Chapter 10 Intrapartum fetal surveillance
PHYSIOLOGY AND PATHOPHYSIOLOGY
FETAL HEART RATE: BACKGROUND
FHR can be recorded intermittently by auscultation with a Pinard stethoscope or electronically by a Doppler instrument. Doppler recordings rely on ultrasound registration of the Doppler shift to signal FHR. Continuous electronic FHR monitoring (Figure 10.1) was introduced to provide uninterrupted intrapartum recordings. A fetal scalp electrode and intrauterine pressure recordings were used to provide the described classic patterns of transient FHR changes. Intrapartum pressure recording of uterine activity, however, is now usually replaced by use of external transducers to register sequential changes in uterine contraction. Correct placement of this external contraction device is important. Idiosyncrasies between the intrauterine and external methods for recording uterine contraction must be appreciated. The universal principle of need to understand the workings of tools used must apply since FHR change is read against the peak of the displayed uterine contraction.
Continuous electronic FHR monitoring is a screening adjunct for intrapartum fetal surveillance. Interpretation remains problematical and emphasises the need for constant education since failure to appreciate and react to signals of fetal insult is consistently identified as an avoidable factor in intrapartum fetal hypoxic damage or demise. Contemporary recommendation is that there should be an ongoing programme of education for interpretation of FHR changes for all involved in intrapartum care (Willis 2005).
Screening fetal welfare by recording FHR changes (cardiotocograms (CTGs)) should:
Further points
FETAL HEART RATE: TYPES
Baseline FHR
Transient changes in heart rate
Transient acceleration
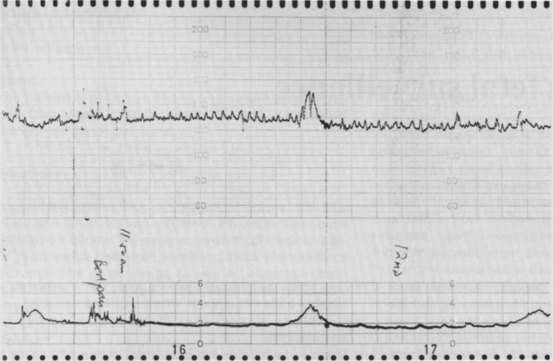
An increase in heart rate (15 beats per minute or more and lasting 15 or more seconds) throughout contraction is an early response to sympathetic stimuli (Figure 10.2) and reflects a fetus in good condition.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


