knees raised to keep the hips flexed at a 45-degree angle.
Russell traction
Used for adolescents with a femur fracture or certain knee injuries
Child lies with the head of the bed elevated 30 to 45 degrees.
Bryant’s traction
Used for children with a fractured femur who are younger than age 2 years and weigh less than 31 lb (14 kg)
Hips are flexed at a 90-degree angle.
Buttocks are raised 1′′ (2.5 cm) above the mattress.
Skin traction
Skin traction is a noninvasive traction that’s especially useful for a child who may not require continuous traction. It’s applied by placing foam rubber straps against the affected part and then securing the straps with elastic bandages.
Sometimes, the straps have an adhesive backing. If this type of strap is used, the nurse should protect the skin by first applying compound benzoin tincture or other skin protectant. Traction should be removed by two people. (See Types of skin traction.)
Skeletal traction
Skeletal traction exerts a greater force than skin traction by using wires or pins inserted into the bone. They’re usually placed under anesthesia. Skeletal traction is continuous. (See Types of skeletal traction, page 426.)
Nursing considerations
The sight and idea of a body part in skeletal traction can be frightening to a child (and his parents). Explain what the child will see and feel before the traction is applied. Use dolls and toy traction devices to show the child what’s about to happen and help familiarize him with the equipment and reduce fear.
Types of skeletal traction
This chart describes the different types of skeletal traction.
Traction
Purpose
Special considerations
Thomas leg splint with Pearson attachment
Used for bone alignment and as a more effective line of pull
Child is placed in the supine position with the knee flexed.
External fixation devices (Ilizarov)
Used to manage open fractures that have soft tissue damage or to provide stability for severe comminuted fractures
Child is on bed rest (however, early mobility and active exercise of other joints are necessary).
Halo
Used to provide immobilization of the cervical spine and to support the neck following injury
Early ambulation is recommended.
The anterior metal bars maintain traction.
The posterior bars can be used to position the patient.
Used to maintain alignment of the cervical spine, for immobilization, and for reduction of cervical roll fractures
Child is on bed rest.
Special frames may be used for turning.
In addition, follow these steps:
Involve the family as much as possible to reduce anxiety, alleviate boredom, encourage cooperation with the recommended treatment, and minimize disruption of the family structure.
Maintain the traction system and frequently check the ropes, pulleys, and weights for proper function.
Maintain correct alignment of the affected body part.
Don’t fall behind
Provide age-appropriate activities to help maintain the child’s developmental level, prevent developmental delay, and alleviate boredom.
Frequently assess for signs of skin breakdown. Place sheepskin under the affected extremity to help alleviate pressure.
Provide footplates for the affected side to prevent footdrop.
Pin and skin
For the child in skeletal traction, assess the pin insertion sites for signs of infection or tenting (new skin that has attached to the insertion site, creating a tentlike configuration); tenting may cause the skin to tear, which can promote infection.
Clean the area around the pin insertion sites frequently, and cover the tips of the pins to prevent injury to the skin or other parts of the child’s body. Notify the doctor immediately if the pins become loose, and keep the child immobilized until skeletal traction is assessed.
Surgical repairs
At times, surgical repairs may be necessary to promote normal growth and development. Examples of these types of repairs include tendon release and leg-length corrections. Surgery to release a tendon involves cutting a part of the tendon in order to decrease the tension in the muscle that the tendon controls. Tendon release surgery is often used in correcting severe congenital clubfoot in young children. It can also be used on shoulder, hips, knees, or even thumbs.
Leg lengthening or shortening is often used to treat children who have an abnormally short or long leg causing a discrepancy between the two legs. Lengthening requires several surgeries over an extended length of time and is used if there is a significant difference (>5 cm or 2′′) between the leg lengths. Plates and screws (some may be external) are used to hold the cut bone in place and slowly pull apart the bone, allowing new bone to fill in the gap, thereby lengthening the bone. Bone growth restriction or shortening is used if there is less than a 5 cm (2′′) difference. Surgery is done to stop the epiphysis (growth plate) from promoting further growth. The metal plates and screws used may be removed after several months once complete healing has occurred.
Nursing considerations
As with any surgery, the child and family need to be prepared.
Allow the child and the parents to express their fears and answer any questions they may have about the procedure itself. In addition, follow these steps:
Following surgery, check the site for circulation, signs of infection, or complications.
Notify the health care provider if there are any abnormal signs.
Teach the parents how to care for the pin insertion site and signs and symptoms of any complications.
Amputation
Unfortunately, amputations occur in children as well as adults. An amputation may be needed because of a trauma; a disease process, such as osteosarcoma; or it may have occurred prenatally due to teratogens, metabolic diseases in the mother, or small pieces of the amnion that cut off circulation to a certain body part (known as an amniotic band). Only rarely is a congenital amputation genetically determined. Occasionally, a hair or a loose piece of thread can cause a tourniquet on an infant’s toes and feet or fingers and hands. This strand of hair or thread can wrap itself so tightly around a wiggling infant that it can cause significant damage to the extremity and may even lead to amputation if not caught in enough time (known as a hair tourniquet). In rare circumstances, it may be caused by child abuse. Teach the parents to daily take off mittens or booties and inspect for any loose threads or hair.
A loss that lasts
Limb amputation that isn’t congenital can be traumatic to a child or adolescent and his family. It may be particularly damaging to the child’s self-image. Everyone deals with feelings of loss in his own way and in his own time; there’s no right or wrong way to grieve. Families need extra time and support to deal with the grief and loss they feel when they’re given the news that amputation is required.
Something in common
It may be helpful to introduce the child and family to another family who has gone through an amputation and has learned to cope successfully with day-to-day activities and enjoy life. Support groups such as the Amputee Coalition have pediatric support groups in many areas around the country.
Many amputations are treated with a prosthesis. Sometimes, stump shrink bandages are used to apply pressure, reduce swelling, and help mold the stump for fitting a prosthesis, which usually can be done within 4 to 6 weeks after the amputation.
Quick studies
Children quickly learn how to function with a prosthesis and can lead very active, normal lives. They should be reassured that amputation doesn’t have to mean permanent disability. Many children participate in sports and other strenuous activities while using a prosthesis. The nurse can play an essential role in helping the child and his family cope with this traumatic situation.
Only gold members can continue reading. Log In or Register to continue
 Just the facts
Just the facts

 It’s all relative
It’s all relative skin
skin skeletal.
skeletal.