tests used to diagnose endocrine and metabolic problems
treatments for children with endocrine and metabolic problems
disorders of the endocrine system and metabolic function.
Anatomy and physiology
The endocrine system is composed of glands that secrete hormones necessary for normal metabolic function. Along with the nervous system, the endocrine system regulates and integrates the body’s metabolic activities. (See Endocrine system components, page 508.)
Too little, too much
Altered endocrine function involves a hyposecretion or hypersecretion of hormones, which affects the body’s metabolic processes and function. Nursing care involves measures to support hormonal secretion, such as hormone replacement, or curtail secretion, such as radiation therapy. Inborn errors of metabolism involve a biochemical alteration that affects metabolism.
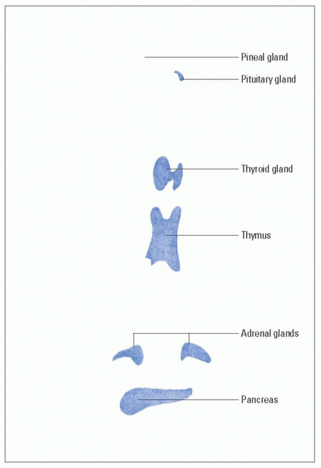
Endocrine system components
Endocrine glands secrete hormones directly into the bloodstream to regulate body function. This illustration shows the locations of the major endocrine glands (except the gonads).
Glands
The major glands of the endocrine system are:
pituitary gland
thyroid gland
parathyroid glands
adrenal glands
pancreas
ovaries and testes.
Pituitary gland
The pituitary gland (also called the hypophysis or master gland) rests in the sella turcica, a depression in the sphenoid bone at the base of the brain.
Small but mighty
This pea-sized gland connects with the hypothalamus via the infundibulum, from which it receives chemical and nervous stimulation. The pituitary has two main regions:
anterior pituitary
posterior pituitary.
Prolific producer
The anterior pituitary, also called the adenohypophysis, makes up 80% of the pituitary gland. It produces seven hormones:
growth hormone (GH), or somatotropin
thyroid-stimulating hormone (TSH), or thyrotropin
corticotropin
follicle-stimulating hormone (FSH)
luteinizing hormone (LH)
prolactin
melanocyte-stimulating hormone.
Hormones in storage
The posterior pituitary, or neurohypophysis, makes up about 20% of the pituitary gland. It serves as a storage area for antidiuretic hormone (ADH), or vasopressin, and oxytocin, which are produced by the hypothalamus.
Thyroid gland
The thyroid gland lies directly below the larynx, partially in front of the trachea. Its two lateral lobes—one on either side of the trachea—join with a narrow tissue bridge, called the isthmus, to give the gland its butterfly shape.
Thyroid lobe duo
The two lobes of the thyroid gland function as one unit to produce the hormones triiodothyronine (T3), thyroxine (T4), and calcitonin. T3 and T4 are collectively referred to as thyroid hormones (THs), the body’s major metabolic hormones. They regulate metabolism by speeding cellular respiration.
The calcitonin-calcium connection
Calcitonin maintains the blood calcium level by inhibiting the release of calcium from bone. Secretion of calcitonin is controlled by the calcium concentration of the fluid surrounding the thyroid cells.
Parathyroid glands
The parathyroid glands are the body’s smallest known endocrine glands. These glands are embedded on the posterior surface of the thyroid, one in each corner.
PTH: A parathyroid production
Working together as a single gland, the parathyroid glands produce parathyroid hormone (PTH). The main function of PTH is to help regulate the blood’s calcium balance. This hormone adjusts the rate at which calcium and magnesium ions are removed from urine. PTH also increases the movement of phosphate ions from the blood to urine for excretion.
Adrenal glands
There are two adrenal glands in the body; each gland is situated on top of a kidney. These almond-shaped glands contain two distinct structures—the adrenal cortex and the adrenal medulla— that function as separate endocrine glands.
Adrenal cortex
The adrenal cortex is the large outer layer of the adrenal gland and forms the bulk of the gland. It has three zones, or cell layers:
zona glomerulosa, the outermost zone, which produces mineralocorticoids, primarily aldosterone
zona fasciculata, the middle and largest zone, which produces the glucocorticoids cortisol (hydrocortisone), cortisone, and corticosterone as well as small amounts of the sex hormones androgen and estrogen
zona reticularis, the innermost zone, which produces mainly glucocorticoids and some sex hormones.
Adrenal medulla
The adrenal medulla, or inner layer of the adrenal gland, functions as part of the sympathetic nervous system and produces two catecholamines:
epinephrine
norepinephrine.
A leading role
Because catecholamines play an important role in the autonomic nervous system, the adrenal medulla is considered a neuroendocrine structure.
Pancreas
The pancreas, a triangular gland, is nestled in the curve of the duodenum, stretching horizontally behind the stomach and extending to the spleen. The pancreas performs endocrine and exocrine functions. Acinar cells make up most of the gland and regulate pancreatic exocrine function.
Clusters of islets
The endocrine cells of the pancreas are called the islet cells, or islets of Langerhans. These cells exist in clusters and are found scattered among the acinar cells. The islets contain alpha, beta, and delta cells that produce important hormones:
Alpha cells produce glucagon.
Beta cells produce insulin.
Delta cells produce somatostatin.
Gonads
The gonads include the ovaries in the female and the testes in the male.
Ovaries
The ovaries are oval-shaped glands in females located on either side of the uterus. They produce ova (eggs) as well as estrogen and progesterone.
It’s a girl thing
Estrogen and progesterone are responsible for:
promoting the development and maintenance of female sex characteristics
regulating the menstrual cycle
maintaining the uterus for pregnancy
preparing the mammary glands for lactation.
Testes
The testes are located in the scrotum. They produce the male hormone testosterone, which stimulates and maintains male sex characteristics. They also produce spermatozoa.
Hormones
Hormones are complex chemical substances that trigger or regulate the activity of an organ or a group of cells. They include pituitary hormones, THs, adrenal hormones, and androgens and estrogens. (See Effects of altered hormonal function.)
Pituitary hormones
Pituitary hormones include the anterior pituitary hormones (GH, TSH, FSH, LH, and prolactin) and the posterior pituitary hormones (ADH and oxytocin). Each of these hormones has a particular function:
GH, secreted by the anterior pituitary gland, affects most body tissues. It triggers growth by increasing protein synthesis and fat mobilization and decreases carbohydrate use.
TSH is secreted by the anterior pituitary gland and stimulates the thyroid.
FSH, secreted by the anterior pituitary gland, stimulates the graafian follicles to mature and secrete estrogen in the female. In males, it stimulates development of the seminiferous tubules.
LH, secreted by the anterior pituitary gland, produces the rupture of the follicle, which results in the discharge of a mature ovum in the female. In the male, it stimulates the production of androgens, particularly testosterone.
Prolactin is secreted by the anterior pituitary gland and stimulates milk secretion.
ADH is secreted by the posterior pituitary gland. It controls the concentration of body fluids by altering the permeability of the distal convoluted tubules and collecting ducts of the kidneys to conserve water.
Oxytocin, secreted by the posterior pituitary gland, stimulates the contraction of the uterus and the letdown reflex in lactating women.
Thyroid hormones
The THs are T3 and T4. These hormones are necessary for normal growth and development and act on many tissues to increase metabolic activity and protein synthesis.
Effects of altered hormonal function
This chart shows the effects that may result from excessive or deficient secretion of select hormones.
• Absence or loss of secondary sex characteristics
• Amenorrhea
• Precocious puberty
• Primary gonadal failure
• Hirsutism
• Polycystic ovary
• Early epiphyseal closure
LH
• Hypogonadism
• Sterility
• Impotence
• Absence or loss of secondary sex characteristics
• Ovarian failure
• Precocious puberty
• Primary gonadal failure
• Hirsutism
• Polycystic ovary
• Early epiphyseal closure
Prolactin
• Inability to lactate
• Amenorrhea
• Galactorrhea
• Functional hypogonadism
Melanocyte-stimulating hormone
• Diminished or absent skin pigmentation
• Increased skin pigmentation
Posterior pituitary hormone
Antidiuretic hormone or vasopressin
• Diabetes insipidus
• Syndrome of inappropriate antidiuretic hormone secretion
• Fluid retention
• Hyponatremia
Thyroid hormones
T4 and T3
• Hypothyroidism
• Myxedema
• Hashimoto thyroiditis
• Greatly reduced general growth (extent depends on age at which deficiency occurs)
• Mental retardation (in infants)
• Exophthalmic goiter (Graves’ disease)
• Accelerated linear growth
• Early epiphyseal closure
Parathyroid gland hormone
PTH
• Hypocalcemia (tetany)
• Hypercalcemia (bone demineralization)
• Hypophosphatemia
Adrenal hormones
Aldosterone
• Adrenocortical insufficiency
• Electrolyte imbalance
• Hyperaldosteronism
Glucocorticoids (cortisol and corticosterone)
• Addison’s disease
• Acute adrenocortical insufficiency
• Impaired growth and sexual function
• Cushing’s syndrome
• Severe impairment of growth with slowing in skeletal maturation
Adrenal hormones
The adrenal hormones are cortisol, aldosterone, androgens, and estrogen:
Cortisol is a glucocorticoid that stimulates glucogenesis and increases protein breakdown and free fatty acid mobilization; it also suppresses the immune response and provides for an appropriate response to stress.
Aldosterone, a mineralocorticoid, regulates the resorption of sodium and the excretion of potassium by the kidneys; it’s affected by corticotropin and is regulated by angiotensin II, which, in turn, is regulated by renin. Together, aldosterone, angiotensin II, and renin are involved in the pathogenesis of hypertension.
Androgens are male sex hormones; they promote male traits, especially secondary sex characteristics, such as facial hair and a low-pitched voice.
Estrogens are responsible for the development of secondary female sex characteristics.
Pancreatic hormones
The islets of Langerhans are small clusters of endocrine cells in the pancreas. These structures contain cells that produce insulin, glucagon, and somatostatin:
Insulin: a hormone that raises the blood glucose level by triggering the breakdown of glycogen to glucose
Glucagon: lowers the blood glucose level by stimulating the conversion of glucose to glycogen
Somatostatin: inhibits the release of GH, corticotropin, and certain other hormones
Hormone release and transport
Although all hormone release results from endocrine gland stimulation, release patterns of hormones vary greatly.
Secretion of PTH (by the parathyroid gland) and prolactin (by the anterior pituitary) occurs fairly evenly throughout the day.
Corticotropin (secreted by the anterior pituitary) and cortisol (secreted by the adrenal cortex) are released in spurts in response to body rhythm cycles; levels of these hormones peak in the morning.
Secretion of insulin by the pancreas has both steady and sporadic release patterns.
Hormonal action
When a hormone reaches its target site, it binds to a specific receptor on the cell membrane or within the cell. Polypeptides and some amines bind to membrane receptor sites. The smaller, more lipid-soluble steroids and THs diffuse through the cell membrane and bind to intracellular receptors.
Right on target!
After binding occurs, each hormone produces unique physiologic changes, depending on its target site and its specific action at that site. A particular hormone may have different effects at different target sites.
Hormonal regulation
To maintain the body’s delicate equilibrium, a feedback mechanism regulates hormone production and secretion. The mechanism involves hormones, blood chemicals and metabolites, and the nervous system. The feedback mechanism may be simple or complex.
For normal function, each gland must contain enough appropriately programmed secretory cells to release active hormone on demand.
Unsupervised cells
Secretory cells need supervision. A secretory cell can’t sense on its own when to release the hormone or how much to release. It gets this information from sensing and signaling systems that integrate many messages. Together, stimulatory and inhibitory signals actively control the rate and duration of hormone release.
It’s nice to be recognized
When released, the hormone travels to target cells, where a receptor molecule recognizes it and binds to it. The sensitivity of a target cell depends on how many receptors it has for a particular site. The more receptor sites, the more sensitive the target cell.
Diagnostic tests
Diagnostic tests are used to assess endocrine system problems and metabolic function in the pediatric population:
Blood glucose tests are used to diagnose type 1 and type 2 diabetes mellitus. Blood glucose tests commonly used for the pediatric patient include the fasting blood glucose test and the oral glucose tolerance test (OGTT).
Growth hormone tests are used to determine pituitary function. The human growth hormone (hGH) test helps detect hypopituitarism, whereas the growth hormone suppression test is used to diagnose pituitary hyperfunction.
Neonatal screening, which began in the 1960s, is now performed in every state and may consist of tests for a variety of diseases. Typically, neonatal screens are performed for commonly occurring diseases that may cause severe mental retardation or death without early detection and treatment. These tests are all done by dried filter paper blood spots. A very small amount of blood is required and is usually obtained by a heel stick. An example of endocrine and metabolic tests that may be screened for during newborn screening include phenylketonuria (PKU), maple syrup urine disease (MSUD), galactosemia, congenital adrenal hyperplasia, and congenital hypothyroidism.
Thyroid function tests are used to determine thyroid function and include T4 and T3 studies.
Radioimmunoassay is a test used to measure minute quantities of hormones.
Glucose, fasting plasma
The fasting plasma glucose test (also known as the fasting blood sugar test) is commonly used to screen for diabetes mellitus. It measures plasma glucose levels after an 8-hour fast.
To fast or not to fast
In the fasting state, plasma glucose levels decrease, stimulating the release of the hormone glucagon. Glucagon then acts to raise plasma glucose by accelerating glycogenolysis, stimulating glyconeogenesis, and inhibiting glycogen synthesis. Normally, secretion of insulin checks this rise in glucose levels. In diabetes, however, absence or deficiency of insulin allows persistently high glucose levels.
And the level is …
The normal range for fasting plasma glucose varies according to the laboratory procedure. Normal values after a fast of at least 8 hours differ according to the age of the child:
premature neonates—40 to 65 mg/dl (SI, 2.2 to 3.6 mmol/L)
young children (birth to age 2 years)—60 to 110 mg/dl (SI, 3.3 to 6.1 mmol/L)
children (ages 2 to 18 years)—60 to 100 mg/dl (SI, 3.3 to 5.6 mmol/L).
Glucose tells all
A fasting plasma glucose level of 126 mg/dl or higher obtained on two or more occasions confirms provisional diabetes mellitus. An impaired blood glucose level is 125 mg/dl. A borderline or transiently elevated level requires a 2-hour postprandial plasma glucose test or an OGTT to confirm the diagnosis.
Nursing considerations
Explain the procedure to the parents and the child, and encourage the parents to stay with the child.
Determine how long the child must fast.
Determine if the timing of the patient’s medication will interfere with the test results and withhold medication if indicated.
Backup plan
Apply a topical anesthetic (when possible) to two spots so an alternate puncture site will be available if the first one isn’t successful.
Specify on the laboratory request the time the patient last ate, the sample collection time, and the time he received the last pretest dose of insulin (if applicable).
Glucose tolerance, oral
The OGTT measures carbohydrate metabolism after ingestion of a challenge dose of glucose. A 2-hour OGTT is typically done to diagnose diabetes mellitus in children. (See Administering oral glucose solutions, page 518.)
Administering oral glucose solutions
The oral glucose load in a glucose tolerance test usually varies from 50 to 100 g. The American Diabetes Association recommends a glucose dose of 40 g/m2 of body surface area, as calculated by a nomogram based on height and weight. Other authorities advocate a glucose load of 1.75 g/kg of body weight, which is especially useful in testing pediatric patients.
Glucose in disguise
Many patients become nauseated after drinking the overly sweet glucose solution. One way to make the solution more palatable is to dissolve it in water, flavor it with lemon juice, and chill it. Another way is to substitute Glucola, a carbonated drink, or Gel-a-dex, a cherry-flavored gelatin, for the appropriate amount of glucose.
Up to the challenge?
The body absorbs the challenge dose rapidly, causing plasma glucose levels to rise and peak within 30 minutes to 1 hour. The pancreas responds by secreting more insulin, causing glucose levels to return to normal after 2 to 3 hours.
During this period, plasma and urine glucose levels are monitored to assess insulin secretion and the body’s ability to metabolize glucose. Occasionally, glucose levels are monitored for an additional 2 to 3 hours to aid in the diagnosis of hypoglycemia and malabsorption syndrome.
A little intolerant
Some patients with diabetes may have fasting plasma glucose levels in the normal range; however, insufficient secretion of insulin after ingestion of carbohydrates causes plasma glucose levels to rise sharply and return to normal slowly. This decreased tolerance for glucose helps confirm diabetes.
Nursing considerations
Explain to the child and his parents that the test usually requires five blood samples and five urine specimens. Provide the child with coping mechanisms and help him deal with the multiple blood draws by giving him a small reward, such as a sticker, after each blood draw.
In addition, follow these steps:
Instruct the parents that the child must fast for 8 to 12 hours before the test because the first blood test is a fasting glucose level.
Send blood and urine samples to the laboratory immediately, or refrigerate them.
Specify blood and urine collection times and the time the child last ate.
As appropriate, record the time that the child received his last pretest dose of insulin or oral antidiabetic drug.
Blood totals
If the patient is an infant or young child, keep an ongoing record of repeated specimen collection and a total of the amount of blood collected.
As ordered, resume administration of medications withheld before the test.
Growth hormone, human
The hGH test is used to detect hypopituitarism. Also known as growth hormone and somatotropin, hGH is a protein secreted by the anterior pituitary and is the primary regulator of human growth. Children generally have higher hGH levels than adults; these levels can range from undetectable to 16 ng/ml (SI, 16 mcg/L).
The hGH test, a quantitative analysis of plasma hGH levels, is usually performed as part of an anterior pituitary stimulation or suppression test.
The lowdown on levels
Increased hGH levels may indicate a pituitary or hypothalamic tumor (commonly an adenoma), which causes gigantism in children and acromegaly in adults and adolescents.
The highs …
Patients with diabetes mellitus sometimes have elevated hGH levels without acromegaly. Suppression testing is necessary to confirm the diagnosis.
… and the lows
Pituitary infarction, metastatic disease, and tumors may reduce hGH levels. Dwarfism may be caused by low hGH levels, but confirmation of the diagnosis requires stimulation testing with arginine or insulin.
Nursing considerations
Prepare the child for the test with a simple, developmentally appropriate explanation. Tell the child and his parents that another sample may have to be drawn the following day for comparison. Explain to the parents that the laboratory requires at least 2 days of samples for analysis.
In addition, follow these steps:
Withhold all medications that affect hGH levels, such as pituitary-based steroids, as ordered. If these medications must be continued, note this on the laboratory request.
Make sure the patient is relaxed and recumbent for 30 minutes before the test because stress and physical activity elevate hGH levels. Explain that the child must fast and limit physical activity for 10 to 12 hours before the test.
Between 6 a.m. and 8 a.m. on 2 consecutive days, or as ordered, draw venous blood and send it to the laboratory.
Growth hormone suppression
The growth hormone suppression test, also known as the glucose loading test, is used to diagnose pituitary hyperfunction. It evaluates excessive baseline levels of hGH from the anterior pituitary by measuring the secretory response to a loading dose of glucose.
Failure to suppress
Normally, hGH raises plasma glucose and fatty acid concentrations; in response, insulin secretion increases to counteract these effects. A glucose load should suppress hGH secretion. In a patient with excessive hGH levels, the failure to suppress hGH indicates anterior pituitary dysfunction and confirms a diagnosis of acromegaly or gigantism.
Glucose normally suppresses hGH to levels ranging from undetectable to 3 ng/ml (SI, 3 mcg/L) in 30 minutes to 2 hours. In a patient with active acromegaly, basal hGH levels are elevated to 75 ng/ml (SI, 75 mcg/L) and aren’t suppressed to less than 5 ng/ml (SI, 5 mcg/L) during the test. In children, rebound stimulation may occur after 2 to 5 hours.
Rest and repeat
When the hGH levels are unchanged or increased in response to glucose loading, hGH hypersecretion is indicated and may confirm suspected acromegaly or gigantism. This response may be verified by repeating the test after a 1-day rest.
Nursing considerations
Explain the test to the child and his parents. Tell the child that he may experience nausea after drinking the glucose solution, and prepare him for the needle sticks. In addition:
Withhold all steroids; if these or other medications must be continued, note this on the laboratory request.
Administer 100 g of glucose solution by mouth; to prevent nausea, tell the child to drink the glucose slowly.
Guthrie screening
The Guthrie screening test, also known as the phenylalanine test, is a screening method used to detect elevated levels of serum phenylalanine, a naturally occurring amino acid essential for growth and nitrogen balance.
Metabolic upset
Elevated levels of phenylalanine may indicate PKU, a metabolic disorder inherited as an autosomal-recessive trait. An infant with PKU usually has normal phenylalanine levels at birth, but after he begins feeding with breast milk or formula (both of which contain phenylalanine), levels gradually rise because of a deficiency of the liver enzyme that converts phenylalanine to tyrosine. The resulting accumulation of phenylalanine, phenylpyruvic acid, and other metabolites hinders normal development of central nervous system cells, causing mental retardation.
Three’s a charm
The serum phenylalanine screening test detects abnormal phenylalanine levels through the growth rate of Bacillus subtilis, an organism that needs phenylalanine to thrive. To ensure accurate results, the test must be performed after 3 full days (preferably 4 days) of breast milk or formula feeding. (In some states, a preliminary test is required 25 hours after birth.)
Danger ahead
Growth of B. subtilis on the filter paper indicates that serum phenylalanine levels are high enough to overcome the antagonist. Such a positive result suggests the possibility of PKU; diagnosis requires exact serum phenylalanine measurement and urine testing. A positive screening test may also result from hepatic disease, galactosemia (an inherited, autosomal-recessive disorder of galactose metabolism), or delayed development of certain enzyme systems. (See Confirming PKU.)
Only gold members can continue reading. Log In or Register to continue
 Just the facts
Just the facts
 anterior pituitary
anterior pituitary posterior pituitary.
posterior pituitary. growth hormone (GH), or somatotropin
growth hormone (GH), or somatotropin thyroid-stimulating hormone (TSH), or thyrotropin
thyroid-stimulating hormone (TSH), or thyrotropin corticotropin
corticotropin follicle-stimulating hormone (FSH)
follicle-stimulating hormone (FSH) luteinizing hormone (LH)
luteinizing hormone (LH) prolactin
prolactin melanocyte-stimulating hormone.
melanocyte-stimulating hormone.
 zona glomerulosa, the outermost zone, which produces mineralocorticoids, primarily aldosterone
zona glomerulosa, the outermost zone, which produces mineralocorticoids, primarily aldosterone zona fasciculata, the middle and largest zone, which produces the glucocorticoids cortisol (hydrocortisone), cortisone, and corticosterone as well as small amounts of the sex hormones androgen and estrogen
zona fasciculata, the middle and largest zone, which produces the glucocorticoids cortisol (hydrocortisone), cortisone, and corticosterone as well as small amounts of the sex hormones androgen and estrogen zona reticularis, the innermost zone, which produces mainly glucocorticoids and some sex hormones.
zona reticularis, the innermost zone, which produces mainly glucocorticoids and some sex hormones. epinephrine
epinephrine norepinephrine.
norepinephrine.





