Chapter 21 Malpositions of the Occiput and Malpresentations
Occipitoposterior positions






Diagnosis during labour
 The woman may complain of continuous and severe backache worsening with contractions.
The woman may complain of continuous and severe backache worsening with contractions.
 Spontaneous rupture of the membranes may occur at an early stage of labour.
Spontaneous rupture of the membranes may occur at an early stage of labour.
 Contractions may be incoordinate.
Contractions may be incoordinate.
 There is slow descent of the head, even with good contractions.
There is slow descent of the head, even with good contractions.

Management of labour
Management is described in Box 21.1.
Box 21.1 Management of labour: occipitoposterior positions
First stage of labour
• Assist with pain management techniques, such as massage, changes of posture and position. Offer pharmacological pain control methods as appropriate
• Prevent dehydration and ketosis
• Correct any incoordinate uterine action or ineffective contractions with an oxytocin infusion
• The urge to push long before the cervix has become fully dilated may be eased by a change in position and the use of breathing techniques or nitrous oxide and oxygen to enhance relaxation
Second stage of labour
• Full dilatation of the cervix may need to be confirmed by a vaginal examination
• Encourage the woman to remain upright
• If contractions are weak and ineffective, an oxytocin infusion may be commenced
• The length of the second stage of labour is increased when the occiput is posterior, and there is an increased likelihood of operative delivery
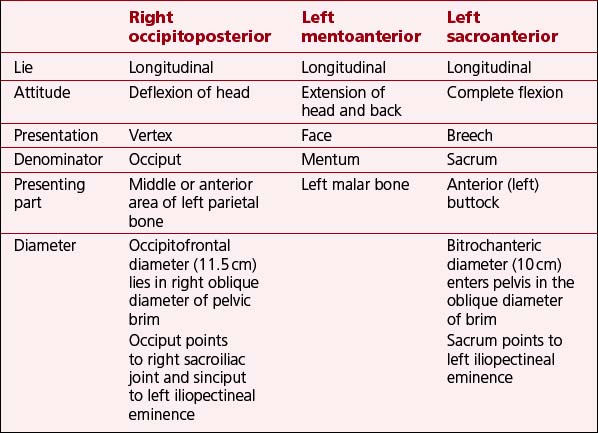
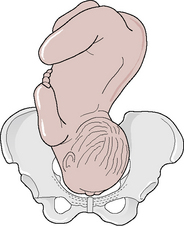
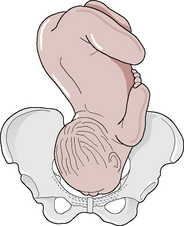
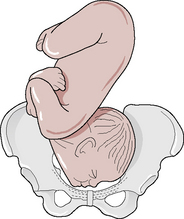
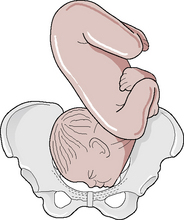
Mechanism of the right occipitoposterior position (Long rotation)
See Figures 21.1–21.4 and Table 21.1.
 Flexion. Descent takes place with increasing flexion. The occiput becomes the leading part.
Flexion. Descent takes place with increasing flexion. The occiput becomes the leading part.

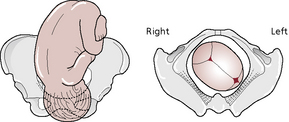
 Crowning. The occiput escapes under the symphysis pubis and the head is crowned.
Crowning. The occiput escapes under the symphysis pubis and the head is crowned.





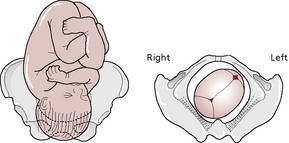
Fig. 21.1: Head descending with increased flexion. Sagittal suture in right oblique diameter of the pelvis.
Possible course and outcomes of labour
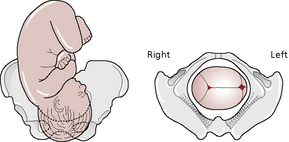
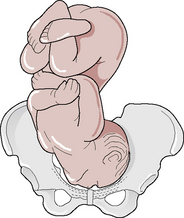
Short internal rotation (persistent occipitoposterior position)
This results from failure of flexion.
 The sinciput reaches the pelvic floor first and rotates forwards.
The sinciput reaches the pelvic floor first and rotates forwards.
 The occiput goes into the hollow of the sacrum.
The occiput goes into the hollow of the sacrum.





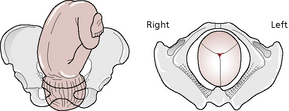
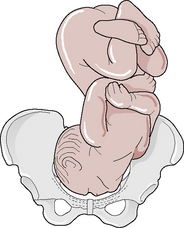
Deep transverse arrest
 This occurs when the occiput begins to rotate forwards but flexion is not maintained; the occipitofrontal diameter becomes caught at the narrow bispinous diameter of the outlet.
This occurs when the occiput begins to rotate forwards but flexion is not maintained; the occipitofrontal diameter becomes caught at the narrow bispinous diameter of the outlet.
 Arrest may be due to weak contractions, a straight sacrum or a narrowed outlet.
Arrest may be due to weak contractions, a straight sacrum or a narrowed outlet.









Face presentation
The attitude of the head is one of complete extension. It may be primary (presents before labour) or secondary (develops during labour). The denominator is the mentum and the presenting diameters are the submentobregmatic (9.5 cm) and the bitemporal (8.2 cm) (Figs 21.5–21.10).











Mechanism of the left mentoanterior position
See Table 21.1 (p. 232).







Possible course and outcomes of labour
Management of labour
Box 21.2 Management of labour: face presentations
First stage of labour
• Do not apply a fetal scalp electrode and take care not to infect or injure the eyes during vaginal examinations
• Following rupture of the membranes, exclude cord prolapse
• Observe descent of the head by abdominal palpation
• Assess cervical dilatation and descent of the head by vaginal examination every 2–4 hours. In mentoposterior positions, note whether the mentum is lower than the sinciput. If the head remains high in spite of good contractions, caesarean section is likely
Birth of the head
• When the face appears at the vulva, maintain extension by holding back the sinciput and permitting the mentum to escape under the symphysis pubis before the occiput is allowed to sweep the perineum. In this way the submentovertical diameter (11.5 cm), instead of the mentovertical diameter (13.5 cm), distends the vaginal orifice
• Because the perineum is also distended by the biparietal diameter (9.5 cm), an elective episiotomy may be performed
• If the head does not descend in the second stage and is in a mentoanterior position, it may be possible for the obstetrician to deliver the baby with forceps; when rotation is incomplete, or the position remains mentoposterior, a rotational forceps delivery may be feasible
• If the head has become impacted, or there is any suspicion of disproportion, a caesarean section will be necessary
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


