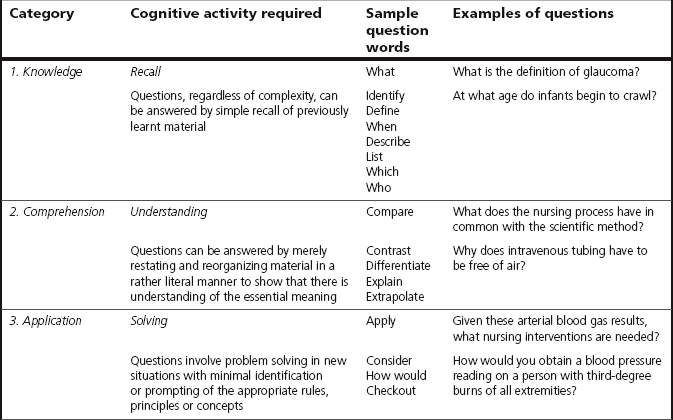
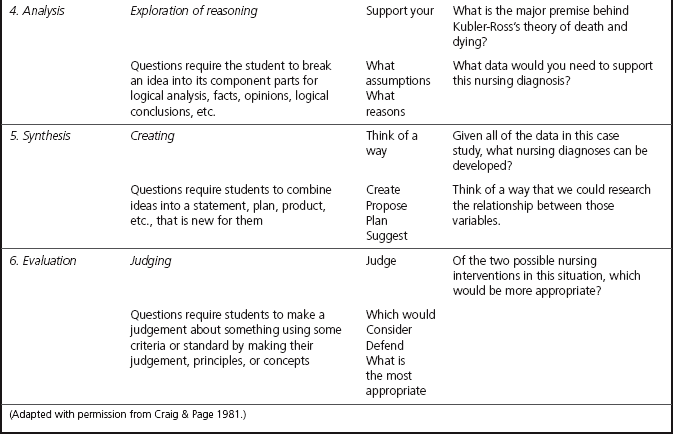
Chapter 4 It is discussed in Chapter 3 that competence is a construct that is not directly observable, but rather, is inferred from performance. Assessing performance will therefore be important to infer clinical competence. Equally important will be the requirement to gather sufficient evidence to justify the inference and, in particular, that a safe inference has been made (Gonczi et al 1993). Clinical competence is a complex entity and it almost always requires the practitioner to use a combination of attributes simultaneously and adapt practices to different contexts. Thus, the assessment of clinical competence is not straightforward and no one method can hope to assess overall competence. Moreover, some competencies are less easily assessed through performance than others. Hager & Gonczi (1996) state that it is not enough merely to observe performance in the complex world of professional work – a breadth of evidence is required to enable practice educators to make a sound inference that pre-registration health care students can perform competently in the variety of clinical situations in which they can find themselves. What is therefore needed is a ‘range of forms of evidence’ (Bedford et al 1993) to provide this breadth so that practice educators can make valid and reliable inferences. Following their extensive review of the literature on assessment of competence to practise, Redfern et al (2002) drew the conclusion that a multi-method approach enhances validity and ensures comprehensive assessment of the complex range of skills required of pre-registration nursing students. Consequently, it is necessary to use planned combinations of a variety of methods of assessment to obtain this ‘breadth of evidence’ to evaluate overall clinical competence, so that assessors of clinical practice know with confidence that the student has the necessary knowledge, skills and attributes to ensure public safety and protection. In the standard to support learning and assessment in practice, the Nursing and Midwifery Council (NMC 2008) requires practice educators to consider how evidence from various sources might contribute towards making a judgement on performance and competence. Bedford et al (1993) suggest that the strategy of triangulation is utilized to obtain this breadth of evidence. There is one key similarity between the processes of clinical assessment and research: simplistically, both seek to obtain data or evidence to add to the knowledge base about the subject and/or prove or disprove the case under investigation. In clinical assessment we seek data by which we obtain clearer perspectives of our learners, and evidence to confirm the achievement of competence for safe practice. When conducting clinical assessment there is much to be learnt from the rigour with which research studies are generally conducted in order to achieve validity and reliability of results. One rigorous research strategy is the use of triangulation. In this chapter the importance of using the strategy of triangulation to achieve validity and reliability of assessment is explored. In research, the technique of triangulation is used to obtain more valid and reliable research data. The principles guiding the use of this technique will be extrapolated for use in assessment so that assessments can also be conducted with the same degrees of validity and reliability as in research. The uses, merits and limitations of a range of methods that can be used in the competency-based approach for the assessment of clinical practice are also explored and debated. To reflect the principle of integration through the use of the holistic/integrated competency-based model of assessment (see Figure 3.4), integrated assessment approaches that use a combination of methods are put forward so that a number of competencies and their performance and knowledge outcomes can be assessed simultaneously. The theoretical perspectives of the term ‘triangulation’ are drawn from the literature on research, as literature that relates this term to the conduct of assessment is perfunctory and indirect (see, for example, Bedford et al 1993). Triangulation is a term borrowed by the social sciences from surveying and navigation. It refers to the principle of geometry that the third point of a triangle can be plotted using the two known points as the vertices (Fielding & Fielding 1986, in Redfern 1994). This concept of triangulation was first applied to research methodology by Campbell & Fiske (1959, in Redfern 1994) in psychological research as a metaphor to describe the use of several methods to measure a single construct in order to confirm a hypothesis. Triangulation in this context then does not mean three. Later researchers such as Denzin (1989) argue that triangulation is more than the use of several methods – it is the combination of ‘methodologies’ used to investigate the same phenomenon. These ‘methodologies’ are referred to as ‘types of triangulation’: four of them are described by Denzin (1989). From the work of Denzin, three types of triangulation are selected for exploration here, as these are seen to be relevant and applicable for the conduct of integrated assessments: they are therefore discussed and extrapolated to our discussion on assessment in this chapter. The types of triangulation are: There are two kinds of method triangulation: within-methods and between-methods. Data triangulation refers to the use of multiple data sources, with each source focused upon the phenomenon of interest (Denzin 1989). These data sources can differ by person, time or place. For example, data can be collected from different people or during different times or at different locations. The aim is that the data sources provide unique and diverse views about the same topic to contribute to validity and reliability: this enables the researcher to discover the dimensions of a phenomenon that are similar and dissimilar. As shown below, it is appropriate to make use of the three data sources as described by Denzin (1989) for the purposes of clinical assessment: • Person – assessment evidence is collected from other assessors and/or student self-evaluation. • Time – assessment evidence is collected on different clinical shifts over a period of time. • Place – assessment evidence is collected from the different instances of practice provided within the range of context in the learning contract (see Ch. 6). Investigator triangulation occurs when the different knowledge and expertise held by members of the research team are used in the analysis of raw data. When several investigators are involved in a study, this type of triangulation helps reduce the potential bias that occurs when only a single investigator is involved. In clinical assessment, investigator triangulation takes place when the range of evidence contributed by different assessors is used in the analysis of student competence. This will help reduce the potential bias of a single assessor. In their research report on the assessment of competence, Bedford et al (1993) recommend that: These ‘witnesses’ could be the assessor, other clinical colleagues, the clinical link lecturer and the service user. Each person is likely to ‘know’ the student in slightly different ways and be able to contribute to identification of the range of learning that has taken place, what the strengths and weaknesses of the student are and so on. Investigator triangulation may be particularly valuable when attempting to evaluate the student’s attitudes. Several people’s views are likely to have been collected after independent assessment of the student, thus reducing biases and adding to the reliability of the assessment (Phillips et al 2000). Whilst there is a requirement for service user and carer involvement in all aspects of the social work degree (Department of Health 2002), the involvement is not well tested as a valid source of witness testimony (Rhodes 2012, Elliott et al 2005, Edwards 2003). The use of evidence from the service user will be considered later in the chapter. So far, then, triangulation is about: • the use of different assessment methods or ways of collecting assessment evidence • ensuring that different assessment methods complement each other. You may wish to try Activity 4.1. 1. It allows confirmation of assessment evidence and increases confidence in the assessment decision made. By combining the types of triangulation – that is, method, data and investigator triangulation – a fuller and more complete picture of the student’s achievement or non-achievement is obtained. Different aspects of the student’s competence can be identified so that there is a richer and deeper understanding of the student’s learning, be it performance or knowledge and understanding or the development of some attitude or a set of values, which confirms our assessment of the student. This therefore increases our confidence when we are making the assessment decision. Consider this scenario: you have a student who is not achieving several competencies. You have come to this decision over several weeks of observing the student in practice and asking her questions about her practice. You wonder whether your decision is influenced by the fact that you do not like the student’s green and red hair! Another assessor provides assessment evidence that confirms your decision. You probably breathe a sigh of relief and say: ‘I’m not biased after all’. The testimony provided by another assessor increases your confidence in your assessment decision. Does this enhance the validity, or reliability, or both, of your assessment? (See discussion in Ch. 5.) 2. It guards against a blinkered perspective. The use of triangulation can potentially help to overcome the bias of ‘single-method, single-observer’ assessments (Redfern 1994). However, Redfern warns that the use of several methods and assessors may not compensate for assessor bias. It can be difficult to overcome strong likes and dislikes. 3. It is more likely to portray a ‘whole picture’ of the student. Rowntree’s (1987) book has this question as the title: Assessing Students: How Shall We Know Them? Attempting to ‘know’ students so that we are fair in our assessments of them requires us to understand a complex and multidimensional being. Furthermore, competencies are generally complex, which requires the student to learn and develop several attributes concurrently (see Ch. 3 for a discussion of the holistic/integrated competency-based model). A range of assessment evidence will provide a richer and deeper understanding of the student’s strengths and weaknesses and what has and has not been achieved, so that a fuller picture of the student’s achievement is obtained. We will then be in a better position to provide the guidance and support that the student requires in order to learn and achieve some more. 4. It allows divergent evidence to enrich explanation. When triangulation is used we are more likely to obtain or be given unexpected and divergent assessment evidence about the student. This should be regarded as a bonus (Redfern 1994), as such evidence may explain some aspect of the student or the student’s performance that has been eluding us. For example, a colleague who was working with your student may report to you that your student was observed to have been in tears when caring for a patient with terminal cancer. The student subsequently revealed that a close friend had recently died of cancer. For several weeks you have been attempting to involve the student in this aspect of care, but had been unsuccessful as the student was always reluctant. You were getting concerned that the student is not learning about care of patients with terminal cancer. The evidence from your colleague has served as a source of divergent evidence. 1. It is expensive on resources. When using triangulation, arrangements need to be made for the student to learn and practise over a range of contexts over time. Several assessment methods, including other assessors, need to be used: more resources, such as time and extra assessors, are required. In today’s climate of health care, where such resources are in scarce supply, the need for student supervision and assessment competes with the need to deliver care. It would be tempting, and certainly easier, to ignore the use of triangulation when assessing students! As was practised by the General Nursing Council for England and Wales in the 1970 s, the use of ‘one-off’ assessment when student nurses were assessed on four ‘one-off’ occasions, for a stated period of time on each occasion, for four aspects of learning, was much more economical on resources: Have you experienced this form of assessment? And how valid and reliable were the assessments? 2. It cannot compensate for assessor bias. If we cannot overcome our biases, or if we are not aware of them, the use of triangulation will not help us achieve the validity and reliability we desire in our assessment. 3. It may compound sources of error: This point relates to Point 2 above. If we hold some biases and the other assessor also holds some biases that are different from ours, our assessment evidence will not be as objective as we perceive. In fact, the student could be more disadvantaged than if we had not used the evidence from the other assessor. 4. Methods selected may be inappropriate. As discussed earlier, the assessment methods selected should complement each other so that a ‘rich’ range of evidence is provided to allow the development of professional competence to be assessed fully (Fotheringham 2010). This means we have to assess the development of knowledge, attitudes, skills and attributes. The selection of methods should allow the assessment of those areas of learning, performance and development equally, and not focus on the assessment of one or two domains of learning. For example, if we use observation to assess the student’s performance, the testimony of another assessor was also based on observation of practice and simulation as our assessment methods, we have assessed very well the student’s abilities to perform, but may not have assessed attributes such as understanding and attitudes well, if at all. 5. Triangulation is no use with the ‘wrong’ research question. This limitation is equally relevant to assessment. If we are not clear about what we want to assess, then triangulation is not going to enhance the validity and reliability of the assessment. It is therefore important to define, and describe clearly, the competency statement, the knowledge and performance outcomes we wish students to achieve. You may wish to try Activity 4.2. Despite the challenges and difficulties associated with the use of triangulation, the advantages of using this strategy indicate that it can give better opportunities to achieve validity and reliability of assessment. What this means when using the holistic/integrated competency-based approach to assessment is that both the attributes of the learner and the performance of key professional tasks are assessed. The discussion of competence in Chapter 3 stated that the attributes of individuals do not in themselves constitute competence. Nor is competence the mere performance of a series of tasks. Rather, the notion of competence integrates attributes with performance. Another point about competence to be reiterated is that competence is a construct that is not directly observable, but is inferred from successful performance. Therefore, combinations of assessment methods need to be considered and used so that a range of evidence is provided to enable a safe judgement of competence to be made (Gonczi et al 1993). This section starts with Activity 4.3. In my experience, the following methods are the most commonly used by assessors: • working with the students and observing their practice • asking questions leading to reflective discussions on contextualized practice • obtaining the opinion (testimony) of other assessors Gonczi et al (1993) say that all existing methods of assessment used by a profession are potentially appropriate for use in the competency-based approach to assessment. They go on to explain that it is not the methods themselves that are competency-based but the way they are used, the emphasis given to the methods and how results are interpreted that are important in competency-based assessment. The uses, merits and limitations of a range of methods that can be used for the assessment of the different components of professional competence are now explored. Observation simply means watching and noting what you see (Stoker 1994). Stoker (1994:iv) says that ‘observation is an essential tool in assessment – it is one of the most effective ways of finding out whether learning has taken place’. It is an NMC (NMC 2008) requirement that confirmation of clinical competence is made through direct observation of a student’s delivery of care in the practice setting. There is a better chance of making more accurate assessments if observation is part of a continuous process of working with the learner. Learners can be assessed on a number of occasions in their everyday working environment while they are performing in their ‘natural’ surroundings to give us a picture of their ability to perform a variety of real tasks so that direct evidence of competence can be collected. As the learner is watched in action, direct evidence of behaviours and behavioural patterns is obtained. Far more reliable judgements about professional competence are therefore possible than with assessments conducted in limited time periods on limited ranges of context. Assessments are also more likely to have predictive validity. There are two ways we can observe the learner’s performance: by participant and non-participant observation. Working directly with the learner is known as participant observation. In research, during participant observation, researchers join the group, often keeping their identities a secret to try to minimize any changes in behaviour that participants may be inclined to make as a result of being observed (Swanwick 1994). In clinical assessment, however, the identity of the assessor cannot be made a secret! Therefore, the effects of being observed – the observer effect – may affect the learner’s performance. The observer effect is discussed in Chapter 5. Another important point to bear in mind when observing practice is that of observer bias and how this may affect assessment; this is also discussed in Chapter 5. Observing the learner ‘from a distance’ is known as non-participant observation. In research, the researcher does not interact with the participants unless approached. If this happens, interaction is kept to a minimum (Swanwick 1994). During clinical assessment, we may observe the learner caring for a patient while we are performing another activity such as dispensing medications, talking to someone else and so on. What strategies have you used for observing a learner ‘from a distance’? Fletcher (1991:66) stated that in competence-based assessment ‘it is individual performance which is judged – and judged against explicit standards which reflect … the expected outcomes of that individual’s competent performance …’. When assessing for the development and achievement of a professional competency, the assessor looks for pre-specified behaviours such as the ways a skill is performed, or the ways the learner interacts with a patient, or how care is being given. These criteria are used to determine whether learning has taken place. When using observation to assess performance, noting these criteria in the form of a mental or written checklist (Stoker 1994) will guide the assessor’s observation. Dawson (1992) says that: Ewan & White (1996) recommend the use of written checklists, as they have a high inter-observer agreement. They also have the advantages of ensuring validity, discriminatory power and feasibility (Stoker 1994), concepts that are discussed in Chapter 5. As checklists are generally detailed, they provide a useful profile of performance that can be discussed with the learner and other assessors. When using written checklists, the following points may be useful to remember (Ewan & White 1996): • longer checklists tend to be more reliable than shorter ones • as checklists require the observer to judge whether certain behaviours have taken place, they are most effective where components of performance are specified in detail • it is possible to include behaviours that may underpin aspects of attitudes and interpersonal relationships • have three options for recording (i.e. observed, not observed, not applicable) • important errors should also be noted • if any essential component of the performance is omitted, the learner is assessed as not yet competent and is re-assessed. In particular instances it becomes necessary to assess the process of performance (Gonczi et al 1993). When observing these instances of practice, the ways of performing a task can also be included in a checklist, such as: Although the use of checklists has advantages, Ewan & White (1996) warn that if the criteria in the checklist emphasize the performance of a specific skill then beginning students may become fixated on specifics rather than learning the perspectives of care as a whole. Conversely, Benner (1984) thinks it necessary to break a psychomotor skill down into sequenced elements that the student can grasp in order to become technically competent as a beginning practitioner in the real world of clinical practice. One key facilitation skill of the practice educator is to be able to coach the student through the necessary paces to learn the psychomotor skill and, at the same time, learn about how to care for the patient. Assessments, in general, sample only a fraction of what a learner is expected to know. This is inevitable as it is not feasible or desirable to attempt to assess every aspect of learning; for example, it would be impractical to attempt to assess a pharmacist’s knowledge of every drug that could be encountered in everyday practice. Likewise, when assessing the competent clinical practice of students, inference of competence is inevitably based on a sampling of performance. Fish & Twinn (1997:114) made this important point about observing practice: ‘all seeing is selective, and all reporting of what is seen is interpretive; there is no such thing as purely objective factual observation’. It is important to remember that competence is a construct that is not directly observable, but is inferred from successful performance. There must therefore be enough evidence so that we are confident that it is safe to make the inference that the learner is competent. The assessor must therefore allow enough time to observe the learner on a number of occasions so that it is possible for sufficient evidence of learning to be demonstrated. It is an NMC requirement (NMC 2008) that most assessment of competence should be undertaken through direct observation in practice. It is also a requirement that, whilst giving direct care in the practice setting, at least 40% of a student’s time must be spent being supervised by the named practice educator. This working arrangement will give the practice educator more time to work with the student so that learning and progression can be monitored with accuracy. How does the assessor know when there is enough evidence? Making an assessment decision based on concrete evidence is one of the key principles of competency-based assessment. This important aspect of competency-based assessment is discussed in Chapter 7. So far, there has been a consideration of how to use observation as an assessment method, its usefulness or otherwise in ascertaining a true picture of the learner’s ability in ‘natural’ surroundings and some of the difficulties associated with its use. To summarize, effective observation (Stoker 1994) requires you to: Which components of competence can be assessed with any accuracy using observation? When a learner’s performance is observed, only overt behaviours and behavioural patterns exhibited by the learner when care is performed can be seen. Although behavioural patterns may indicate the underlying attitude (Andrusyszyn 1989), inwardly held beliefs, values or feelings cannot be seen (Dawson 1992), nor can knowledge and understanding of the care or task be determined. As an observer, one can only say that the observable performance is mainly a reflection of the possession of skills. Observation is therefore useful only for the assessment of the skills developed that are contributing to effective performance at the time. Gonczi et al (1993), however, claim that observation allows assessment of attitudes and interpersonal skills. Try Activity 4.5 on the use of observation as an assessment method. • Can provide a high level of integrated assessments. As the learner is observed performing care and tasks, it is possible to use evidence of performance to assess several competencies and several components of competence simultaneously. • Allows assessment of attitudes and interpersonal skills. Attitudes can be inferred from behaviours and behavioural patterns. Interpersonal skills can be directly observed. • Offers realistic evidence of competence. Competence-based assessment uses explicit standards of occupational performance as its foundation. The logical way to assess whether someone is meeting those standards is to watch them working in that occupation (Fletcher 1991). • Allows evaluation of problem solving. As the learner is observed managing a situation, it is possible to assess how well the learner has managed the situation. From this, it can be inferred that the learner has been able to solve the problem. • Mistakes in performance can be corrected. Direct observation and supervision of practice will enable the practice educator to identify and correct any mistakes at the time or immediately afterwards. • Circumstances of observation may be too specific. Evidence obtained about the ability to perform in care situations that occur rarely generally cannot be used with any degree of validity towards the assessment of many competencies. • Requires lengthy and costly assessments for reliability. The learner needs to be observed on more than one occasion to ensure reliability. This means that the period of assessment is longer rather than shorter and is therefore costly in terms of time and effort required. • Gives indirect evidence of knowledge/understanding only. If a learner is able to perform the care or task, it can only be inferred that knowledge/understanding underpins that performance. • Does not assess ability to learn through practice. Even if a learner is able to perform a task, or care for a patient, it cannot be assumed that the learner can transfer this performance to another situation and perform to the same standards another time. • Subject to observer bias and observer effect. Polit et al (2010) state that one of the most pervasive problems with observation is the vulnerability of observational data to distortions and biases – human perceptual judgemental errors can pose a serious threat to the validity and accuracy of observational information. An ability to perform is only one component of competence. Evidence of achievement of the other components of competence needs to be obtained using other assessment methods. Questioning frequently complements observation in that we are obtaining the ‘indirect evidence’ of competence, which is ‘hidden’ and not open to observation (Stoker 1994). It is discussed in Chapter 1 that one of the purposes of assessment is to maximize learning. Gipps (1994:15) made the point that ‘assessment alone will not develop higher-order skills in the absence of clearly delineated teaching strategies that foster the development of higher-order thinking in pupils’. Asking questions is an integral part of teaching and learning, and places students in the role of active learners (De Young 1990). It is one teaching/learning strategy to help students develop higher level cognitive skills. Questioning can also serve as positive reinforcement for students when we indicate that answers are correct and/or insightful. This gives feedback to the student that material has been understood and higher level thought processes were used (Activity 4.6). In clinical assessment, questioning can be used for the following purposes: • To assess baseline knowledge (e.g. knowledge of the stages of the grieving process). • To assess ability to form links between previously isolated information (e.g. if a student midwife is learning how to support women in labour, questions could be asked about the support strategies used for the individual woman and how well these worked for that woman; further questioning could then lead the student to explore those common strategies that work, or do not work, for a number of women the student has looked after). • To assess application of theory to practice (e.g. using the policy on infection control you had previously discussed with the learner, ask your learner to discuss the actions he/she would take when preparing for the admission of the next patient who requires barrier nursing). • To assess understanding of care given (e.g. the rationale for using certain communication skills when comforting the dying patient; if the learner understands the why behind the use of these ways of communicating, it indicates that theory underpins practice). • To assess problem solving skills (e.g. by posing: … What’s the real issue here? What other information do you need before you can solve this problem? How else could you … ? Give reasons for …. What would happen if you tried … ? What other options do you have?). • To assess decision-making skills (e.g. by posing: … What action would you take if … ? Give reasons …. What do you intend doing about it?). • It is possible to obtain an indication of underlying attitudes, values and beliefs (e.g. by posing: … What do you think of euthanasia? … detaining psychiatric patients under the Mental Health Act? Do you agree with Jenny’s opinions? Why?). • It is possible to assess verbal communication skills by the ability of the student in verbalizing responses. From the above discussion of the uses of questioning, it can be seen that learning in the cognitive domain and affective domain (Bloom et al 1956) – and thus several attributes of competence – can be assessed using this assessment method. When we assess learning in the cognitive domain, it is important to assess not only the knowledge base but also higher level thinking, so that the range of cognitive skills is assessed. The kinds of questions asked will stimulate different kinds and levels of thinking and the learner will then become aware of the kind and level of thinking expected (Perrott 1982). Formulating questions to assess higher level thinking can be tricky. An understanding of how questions can be classified may assist in the framing of those questions that are necessary to elicit the level of thinking required of the learner. The most popular classification system is based on Bloom’s taxonomy of educational objectives (Bloom et al 1956). Although the taxonomy was developed to classify educational objectives, questions can be related to each level of the taxonomy. Table 4.1, adapted from De Young (1990), lists the cognitive activity at each level, as well as some sample questions. Table 4.1 Question classification according to Bloom’s taxonomy (Adapted with permission from Craig & Page 1981.) With the assistance of the information in Table 4.1, try Activity 4.7. The aim is to structure questions so that they define a linking path, as these are more valuable in assessing the quality of learning and helping the learner to develop higher-level thinking (Minton 1997). Do not be too concerned if you have had difficulties formulating the questions. Many trained teachers manage only to ask questions predominantly at the lower cognitive levels (De Young 1990). In view of the high-level thinking required of health professionals, however, it is beneficial to assess students at the application through to evaluation levels (see Table 4.1). Stoker (1994) says that using questions effectively is an essential skill in assessment. This skill should, and can, be developed. The reader is referred to the chapter on questioning in De Young (1990) for a further discussion of how to frame and ask questions. It is important to remember that, when questioning is used in clinical assessment, the main aim is to gain evidence about how much learning has taken place (i.e. how much of the competency the student has achieved). Questions asked should therefore be related to the competency and be based on the context of the practice event. The following checklist on the use of questioning may be helpful. It builds upon the work of Stoker (1994): • Are the questions relevant to the learner? Do they relate to things the learner needs to know and should know rather than focusing on unusual aspects of the subject? • Are the questions appropriate for the stage of the course of the student? • Is the wording clear? Does it indicate what sort of answer you require? • Have you provided some sort of feedback at the time? Be especially aware of how you deal with incorrect or incomplete answers. Try not to let your reaction have the effect of demotivating the learner. • Be careful not to make learners feel that you are trying to catch them out. The limitations of using questioning for assessing clinical practice are: • Questions cannot assess attitudes, values and beliefs with accuracy, as what the learner says may not be a reflection of inwardly held beliefs. • The learner may feel threatened. This may affect the responses, and an inaccurate picture is formed of the student’s ability. • Inappropriately framed questions may not elicit the correct responses. • Questioning can be time consuming. • It may not have predictive validity. Correct responses to questions may not reflect the ability to perform. As the use of questioning in the clinical setting is frequently related directly to the care-giving experiences of the learner, questioning sessions may lead to a discussion of these instances of practice. It is generally believed that reflection on practice – where the thinking done in one situation is made explicit and built on to be used in another – should be developed through discussion that takes place away from the arena of care activity (Bedford et al 1993). The use of discussions in clinical assessment is now examined. De Young (1990) says that topics that are most suitable for discussion are controversial issues, clinical or professional problems, and emotionally laden topics such as death and dying. After deciding on which clinical event you wish to explore further with the student through discussion, you need to provide some structure for the discussion. De Young (1990:87) made this important point about the use of discussion: ‘Good discussions do not just happen spontaneously; they require careful planning’. She suggests making the following arrangements before you start:
How do we assess?
Introduction
Triangulation
Method triangulation
Data triangulation
Investigator triangulation
Advantages and limitations of triangulation
Advantages
Limitations
Assessment methods
Observation of practice
Using the standards and performance criteria in a checklist
Allow enough time for observation
Advantages of observation of practice
Disadvantages of observation of practice
Questioning
Discussion around care and care activities
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


How do we assess?

Get Clinical Tree app for offline access
