Gender, Socioeconomic, and Cultural Attributes of the Learner
Gender, Socioeconomic, and Cultural Attributes of the Learner
Susan B. Bastable
Deborah L. Sopczyk
CHAPTER HIGHLIGHTS
Gender Characteristics
Cognitive Abilities
Personality Traits
Sexual Orientation and Gender Identity
Socioeconomic Characteristics
Teaching Strategies
Cultural Characteristics
Definition of Terms
Assessment Models for the Delivery of Culturally Sensitive Care
General Assessment and Teaching Interventions
Use of Interpreters
The Four Major Subcultural Ethnic Groups
Hispanic/Latino Culture
Black/African American Culture
Asian/Pacific Islander Culture
American Indian/Alaskan Native Culture
Preparing Nurses for Diversity Care
Stereotyping: Identifying the Meaning, the Risks, and the Solutions
State of the Evidence
KEY TERMS
gender-related cognitive abilities
gender-related personality behaviors
gender gap
gender bias
socioeconomic status (SES)
poverty circle (cycle of poverty)
acculturation
assimilation
cultural awareness
cultural competence
cultural diversity
cultural relativism
culture
ethnic group
ethnocentrism
ideology
subculture
transcultural
worldview
primary characteristics of culture
secondary characteristics of culture
spirituality
religiosity
stereotyping
OBJECTIVES
Afier completing this chapter, the reader will be able to
Identify gender-related characteristics in the learner based on social and hereditary infiuences on brain functioning, cognitive abilities, and personality traits.
Recognize the influence of socioeconomics in determining health status and health behaviors.
Define the various terms associated with diversity.
Examine cultural assessment from the perspective of difierent models of care.
Distinguish between the beliefs and customs of the four predominant ethnic (subcultural) groups in the United States.
Suggest teaching strategies specific to the needs of learners belonging to each of the four ethnic groups.
Examine ways in which transcultural nursing can serve as a framework for meeting the learning needs of various ethnic populations.
Identify the meaning of stereotyping, the risks involved, and ways to avoid stereotypical behavior.
Gender, socioeconomic level, and cultural background have a significant influence on a learner’s willingness and ability to respond to and make use of the teaching-learning situation. These three factors also play a role in how clients experience health and illness and their expectations of the nurse (Core, 2008). Two of these factors—gender and socioeconomic status (SES)—have been given very little attention to date by nurse educators. In contrast, the third factor—cultural and ethnic diversity—has been the focus of considerable study in recent years with respect to its effects on learning. Understanding diversity, particularly those variations among learners related to gender, socioeconomics, and culture, is of major importance when designing and implementing education programs to meet the needs of an increasingly unique population of learners.
This chapter explores how individuals respond differently to healthcare interventions through examination of gender-related variations resulting from heredity or social conditioning that affects how the brain functions for learning. In addition, the influence of environment on the learner from a socioeconomic viewpoint is examined. Consideration is also given to the significant effects that cultural norms have on the behaviors of learners from the perspective of the four major ethnic (subcultural) groups in the United States. Models for cultural assessment and the planning of care are highlighted as well. Finally, this chapter outlines ways to prepare nurses for diversity care and to deal with the issue of stereotyping.
GENDER CHARACTERISTICS
Most of the information on gender variations with respect to learning can be found in the educational psychology and neuroscience literature. Indeed, the nursing literature contains scant information about this subject from a teaching-learning perspective. There are, however, characteristics of male and female orientations that affect learning, which need to be addressed more closely. Two well-established facts exist. First, individual differences within a group of males or females are usually greater than differences between groups of males versus groups of females. Second, studies that compare the sexes seldom are able to separate genetic differences from environmental influences on behavior (Crandell, Crandell, & Vander Zanden, 2012; Santrock, 2011).
There remains a gap in knowledge of what the sexes would be like if humans were not subject to behavioral conditioning. No person can survive outside a social matrix and, therefore, individuals begin to be shaped by their environment right from birth. For example, our U.S. culture exposes girls and boys, respectively, to pink and blue blankets in the nursery, dolls and trucks in preschool, ballet and basketball in the elementary grades, and cheerleading and football in high school. These social influences continue to affect the sexes throughout the life span.
Of course, men and women are different. But the question remains: Are they different or the same when it comes to learning, and to what can the differences and similarities be attributed? Biological and behavioral scientists have, to date, been unable to quantify the exact impact that genetics and environment have on the brain. Opinions are rampant, and research findings are inconclusive.
Traditionally, there has been a great divide between neuroscience and education. What is needed now is multidisciplinary research to bridge the gap in the discoveries being made in cognitive science laboratories and the application of this information to teaching in the real world. To address this need, the National Science Foundation in 2005 pledged $90 million in grants over 5 years to support four teams of cognitive neuroscientists, psychologists, computer scientists, and educationalists to “give the craft of teaching a solid scientific underpinning” (Gura, 2005, p. 1156). By discovering how the brain works in learning, teaching methods and tools can be designed “to complement the brain’s natural development” (p. 1156). This is “a massive effort to put the way children are taught on a sounder scientific footing” (p. 1156).
The fact remains that there are gender differences as to how males and females act, react, and perform in situations affecting every aspect of life (Cahill, 2006). As Cahill contends, the issue of gender influences is much too important to be ignored or marginalized. The National Academy of Sciences reports “sex does matter in ways that we did not expect. Undoubtedly, it matters in ways that we have not yet begun to imagine” (p. 7).
For example, when it comes to human relationships, intuitively women tend to pick up subtle tones of voice and facial expressions, whereas men tend to be less sensitive to these communication cues. In navigation, women tend to have difficulty finding their way, whereas men seem to have a better sense of direction. In cognition, females tend to excel in languages and verbalization, yet men are likely to demonstrate stronger spatial abilities and interest in mathematical problem solving. Scientists are beginning to believe that gender differences have as much to do with the biology of the brain as with the way people are raised (Baron-Cohen, 2005; Gorman, 1992). Kimura (1999), for example, reported on the many different patterns of behavior and cognition between men and women that are thought to reflect varying hormonal influences on brain development.
Some would argue that these examples are representative of stereotyping. Nevertheless, as generalizations, these statements seem to hold some truth. Neuroscientists have begun to detect both structural and functional differences in the brains of males and females. These early findings have led to an upsurge in neuroscience research into the mental lives of men and women (Baron-Cohen, 2005).
Neurobiologists are just at the dawn of understanding how the human brain works, including exactly which types of sensory input wire the brain and how that input affects it. Scientists suspect that cognitive abilities operate much like sensory ones in that they are promoted by those activities and experiences to which a person is exposed right from birth. Circuits in different regions of the brain are thought to mature at different stages of development. These circuits represent critical windows of opportunity at different ages for the learning of math, music, language, and emotion.
Brain development is much more sensitive to life experiences than once believed (Begley, 1996; Hancock, 1996). A baby’s brain is like “a work in progress, trillions of neurons waiting to be wired … to be woven into the intricate tapestry of the mind” (Begley, 1996, pp. 55-56). Some of the neurons of the brain have been hardwired by genes, but trillions more have almost infinite potential and are waiting to be connected by the influence of environment. The first 3 years of life, scientists have realized, are crucial in the development of the mind. The wiring of the brain—a process both of nature and of nurture, dubbed the “dual sculptors”—forms the connections that determine the ability to learn and the interest for learning different types of skills (Harrigan, 2007; Nash, 1997).
Thanks to modern technology, imaging machines are revolutionizing the field of neuroscience. Functional magnetic resonance imaging (fMRI) and positron emission tomography (PET) are being used to observe human brains in the very acts of thinking, feeling, and remembering (Kawamura, Midorikawa, & Kezuka, 2000; Monastersky, 2001; Speck et al., 2000; Yee et al., 2000). Amazing discoveries through brain scanning have been made, such as where the emotion of love resides in the brain. Although machines can measure the brain’s blood flow that supports nerve activity, no machines have been developed to date that can read or interpret a person’s thoughts.
The field of brain scanning still has far to go, but experts consider its potential to be incredible. The trend in current studies is to focus on how separate parts of the brain interact while performing different tasks rather than focusing on only isolated regions of the brain associated with certain tasks (Monastersky, 2001). Researchers have already reported that men and women use different clusters of neurons when they read than when their brains are idling. For example, Kawamura and colleagues (2000) focused on the cerebral localization of the center for reading and writing music of a male patient. They concluded that the left side of the brain is involved in this type of task, just as it is in an individual’s ability to read and write language. Neuroimaging studies also have found that gender makes a difference in brain connectivity (Gong, He, & Evans, 2011).
In addition, gender differences in brain activity during working memory—an important component for performing many higher functions—have been examined with fMRI. For example, in a study of verbal working memory by Speck et al. (2000), the amount of brain activity was found to increase with task difficulty. Interestingly, male subjects demonstrated more right-sided hemispheric dominance, whereas females showed more left-sided hemispheric dominance, with higher accuracy and slightly slower reaction times than their male counterparts. The results revealed significant gender differences in the functional brain’s organization for working memory.
In general, the brains of men and women seem to operate differently. Provocative new studies have revealed that women engage more of their brains when thinking sad thoughts. When men and women subjects were asked to conjure up sad memories, the front of the limbic system in the brain of women glowed with activity eight times more than in men. Although men and women were able to perform equally well in math problems, tests indicated that they seemed to use the temporal lobes of the brain differently to figure out problems. Also, men and women employ different parts of their brains to figure out rhymes. These study results are just a few examples of some of the tentative, yet tantalizing, findings from research that are beginning to show that male and female identity is a creation of both nature and nurture. Along with genetics, life experiences and the choices men and women make over the course of a lifetime help to mold personal characteristics and determine gender differences in the very way the sexes think, sense, and respond (Begley, Murr, & Rogers, 1995).
In comparing how men and women feel, act, process information, and perform on cognitive tests, scientists have been able to identify only a few gender differences in the actual brain structure of humans (Table 8-1). Most differences that have been uncovered are quite small, as measured statistically. Even the largest differences in gender-related cognitive abilities are not as significant as, for example, the disparity found between male and female height. In fact, a great deal of overlap exists in terms of how the brains of the two sexes work. Otherwise, “women could never read maps and men would always be left-handed. That flexibility within the sexes reveals just how complex a puzzle gender actually is, requiring pieces from biology, sociology, and culture” (Gorman, 1992, p. 44).
With respect to brain functioning, a mixture of the factors of heredity and environment likely accounts for gender characteristics. The following is a comparison of cognitive abilities between the genders based on developmental and educational psychology findings in Crandell et al. (2012), Santrock (2011), Snowman, McCown, and Biehler (2012), and Baron-Cohen (2005).
Cognitive Abilities
GENERAL INTELLIGENCE
Various studies have not yielded consistent findings on whether males and females differ in general intelligence. If any gender differences do exist, they seem to be attributed to patterns of ability rather than intelligence quotient (IQ) (Kimura, 1999). When mean differences have been noted, they have proved small. However, what is well documented is the strong correlation between IQ and heredity (Santrock, 2011). On IQ tests during preschool years, girls score higher; in high school, boys score higher on these tests. These differences may be due to higher dropout rates in high school for low-ability boys and gender identity formation in adolescence. Thus overall no dramatic differences between the sexes have been found on measures of general intelligence (Crandell et al., 2012).
Nevertheless, a very interesting trend in IQ scores has been noted. IQs (as measured by the Stanford-Binet intelligence test) are increasing rapidly worldwide. In America, children seem to be getting smarter. As compared with IQs tested in 1932, if people took the same test today, a large percentage would score much higher. Because this increase has occurred over such a relatively short time, heredity cannot be the cause. Instead, increasing levels of education and the information-age explosion likely explain the trend. This increase in IQ scores is known as the Flynn effect after the researcher who discovered it (Santrock, 2011).
TABLE 8-1 Gender Differences in Brain Structure
Men
Women
Temporal Lobe
Regions of the cerebral cortex help to control hearing, memory, and a person’s sense of self and time.
In cognitively normal men, a small region of the temporal lobe has approximately 10% fewer neurons than it does in women.
More neurons are located in the temporal region where language, melodies, and speech tones are understood.
Corpus Callosum
The main bridge between the left and right brain contains a bundle of neurons that carry messages between the two brain hemispheres.
This part of the brain in men takes up less volume than a woman’s does, which suggests less communication between the two brain hemispheres.
The back portion of the callosum in women is bigger than in men, which may explain why women use both sides of their brains for language.
Anterior Commissure
This collection of nerve cells, smaller than the corpus callosum, also connects the brain’s two hemispheres.
The commissure in men is smaller than in women, even though men’s brains are, on average, larger in size than women’s brains.
The commissure in women is larger than in men, which may be a reason why their cerebral hemispheres seem to work together on tasks from language to emotional responses.
Brain Hemispheres
The left side of the brain controls language, and the right side of the brain is the seat of emotion.
The right hemisphere of men’s brains tends to be dominant.
Women tend to use their brains more holistically, calling on both hemispheres simultaneously.
Brain Size
Total brain size is approximately 3 pounds.
Men’s brains, on average, are larger than women’s.
Women have smaller brains, on average, than men because the anatomic structure of their entire bodies is smaller. However, they have more neurons than men (an overall 11%) crammed into the cerebral cortex.
Girls learn to talk, form sentences, and use a variety of words earlier than boys. In addition, girls speak more clearly, read earlier, and do consistently better on tests of spelling and grammar. Originally, researchers believed females performed better than males on measures of verbal fluency, but recent research has questioned this early superiority of females in the verbal domain. On tests of verbal reasoning, verbal comprehension, and vocabulary, the findings are not consistent. The conclusion is that no significant gender differences in verbal ability exist.
MATHEMATICAL ABILITY
During the preschool years, there appear to be no gender-related differences in ability to do mathematics. By the end of elementary school, however, boys show signs of excelling in mathematical reasoning, and the differences in math abilities of boys relative to girls become even greater in high school. Recent studies reveal that any male superiority likely is related to the way math is traditionally taught—as a competitive individual activity rather than as a cooperative group learning endeavor.
When the approach to teaching math is taken into consideration, only about a 1% variation in quantitative skills is seen in the general population. In our culture, math achievement differences may result from different role expectations. The findings on math ability and achievement can also be extended to science ability and achievement, as these two subjects are related.
SPATIAL ABILITY
The ability to recognize a figure when it is rotated, to detect a shape embedded in another figure, or to accurately replicate a three-dimensional object has consistently been found to be better among males than among females. Of all possible gender-related differences in cognitive activity, the spatial ability of males is consistently better than that of females and probably has a genetic origin. Rubin Gur, a noted researcher on gender differences in the brain, concurs with other research findings pointing out that men do perform better on spatial tasks than women (Gur et al., 2000). However, the magnitude of this sex difference accounts for only about 5% of the variation in spatial ability.
Interestingly, women surpass men in the ability to discern and later recall the location of objects in a complex, random pattern (Kimura, 1999). Scientists have reasoned that historically men may have developed strong spatial skills so as to be successful hunters, whereas women may have needed other types of visual skills so as to excel as gatherers and foragers of food (Gorman, 1992).
PROBLEM SOLVING
The complex concepts of problem solving, creativity, analytical skill, and cognitive styles, when examined, have led to mixed findings regarding gender differences. Men tend to try new approaches in problem solving and are more likely to be field independent—that is, they are less influenced by irrelevant cues and more focused on common features in certain learning tasks. Males also show more curiosity and significantly less conservatism than women in risk-taking situations. In the area of human relations, however, women perform better at problem solving than do men.
SCHOOL ACHIEVEMENT
Without exception, girls get better grades on average than boys, particularly at the elementary school level. Scholastic performance of girls is more stable and less fluctuating than that of boys.
Although no compelling evidence proves significant gender-linked differences in the areas of cognitive functioning, except in spatial ability, some findings do reveal sex differences when it comes to personality characteristics. Evidence reported by Crandell et al. (2012), Santrock (2011), and Snowman et al. (2012) was used to substantiate the following summary findings unless otherwise noted.
Personality Traits
Most of the observed gender-related personality behaviors are thought to be largely determined by culture but are, to some extent, a result of mutual interaction between environment and heredity.
AGGRESSION
Males of all ages and in most cultures are generally more aggressive than females (Baron-Cohen, 2005). The role of the gender-specific hormone testosterone has been cited as a possible cause of the more aggressive behavior demonstrated by males (Kimura, 1999). However, anthropologists, psychologists, sociologists, and scientists in other fields continue to disagree about whether aggression is biologically based or environmentally influenced. Nevertheless, male and female roles differ widely in most cultures, with males usually being more dominant, assertive, energetic, active, hostile, and destructive.
CONFORMITY AND DEPENDENCE
Females have been found generally to be more conforming and more influenced by suggestion. The gender biases of some studies have left these findings open to suspicion, however.
EMOTIONAL ADJUSTMENT
The emotional stability of the sexes is approximately the same in childhood, but differences do arise in how emotional problems are manifested. Some evidence indicates that adolescent girls and adult females have more neurotic symptoms than males. However, this tendency may reflect how society defines mental health in ways that coincide with male roles. In addition, tests to measure mental health usually have been designed by men and, therefore, may be biased against females.
VALUES AND LIFE GOALS
In the past, men have tended to show greater interest in scientific, mathematical, mechanical, and physically active occupations as well as to express stronger economic and political values. Women have tended to choose literary, social service, and clerical occupations and to express stronger aesthetic, social sense, and religious values. These differences have become smaller over time, however, as women have begun to think differently about themselves, women have more freely pursued career and interest pathways, and society has begun to take a more equal opportunity viewpoint for both sexes.
ACHIEVEMENT ORIENTATION
Females are more likely to express achievement motivation in social skills and social relations, whereas men are more likely to try to succeed in intellectual or competitive activities. This difference is thought to reflect sex-role expectations that are strongly communicated at very early ages.
How do the preceding observations on gender characteristics in intellectual functioning and personality relate to the process of teaching clients whom the nurse as educator encounters? It is very difficult to differentiate between biological and environmental influences simply because these two factors are intimately intertwined and influence each other. The cause, meaning, and outcome of these differences remain speculative at this time, and further research needs to be conducted.
The behavioral and biological differences between males and females, known as the gender gap, are well documented. Also well documented is gender bias, “a preconceived notion about the abilities of women and men that prevented individuals from pursuing their own interests and achieving their potentials” (Santrock, 2006, p. 66). Females have an accelerated biological timetable and, in general, are more prone to demonstrate early verbal ability. Conversely, males lag behind females in biological development and attention span but tend to excel in visual-spatial ability and mathematical pursuits (Crandell et al., 2012). During adolescence, they also are likely to surpass females in physical strength.
With respect to gender differences and aging, as suggested by current life-span mortality rates, White females have a life expectancy of approximately 80 years compared to approximately 73 years for White males. Also, men have higher mortality rates for each of the 10 leading causes of death (U.S. Department of Health and Human Services [USDHHS], 2009). However, more needs to be understood about women’s health, because for years their health issues have been underrepresented in research studies. Fortunately, this trend has changed within the last two to three decades, and significant evidence is beginning to surface about the physical and mental health status of females (Dignam, 2000; Kato & Mann, 1996; USDHHS, 2012).
One point that is known is that women are likely to seek health care more often than men do (U.S. Census Bureau, 2006). It is suspected that one of the reasons women have more contact with the healthcare system is that they traditionally have tended to be the primary caretakers of their children, who need pediatric services. In addition, during their childbearing years, women seek health services for care surrounding pregnancy and childbirth (Kato & Mann, 1996).
Perhaps the reason that men tend not to rely as much as women on care from health providers is because of the sex-role expectation by our society that men should be stronger. They also have a tendency to be risk takers and to think of themselves as more independent. Although men are less likely to pursue routine health care for purposes of health and safety promotion and disease and accident prevention, they typically face a greater number of health hazards, such as a higher incidence of automobile accidents, use of drugs and alcohol, suicide, heart disease, and participation in dangerous occupations. Furthermore, men are less likely to notice symptoms or report them to physicians (Kato & Mann, 1996).
Sexual Orientation and Gender Identity
The exact number of lesbian, gay, bisexual, and transgender (LGBT) individuals in the United States and around the world is unknown; however, this population is estimated to include more than 8 million people in the United States alone (Fenway Institute, 2010a). This number is based on U.S. Census data and represents a very conservative estimate of the LGBT population. Although the U.S. Census does gather information on samesex couples, it does not ask questions about sexual orientation or gender identity (Gates, 2010). Therefore, single gays and lesbians are not identified in U.S. Census data, nor are members of the transgender community. Because of hesitancy on the part of many members of the LGBT population to disclose their sexual preference and/or gender identity, underrepresentation is always an issue.
Lack of representation of the LGBT community is not restricted to the U.S. Census. Because questions about sexual preference or gender identity are not included on many health surveys, the LGBT population is also underrepresented in health research (National Coalition for LGBT Health, 2009; Sexual Minority Assessment Research Team, 2009). In an effort to rectify some of these issues, the Institute of Medicine (IOM) convened a panel to write the federal government’s first report about the health issues of the LGBT community. The IOM report will explore the state of the science on LGBT health and outline a research agenda that will assist the National Institutes of Health in directing research in this area (Institute of Medicine of the National Academies, 2010). Furthermore, World Voices for Equality, a nonprofit corporation, completed the first worldwide LGBT census in December 2012 (LGBT Census, 2013).
When considering gender and the social and other factors that influence the unique learning styles and educational needs of men and women, it is important to include the LGBT community. The LGBT population represents a distinct cultural group whose needs are often overlooked by nurses and other health professionals. Although members of the LGBT population have many of the same health problems as do the general population, disparities do exist, and as a group, their health outcomes are worse than those of the heterosexual community (Centers for Disease Control and Prevention [CDC], 2010; Krehely, 2009).
Three main problems contribute to the health disparities experienced by the LGBT population:
1. The social stigma associated with being LBGT creates undue stress and contributes to negative health behavior patterns. For example, research has identified increased rates of tobacco, alcohol, and drug use among the LGBT population as well as a high incidence of depression, anxiety, and other mental health problems (Woodiel & Brindle, 2008).
2. Structural barriers decrease access to health care for people who are LGBT (Mayer et al., 2008). For example, unemployment in the LGBT community resulting from job discrimination and lack of insurance benefits for same-sex domestic partners have led to a higher than average number of people without health insurance coverage (Krehely, 2009).
3. Lack of culturally appropriate care for the LGBT community results in limited or ineffective use of healthcare services. For example, in an attempt to avoid negative interactions with healthcare providers, LGBT clients—particularly bisexual men and women—are often reluctant to disclose their sexual preference or gender identity. Without this vital piece of information, nurses and other health professionals are unable to provide comprehensive care. Other members of the LGBT community simply avoid seeking health care unless absolutely necessary. As a result, they may not take advantage of preventive services or receive early treatment for serious health problems (Durso & Meyer, 2012; McRae, Ochsner, Mauss, Gabrieli, & Gross, 2008).
Although bias and misunderstanding remain, in recent years there has been greater awareness and acceptance of the LGBT lifestyle in the United States. Thanks to the national efforts of organizations such as the National Coalition for LGBT Health, the Williams Institute of the University of California-Los Angeles (UCLA) School of Law, and the Fenway Institute, tremendous efforts have been made in health-related public policy, research, and public and professional education. Also, local groups have been active in advocating for the needs of the LGBT community. Particular emphasis has been placed both at the local and national levels on educating nurses and other health professionals in an attempt to improve LGBT health services (McLees, 2010). For example, the Fenway Institute published the first medical textbook on LGBT health and offers learning modules for health professionals on its website (Fenway Institute, 2010a).
TEACHING STRATEGIES
Davidson, Trudeau, van Roosmalen, Stewart, and Kirkland (2006) describe gender as a “multifaceted construct” (p. 731) that includes a number of modifiable attributes that influence health outcomes and health education. These attributes include personality, social supports, coping skills, values, and health-related behaviors. When planning teaching strategies, nurses must be aware of the extent to which attributes such as these as well as heredity-related characteristics of the genders affect health-seeking behaviors and influence individual health needs. As stated previously, in some areas males and females display different orientations and learning styles (Severiens & Ten Dam, 1994). The precise differences seem to depend on interests and past experiences in the biological and social roles of men and women in American society.
Women and men are part of different social cultures, too. They use different symbols, belief systems, and ways to express themselves, much in the same manner that different ethnic groups exhibit distinct cultures (Tear, 1995). In the future, these gender differences may become less pronounced as the sex roles become more blended. Symbols are also very important to the LGBT community, with the most commonly employed being the pink triangle and the rainbow pride flag. These symbols are used by the LGBT community as a show of pride and unity. In addition, some health professionals display these symbols as a sign of welcome to LGBT clients (Woodiel & Brindle, 2008).
When serving in the role of educator, nurses must create an environment that is welcoming to all men and women regardless of lifestyle. Clients, particularly those living alternative lifestyles, look for subtle clues to determine whether the nurse will accept them without judgment (Woodiel & Brindle, 2008). For example, a women’s or children’s health clinic that displays photos of only traditional families may give the message that nontraditional families are not welcome. Brochures on LGBT health issues and unisex bathrooms are all strategies that give a welcoming message to a diverse client base.
When working with men and women, it is important that the nurse educator avoid making assumptions about family structure, sexual preference, or lifestyle. Many families in the 21st century are structured differently from how families were structured in years past. For example, more men are assuming primary responsibility for child care. The nurse should never assume that a client is heterosexual, even if that person is or has been married to a member of the opposite sex, as almost half of self-identified lesbians have been or are currently married (Fenway Institute, 2010b).
To complete an accurate assessment of each client, the nurse educator should take every opportunity to gather accurate information from the client. Admission or intake forms are often designed for the traditional family. Clients are often not given an opportunity to identify a same-sex domestic partner. Transgender clients are usually forced to select either male or female. By adjusting the forms to be more inclusive, the nurse not only creates a welcoming environment but also offers an opportunity for the client to share important information.
One of the four major goals of Healthy People 2020 is to eliminate health disparities among segments of the population. This includes differences that occur by gender, such as the facts that men are two times more likely to die from injuries than are women, and women are at greater risk for Alzheimer’s disease and two times as likely to be affected by depression as are men (USDHHS, 2012). When considering health disparities that occur by gender, it is also important to consider differences among the LGBT population, such as transgender adults being 10 times more likely to suffer suicidal ideation and LGBT youth being twice as likely to be overweight (Krehely, 2009).
Nurses are encouraged to include information on general health disparities when educating clients and staff. They also are encouraged to use versatile teaching-style strategies so as not to perpetuate stereotypical approaches to teaching and learning with the two genders. In addition, nurses have a responsibility to incorporate gender issues into nursing curricula (McLees, 2010).
SOCIOECONOMIC CHARACTERISTICS
Socioeconomic status (SES), in addition to gender characteristics, influences the teaching-learning process. SES is considered to be the single most important determinant of health in our society (Crimmins & Saito, 2001; Singh-Manoux, Ferrie, Lynch, & Marmot, 2005). Socioeconomic class is an aspect of diversity that must be addressed in the context of education and in the process of teaching and learning.
Class has been described as the “unmentionable five-letter word” (Rhem, 1998, p. 1). Many people are hesitant to categorize themselves according to class. They also are reluctant to discuss the issue of class differences because of the widespread idea that the United States should be a classless society (Felski, 2002; Rhem, 1998). It is a myth, though, that America is a country without classes (McGoldrick, 1995). Class, as universal as race or gender, hides in the shadows. However, class consciousness seems to be a commonality shared by everyone. Those who are privileged often feel guilty about their advantages; those who are poor feel ashamed or embarrassed about their disadvantages (Rhem, 1998).
Social and economic levels of individuals have been found to be significant variables affecting health status, literacy levels, and health behaviors (Crimmins & Saito, 2001; Monden, van Lenthe, & Mackenbach, 2006). Approximately 46.2 million Americans (15% of the total population) live in poverty. The poverty threshold for a family of four is defined as an income of $23,021 per year, while severe poverty is an annual income of at most half ($11,500) of this amount (U.S. Census Bureau, 2011b).
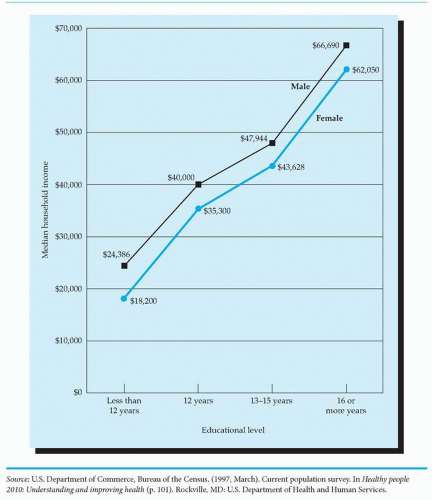
Disadvantaged people—those with low incomes, low educational levels, or social deprivation —come from many different ethnic groups, with their number including millions of poor White people (USDHHS, 2012). SES takes into account the variables of educational level, family income, and family structure (Crandell et al., 2012). Figure 8-1 highlights the relationship between educational level and household income. Collectively, all of these variables influence health beliefs, health practices, and readiness to learn (Darling, 2004; Mackenbach et al., 2003).
The relationships among socioeconomic position, cognitive ability, and health status have been explored to some extent, but the mechanics and processes involved are highly complex and remain poorly understood (Batty, Der, Macintyre, & Deary, 2006; Singh-Manoux et al., 2005). Heredity and environment usually vary together; that is, people who are genetically related (parents and their children) tend to have similar environments. Evidence suggests that variations in heredity are equally as powerful as variations in environmental conditions in producing individual differences in cognitive ability (Crandell et al., 2012; Santrock, 2011; Turkheimer, Haley, Waldron, D’Onofrio, & Gottesman, 2003). Also, low socioeconomic class is correlated with low educational levels and health inequalities (Mackenbach, Cavelaars, Kunst, Groenhof, & EU Working Group on Socioeconomic Inequalities in Health, 2000).
Although many educators, psychologists, and sociologists have recognized that a cause-ande ffect relationship exists among low SES, low cognitive ability, and poor quality of health and life, they are hard pressed to suggest solutions for breaking this cycle (Batty, Deary, & Macintyre, 2006). Likewise, nurses well recognize that clients belonging to lower social classes have higher rates of illness, more severe illnesses, and reduced rates of life expectancy (Mackenbach et al., 2003). People with low SES, as measured by indicators such as income, education, and occupation, have increased rates of morbidity and mortality compared to those with higher SES (USDHHS, 2012).
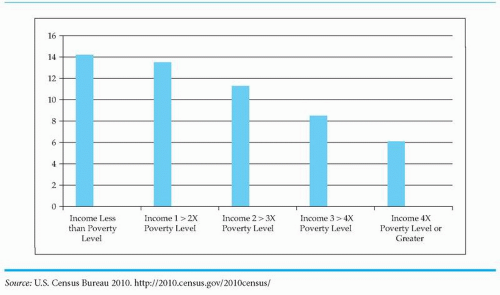
An inverse relationship exists between SES and health status. Individuals who have higher incomes and are better educated live longer and healthier lives than those who are of low income and poorly educated (Crimmins & Saito, 2001; Rognerud & Zahl, 2005). Thus the level of socioeconomic well-being is a strong indicator of health outcomes. Figure 8-2 illustrates the relationship between SES and health status.
FIGURE 8-1 Relationship between education and median household income among adults aged 25 years and older, by gender, United States, 1996.
These findings raise serious questions about health differences among people of the United States as a result of unequal access to health care due to SES. These unfortunate health trends are costly to society in general and to the healthcare system in particular. Although adverse health-related behavior and less access to medical care have been found to contribute to higher morbidity and mortality rates, there is newer but still limited research on the effect SES has on disability-free or active life expectancy (Crimmins & Saito, 2001; Mackenbach et al., 2003).
FIGURE 8-2 Percentage of persons with perceived fair to poor health status by income level.
Social class is measured by one or more of the following types of indices:
Occupation of parents
Income of family
Location of residence
Educational level of parents
Crandell et al. (2012) and Santrock (2011) explain that many factors, including poor health care, limited resources, family stress, discrimination, and low-paying jobs, maintain the cycle by which generation after generation is born into poverty. Elstad and Krokstad (2003) found that health inequalities as a result of socioeconomic factors are reproduced as people mature from young adulthood into middle age. That is, a social causation pattern exists whereby environments are the source of socioeconomic health inequalities. As such, people with good health tend to move up in the social hierarchy, whereas those with poor health move downward.
In addition, rates of illiteracy and low literacy have been linked to poorer health status, high unemployment, low earnings, and high rates of welfare dependency, all of which are common measures of a society’s economic well-being (Giorgianni, 1998; Weiss, 2003). Whatever the factors that keep particular groups from achieving at higher levels, these groups are likely to remain on the lower end of the occupational structure. This cycle has been coined the poverty circle (Gage & Berliner, 1998) or the cycle of poverty. The poverty circle is described as follows:
Parents low in scholastic ability and consequently in educational level create an environment in their homes and neighborhoods that produce children who are also low in scholastic ability and academic attainment. These children grow up and become parents, repeating the cycle. Like them, their children are fit only for occupations at lower levels of pay, prestige, and intellectual demand. (Gage & Berliner, 1998, p. 61)
Family structure and the home environment are not the only factors affecting proficiency in learning. Hirsch (2001), for example, contends that the alarming verbal and reading gap between rich and poor students “represents the single greatest failure in American public schooling” (p. 5). Many low-income children entering kindergarten have heard only half the words and understand only half the meanings of language than the high-income child has heard and understands. This gap continues to widen along the same trajectory as students progress in each succeeding grade in school. Barriers to equal educational opportunity must be reduced by putting the responsibility on the educational system to become more intensive. That is, we need to develop standards for each grade and make sure each child meets these expectations before being allowed to progress to subsequent grades in school.
The lower socioeconomic class has been studied by social scientists more than other economic classes. This research focus probably arises because the health views of this group deviate the most from the viewpoints of the health professionals who care for this group of individuals. People from the lower social stratum have been characterized as being indifferent to the symptoms of illness until poor health interferes with their lifestyle and independence. Their view of life is one of a sense of powerlessness, meaninglessness, and isolation from middle-class knowledge of health and the need for preventive measures, such as vaccination for their children (Lipman, Offord, & Boyle, 1994; USDHHS, 2012; Winkleby, Jatulis, Frank, & Fortmann, 1992).
The high cost of health care may well be a major factor affecting health practices of people in the lower socioeconomic classes. Individuals with adequate financial and emotional resources are able to purchase services and usually have support systems on which to rely to sustain them during recovery or augment their remaining functions after the course of an acute illness. Conversely, individuals deprived of monetary and psychosocial resources are at a much greater risk for failing to reach an optimal level of health and well-being. Unfortunately, the number of Americans at or below the national poverty level is at close to 15%. Approximately 17.4% of Americans lack health insurance of any kind, and another 15.7% are covered by Medicaid. Of those individuals who have no insurance or are covered by Medicaid, only 15% report being in excellent health, as opposed to 85% of individuals who hold private insurance (O’Hara & Caswell, 2012).
Just as SES can have a negative effect on illness, so, too, can illness have devastating implications for a person’s socioeconomic well-being (Elstad & Krokstad, 2003). A catastrophic or chronic illness can lead to unemployment, loss of health insurance coverage or ineligibility for health insurance benefits, enforced social isolation, and a strain on social support systems (Lindholm, Burstrom, & Diderichsen, 2001; Mulligan, 2004). Without the socioeconomic means to counteract these threats to their well-being, impoverished individuals may be powerless to improve their situation.
These multiple losses tax the individual, their families, and the healthcare system. Low-income groups are especially affected by changes in federal and state assistance in the form of Medicare and Medicaid. The spiraling costs associated with illness and consequent overuse of the healthcare system have resulted in increased interest on the part of the public and healthcare providers to control costs (Carpenter, 2011). Today, more emphasis is being given to health promotion, health maintenance, and disease prevention.
Teaching Strategies
The current trends in health care, as a result of these economic concerns, are directed toward teaching individuals how to attain and maintain health. The nurse plays a key role in educating the consumer about avoiding health risks, reducing illness episodes, establishing healthful environmental conditions, and accessing healthcare services. Educational interventions by nurses for those individuals who are socially and economically deprived have the potential to yield short-term benefits in meeting these individuals’ immediate healthcare needs. However, more research must be done to determine whether teaching can ensure the long-term benefits of helping deprived people develop the skills needed to reach and sustain independence in self-care management.
Nurse educators must be aware of the probable effects of low SES on an individual’s ability to learn as a result of suboptimal cognitive functioning, poor academic achievement, low literacy, high susceptibility to illness, and disintegration of social support systems. Low-income people are at greater risk for these factors, all of which can interfere with learning. Stress hormones caused by poverty, for example, have been shown to “poison the brain for a lifetime” (Krugman, 2008). However, nurses cannot assume that everyone at the poverty or near-poverty level is equally influenced by these threats to their well-being. To avoid stereotyping, it is essential that each individual or family be assessed to determine their particular strengths and weaknesses for learning. In this way, teaching strategies unique to particular circumstances can be designed to assist socioeconomically deprived individuals in meeting their needs for health care.
Nevertheless, it is well documented that individuals with literacy problems, poor educational backgrounds, and low academic achievement are likely to have low self-esteem, feelings of helplessness and hopelessness, and low expectations. They also tend to think in concrete terms, are more focused on satisfying immediate needs, have a more external locus of control, and have decreased attention spans. They have difficulty in problem solving and in analyzing and synthesizing large amounts of information. With these individuals, the nurse educator will most likely have to rely on specific teaching methods and tools similar to those identified as appropriate for intervening with clients who have low literacy abilities.
CULTURAL CHARACTERISTICS
The racial makeup of the United States continues to undergo change. At the beginning of the 21st century, the composition of the U.S. population was approximately 71.3% non-Hispanic White and 28.7% minority. By 2012, minority representation in the country grew to 37%. It is anticipated that the minority population will continue to grow and more than double in the next 50 years. By 2043, it is projected that there will be no majority group in the United States and that by 2060, with more than 241.3 million people, minority groups will constitute 57% of the U.S. population (U.S. Census Bureau, 2012).
To keep pace with a society that is becoming increasingly more culturally diverse, nurses need to have sound knowledge of the cultural values and beliefs of specific ethnic groups as well as be aware of individual practices and preferences (Price & Cortis, 2000; Purnell, 2013). In the past, nurses have experienced difficulties in caring for clients whose cultural beliefs differed from their own because beliefs about health and illness vary considerably among ethnic groups. Lack of cultural sensitivity by nurses and other healthcare professionals has resulted in millions of dollars wasted annually through misuse of healthcare services, the alienation of large numbers of people, and the misdiagnosis of health problems with often tragic and dangerous consequences.
In addition, underrepresented ethnic groups are beginning to demand culturally relevant health care that respects their cultural rights and incorporates their specific beliefs and practices into the care they receive. This expectation is in direct conflict with the unicultural, Western, biomedical paradigm taught in many nursing and other healthcare provider programs across the country (Purnell, 2013). A serious conceptual problem exists within the nursing profession because nurses are presumed to understand and be able to meet the healthcare needs of a culturally diverse population, even though they do not have the formal educational preparation to do so (Boss, 2007; Carthron, 2007).
Definition of Terms
Before examining the major ethnic (subcultural) groups within the United States, it is imperative to define the following terms, as identified by Purnell (2013), that are commonly used in addressing the subject of culture:
Acculturation: A willingness to adapt or “to modify one’s own culture as a result of contact with another culture” (p. 481).
Assimilation: The willingness of an individual or group “to gradually adopt and incorporate characteristics of the prevailing culture” (p. 481).
Cultural awareness: Recognizing and appreciating “the external signs of diversity” in other ethnic groups, such as their art, music, dress, and physical features (p. 482).
Cultural competence: Possession of the “knowledge, abilities, and skills to deliver care congruent with the patient’s cultural beliefs and practices” (p. 7).
Cultural diversity: A term used to describe the varieties of cultures that exist within society.
Cultural relativism: “The belief that the behaviors and practices of people should be judged only from the context of their cultural system” (p. 482).
Culture: “The totality of socially transmitted behavioral patterns, arts, beliefs, values, customs, lifeways, and all other products of human work and thought characteristic of a population of people that guide their worldview and decision making. These patterns may be explicit or implicit, are primarily learned and transmitted within the family, and are shared by the majority of the cultures” (p. 482).
Ethnic group: Also referred to as a subculture; a population of “people who have experiences different from those of the dominant culture” (p. 483).
Ethnocentrism: “The tendency of human beings to think that [their] own ways of thinking, acting, and believing are the only right, proper, and natural ones and to believe that those who differ greatly are strange, bizarre, or unenlightened” (p. 483).
Ideology: “The thoughts, attitudes, and beliefs that reflect the social needs and desires of an individual or ethnocultural group” (p. 484).
Subculture: A group of people “who have had different experiences from the dominant culture by status, ethnic background, residence, religion, education, or other factors that functionally unify the group and act collectively on each other” (p. 486).
Transcultural: “Making comparisons for similarities and differences between cultures” (p. 8).
Worldview: “The way individuals or groups of people look at the universe to form values about their lives and the world around them” (p. 487).
ASSESSMENT MODELS FOR THE DELIVERY OF CULTURALLY SENSITIVE CARE
Given increases in immigration and birth rates in the United States as well as the significant increased geographical mobility of people around the globe, the U.S. system of health care and this country’s educational institutions must respond by shifting from a dominant monocultural, ethnocentric focus to a more multicultural, transcultural focus (Narayan, 2003).
Tripp-Reimer and Afifi (1989) describe the interpretation of American cultural ideal from a historical perspective:
In the United States, the myth of the melting pot emerged largely from a combination of a cultural ideal of equality and a European ethnocentric perspective. This myth promoted the notion that all Americans are alike—that is, like white, middle-class persons. For many years, the notion that ethnicity should be discounted or ignored was prominent in the delivery of health care, including health teaching programs … (p. 613)
The question posed by Leininger (1994) remains relevant today: How can nurses competently respond to and effectively care for people from diverse cultures who act, speak, and behave in ways different than their own? Studies indicate that nurses are often unaware of the complex factors influencing clients’ responses to health care.
From a sociological perspective, the symbolic interaction theory provides a theoretical framework for interacting with ethnic groups. It emphasizes social and group identities rather than just individual identity. Tashiro (2002) points out that this framework is useful for understanding the situational nature of identity and the negotiation and renegotiation necessary when working with groups.
Purnell (2013) has proposed that a number of factors influence an individual’s identification with an ethnic group and cause the individual to share his or her worldview. These factors may be distinguished as primary and secondary characteristics of culture. Primary characteristics of culture include nationality, race, color, gender, age, and religious affiliation. Secondary characteristics of culture include many of a person’s attributes that are addressed in this chapter and this text, such as SES, physical characteristics, educational status, occupational status, and place of residence (urban versus rural). These two major characteristics affect one’s worldview and belief system.
The Purnell model for cultural competence represents a popular organizing framework for understanding the complex phenomena of culture and ethnicity. This framework “provides a comprehensive, systematic, and concise” approach that can assist healthcare providers in teaching students in educational settings and clients and staff in practice settings for the delivery of “holistic, culturally competent, therapeutic interventions” (Purnell, 2013, p. 15).
The Purnell model, depicted in a circle format, includes the macro layers of the following metaparadigm concepts:
1. Global society (outermost sphere)
2. Community (second sphere)
3. Family (third sphere)
4. Individual (innermost sphere)
The interior of the circle is cut into 12 equally sized, pie-shaped wedges that represent cultural domains that should be assessed when planning for educational interventions for clients in any setting:
1. Communication (e.g., dominant language and nonverbal expressions and cues)
2. Family roles and organization (e.g., head of household, gender roles, developmental tasks, social status, alternative lifestyles, roles of older adults)
3. Workforce issues (e.g., language barriers, autonomy, acculturation)
Purnell has also identified 19 explicit assumptions upon which the model is based, some of which are most pertinent to this chapter:
One culture is not better than another—they are just different.
The primary and secondary characteristics of culture determine the degree to which one varies from the dominant culture.
Culture has a powerful influence on one’s interpretation of and responses to health care.
Each individual has the right to be respected for his or her uniqueness and cultural heritage.
Prejudices and biases can be minimized with cultural understanding.
Caregivers who intervene in a culturally competent manner improve the care of clients and their health outcomes.
Cultural differences often require adaptations to standard professional practices.
Other models for conducting a nursing assessment have also been proposed. Giger and Davidhizar’s (2004) model includes six cultural phenomena that need to be taken into account: (1) communication, (2) personal space, (3) social organization, (4) time, (5) environmental control, and (6) biological variations (Figure 8-3). Price and Cordell’s (1994) model outlines a four-step approach to help nurses provide culturally sensitive patient teaching (Figure 8-4).
Only gold members can continue reading. Log In or Register to continue