Mercer’s Becoming a Mother Theory in Nursing Practice
Molly Meighan
Although guidelines, printed handouts, and educational materials are important, they cannot replace a nurse’s dialogue with the mother that leads to identifying and understanding her concerns. Nurses are in a unique position to have long term positive effects on mothers during this transition.
Women becoming mothers face increasingly complex situations with fewer role models. The period of transition into the new identity, from pregnancy and over the first year, is a time of much uncertainty that motivates the woman to seek out information and help. The kind of help or care she receives can have long-term effects for her and for her child. For that help or care to be relevant, the caregiver must understand the woman’s experience in this process.
(Mercer, 1995, p. vii)
The study of parental role attainment is complex because of the many factors and processes influencing its achievement. Table 17-1 lists factors that have been identified as having a direct effect on the maternal role. Despite the efforts of researchers to identify and study these and other factors, an understanding of the transition to the parental role remains elusive. Research with women in this process has been beneficial, improving the nursing care of families in a wide variety of settings. Mercer is among the researchers contributing most to understanding this process. She continued to develop and refine her theory based on additional research.
TABLE 17-1
Factors Influencing Maternal Role Identity
| Factors | Effect on the Maternal Role |
| Maternal age | Adolescent mothers are at increased risk for preterm birth and low-birth-weight infants, as well as increased risk for long-range financial, educational, and family structural problems. |
| Older mothers (>30 years) are at increased risk of fetal/infant and maternal health problems, as well as increased risk of depression. | |
| Birth experience | Birth is seen as a formal entry into motherhood. |
| The mother’s experience during birth is related to her knowledge, her self-concept, and her perceived control over the process. | |
| Early separation from infant | Early separation of mother and infant decreases opportunities for bonding or attachment to the child. Therefore, it may delay the process of maternal role attainment. |
| Social stress/social support | Stress has been associated with increased illness, but the effect of stress can be mediated by effective social support. The emotional support from a mate appears to be the most helpful support in the transition to the maternal role. |
| Personality traits | Temperament and learned traits of flexibility and empathy influence maternal role-taking. Empathy is especially important to the maternal role. |
| Self-concept | A positive self-concept influences an individual’s ability to relate to another, thus facilitating the process of maternal role attainment. |
| Childrearing attitudes | Maternal attitudes about childrearing have a direct effect on mothering behavior and are believed to have a direct effect on the child’s socialization. |
| Health status | Maternal illness decreases self-esteem and produces fatigue, which interferes with mothering. Illness may delay the process of maternal role transition. |
| Infant temperament | An infant who is not easily consoled or comforted can make the transition to motherhood more difficult by decreasing the woman’s perception of competence and her confidence in being a mother. |
| Infant health status | Health status is directly related to the infant’s ability to respond to the mother. The separation of mother and infant because of poor health delays the attachment process. The mother may be reluctant to begin the transition to the maternal role for fear that the infant may die. |
Note: Research on these factors yielded empirical evidence of a direct effect on the maternal role.
Data from Mercer, R. T. (1986). First-time motherhood: Experiences from teens to forties (pp. 6-22). New York: Springer.
History and Background
Mercer’s Theory of Maternal Role Attainment was based on her extensive research on the topic beginning in the late 1960s and early 1970s. The initial stimulus forthe development of the theory came from Reva Rubin, who was Mercer’s professor and mentor at the University of Pittsburgh, where Mercer earned a PhD (Bee, Legge, & Oetting, 1994). Rubin’s (1961, 1967a,b) work in defining and understanding maternal role attainment served as a foundational theory for obstetric nursing care for many years. Rubin (1977) described maternal role attainment as a process of “binding-in” (being attached to the child) and “maternal role identity” (seeing oneself in the role and having a sense of comfort about it) (p. 67). Rubin’s concepts and assertions about the variables influencing maternal role attainment served as the basis of Mercer’s research. Whereas Rubin focused on maternal role attainment during pregnancy and the first month after birth, Mercer expanded her concepts to include the first year following birth (Meighan, Bee, Legge, et al., 1998; Mercer, 1995).In addition, Mercer considered the parents, the influence of high-risk pregnancy, and maternal illness in her theory of role attainment.
The mother’s ability to cope with having an infant with a congenital defect was among Mercer’s earliest research interests. In addition, she studied the needs and concerns of breastfeeding mothers, adolescent mothers, and mothers with postpartum illness, as well as the response of fathers to stress and complications during the childbearing process. In 1981, Mercer introduced a framework for studying factors that affect the maternal role. The framework was more clearly defined in her book First-Time Motherhood: Experiences from Teens to Forties (Mercer, 1986). Mercer’s maternal role attainment theory and descriptive model were proposed in 1991 during a symposium at the International Research Conference, sponsored by the Council of Nurse Researchers and the American Nurses Association, Los Angeles, California (Bee, et al., 1994; R. Mercer, personal communication, January 4, 2000). Her theory and the theoretical framework for research were presented in her latest book, Becoming a Mother (Mercer, 1995).
In 2003, Mercer began to reexamine the Theory of Maternal Role Attainment and proposed changes based on current nursing research (Meighan, 2010). Mercer (2004) supported retiring the term Maternal Role Attainment in favor of the term, Becoming a Mother, because role attainment suggests an endpoint rather than the continuing evolvement that occurs in the role of mother. Mercer’s conclusions were based mostly on nursing studies about the cognitive and behavioral dimensions of women in the maternal role. Walker, Crain, and Thompson (1986a,b) raised questions about the continuing changes in a woman’s role as a mother, and Koniak-Griffin (1993) reached similar conclusions about maternal role attainment. Hartrick (1997) concluded that women undergo a process of continual self-definition in the role. McBride and Shore (2001) also suggested there may be a need to retire the term maternal role attainment because “it implies a static situation rather than a fluctuating process” (p. 79). Mercer (2004) explained that becoming a mother connotes continued growth and change in the mothering role and is more descriptive of the process. Mercer writes of motherhood as a lifelong commitment evolving over time.
Overview of Mercer’s Original Theory of Maternal Role Attainment
Mercer not only relied on the previous works of Rubin but also based her research on both role and developmental theories. In addition, she selected study variables from an extensive review of the literature, borrowed from several disciplines, and used a variety of research tools. Her studies served as the platform for the design and development of her Theory of Maternal Role Attainment. Many of the assumptions, definitions, and concepts are based on Rubin’s work, transition theories, and the role theories of Thorton and Nardi (1975).
Mercer’s (1979) definition of maternal role attainment was based on Rubin’s description of the process:
The maternal role may be considered…attained when the mother feels internal harmony with the role and its expectations. Her behavioral responses to therole’s expectations are reflexive and are seen in her concern for and competency in caring for her infant, in her love and affection for and pleasure in her infant, and [in] her acceptance of the responsibilities posed by the role (p. 374).
Mercer (1995) later explained:
The personal role identity stage is reached when the mother has integrated the role into her self system with a congruence of self and other roles; she is secure in her identity as mother, is emotionally committed to her infant, and feels a sense of harmony, satisfaction, and competence in the role (p. 14).
According to Mercer (1986, 1995), “the major components of the mothering role are: (1) attachment to the infant, (2) gaining competence in mothering behaviors, and (3) expressing gratification in maternal-infant interactions” (1986, p. 6; 1995, p. 13). Borrowing from transition theory, Mercer (1995) described the following concepts as having to do with maternal role attainment: “(1) pregnancy is a marker event upsetting the woman’s status quo, (2) pregnancy requires the woman to move from one reality to another, and (3) pregnancy requires a new role identity” (pp. 13, 14). Mercer (1986) stated that a woman who becomes a mother must do the following: “(1) recognize the permanency of the required change, (2) seek out information, (3) seek role models, and (4) test herself for competency” (p. 14).
Four stages of maternal role attainment adapted from Thorton and Nardi (1975)—anticipatory, formal (role-taking), informal (role-making), and personal (role identity)—are part of Mercer’s (1979, 1981, 1985a, 1986, 1990) theory. Table 17-2lists and describes these stages. The anticipatory stage is closely related to Rubin’s cognitive operations and fantasy stages (Rubin, 1967a,b), which included the mother’s acceptance of the fetus as a separate individual and fantasizing about the new baby. Mercer’s definition of the anticipatory stage included the initial social and psychological adjustments to pregnancy. Expectations of the maternal role are learned during this stage by seeking information from others in the role and by visualizing oneself in the role of mother. The formal (role-taking) stage begins with the birth of the infant. Professionals and others in the woman’s social environment often guide this stage. Maternal behavior is learned and replicated in this early stage. The informal (role-making) stage begins as the woman structures the maternal role to fit her based on past experiences and future goals. In the informal stage, she learns infant cues and develops her own unique style of mothering. The final stage is the personal (role identity) stage. The woman integrates mothering into her self-system. The role is internalized, and she views herself as a competent mother (Mercer, 1981).
TABLE 17-2
Comparison of Stages of Maternal Role Attainment and Becoming a Mother
| Maternal Role Attainment Stages | Stages of Becoming a Mother |
| This stage begins during pregnancy and includes the social and psychological adjustments to pregnancy. Expectations of the maternal role are explored. The woman seeks information from others in the role and visualizes herself as a mother. | |
| This stage begins with the birth of the infant and includes recovery from birth. In this role-taking stage, the woman learns from others in the role or from professionals and replicates their behavior. She gains competence through practice. | |
| This stage begins as the woman structures the maternal role to fit herself based on past experiences and future goals. The woman learns infant cues and develops her own unique style of mothering. Mercer (2004) describes it as “settling in” and becoming a new family (p. 17). | |
| This stage begins as the woman integrates mothering into her self-system, internalizes the role, and views herself as a competent mother. |
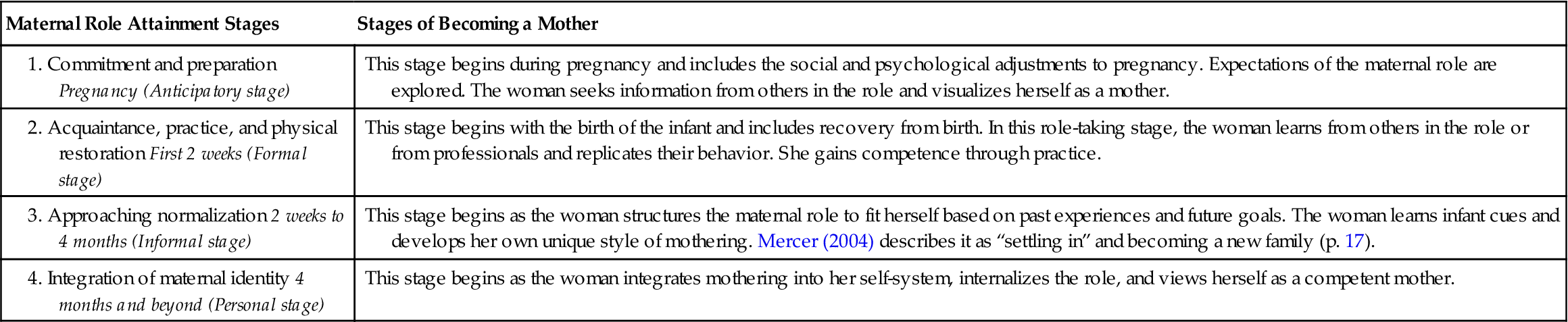
Data from Mercer, R. T. (1981). A theoretical framework for studying factors that impact on the maternal role. Nursing Research, 30, 73-77; Mercer, R. T. (2004). Becoming a mother versus maternal role attainment. Journal of Nursing Scholarship, 36(3), 465-477.
Stages of maternal role attainment and corresponding behaviors overlap and are often readjusted as the infant grows and develops. Maternal role identity may be achieved in 1 month or may require several months (Mercer, 1995). Several factors—including stress, social support, family functioning, and the mother’s relationship with the father—may have indirect or direct effects on role identity. Table 17-1 lists some of the factors related to maternal role identity.
Mercer (1995) expanded her earlier concepts to emphasize the importance of the role of the father or significant other. According to Mercer (R. Mercer, personal communication, January 4, 2000), the father (or the mother’s intimate partner) contributes to the process of role attainment in a way that cannot be duplicated by any other supportive person. As described by Donley (1993), maternal attachment to the infant develops within the emotional field of the parents’ relationship. Figure 17-1 illustrates the interactions among father, mother, and infant. The previously described stages of maternal role attainment are represented in layers a through d. Infant developmental stages are displayed in a similar fashion.
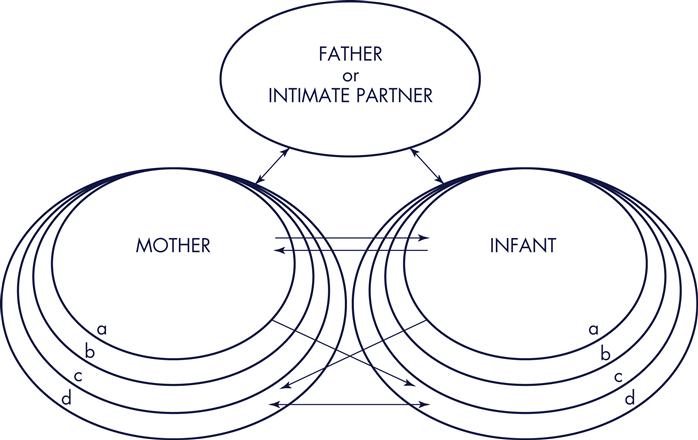
The father’s interactions help diffuse tension and facilitate maternal role identity (Donley, 1993; Mercer, 1995). The father’s role identity also occurs and increases with infant development and maternal role identity (Mercer, 1995). The interaction of mother, father (or significant other), and infant is an important concept added to the larger model presented by Mercer (1991) and described by Bee and colleagues (1994) (Figure 17-2).
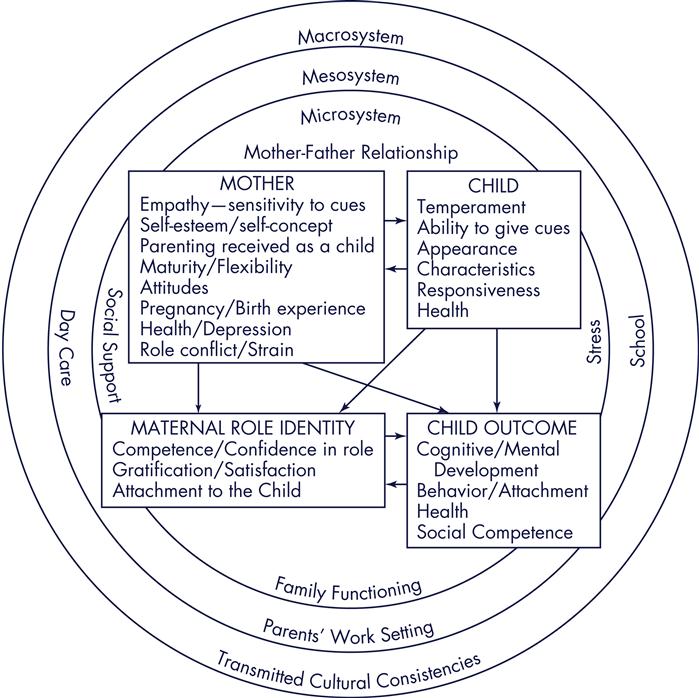
Mercer used a general systems approach in her model of maternal role attainment (see Figure 17-2). Bronfenbrenner’s (1979) design of nested circles provided the overall framework. The original model proposed by Mercer in 1991 during the International Research Conference in Los Angeles, California, was revised in her fifth book, Becoming a Mother (Mercer, 1995). In this book, the term exosystem, used earlier in the second circle, was replaced with the term mesosystem, used in a personal communication (R. Mercer, January 4, 2000). Mercer explained that this change was made to be consistent with Bronfenbrenner’s model, on which it was based.
The mother’s microsystem, which is the most influential on her maternal role attainment, includes the mother, her infant, her partner, and intimate relationships within her family (R. Mercer, personal communication, January 14, 2000).Maternal role attainment is achieved within this microsystem of father-mother-infant interaction (illustrated in Figure 17-1). The mesosystem includes extended family, school, work, church, and other systems within her more immediate community that directly influence the mother and her microsystem. The exosystem is an extension of the mesosystem and is described by Mercer (1995; R. Mercer, personal communication, January 4, 2000) as interrelationships of two or more settings (subsystems) that influence the mother more indirectly. Examples of mesosystem factors are interactions between the woman’s work setting, daycare, local laws/rules, or church. Examples of the outer circle or macrosystem include the social, political, and cultural influences on all of the systems.
Traits and behaviors influencing maternal role identity are included in the model. Maternal characteristics are empathy or sensitivity to infant cues, self-esteem or self-concept, parenting received as a child, maturity and flexibility, attitudes, pregnancy and birth experience, overall health, and role conflict or strain. Infant characteristics that influence maternal role attainment include temperament, ability to give cues, appearance, responsiveness, and health. The outcomes of maternal role identity include competence and confidence in the role, gratification in the role, and attachment to the child. Child outcomes are cognitive and mental development, behavior, attachment, health, and social competence.
A Revised Theory of Becoming a Mother
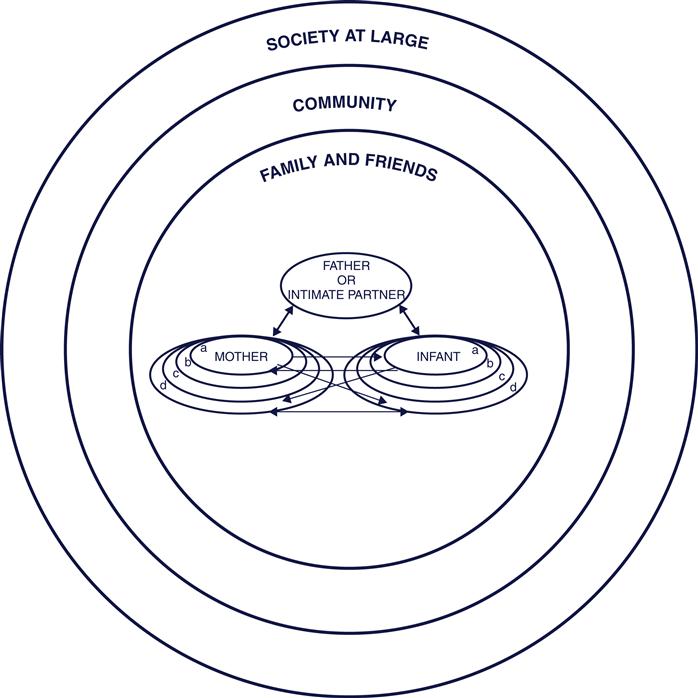
Mercer (2004) recognized theory building as a continual process as research provides evidence to clarify concepts, deletions, and additions. She continued workingtoward greater clarity and usability of her theory. Therefore, after extensive review of research, Mercer (2004) proposed adopting the process phrase becoming a mother and retiring the phrase maternal role attainment. Qualitative studies inspired Mercer to make additional changes in terminology based on the actual words used by women who were undergoing the experience of becoming a mother. Although there are some changes in the original terminology and concepts, the Theory of Becoming a Mother closely parallels the original Theory of Maternal Role Attainment as illustrated in Figure 17-3.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


