The gastrointestinal (GI) system is comprised of the alimentary canal and its accessory organs. The alimentary canal begins at the mouth and extends through the pharynx, esophagus, stomach, small intestine, colon, and rectum, and ends at the anus. The accessory organs include the teeth, salivary glands, liver, pancreas, and spleen.
The functions of the GI system include ingestion and propulsion of food; mechanical and chemical digestion of food; synthesis of nutrients, such as vitamin K; absorption of nutrients into the bloodstream; and the storage and elimination of nondigestible waste products from the body through feces.
A comprehensive health history should be obtained to elicit subjective data related to major manifestations of GI problems. Common manifestations include nutritional problems, abdominal pain, indigestion, nausea, vomiting, diarrhea, constipation, bloody bowel movements, change in bowel habits, weight loss, and dysphagia.
STANDARDS OF CARE GUIDELINES 18-1
Gastrointestinal Dysfunction
When caring for a patient after abdominal surgery or with any type of GI disorder:
Make sure that adequate bowel sounds are present before allowing anything by mouth. Periodically reassess for bowel sounds, bloating, nausea, vomiting, and abdominal distension or tenderness.
Monitor food/fluid intake and output as indicated.
Periodically monitor weight, and watch for trend in weight loss or weight gain.
Assess stools for frequency, consistency, color, and amount.
Report increase in pain, fever, nausea, vomiting, bloating, change in stools, or signs of wound infection to health care provider promptly.
Monitor complete blood count, electrolytes, albumin, and protein as directed.
This information should serve as a general guideline only. Each patient situation presents a unique set of clinical factors and requires nursing judgment to guide care, which may include additional or alternative measures and approaches.
Nutritional Problems
Characteristics: What is your typical 24-hour food intake? What is your usual weight? Has there been a recent weight gain or loss? If a recent weight change, how many pounds and over what time period? How is your appetite?
Associated factors: Explore other factors that may influence weight changes—food preferences; family/individual routines associated with eating; cultural and religious values; psychological factors, such as depression, anxiety, stress; physical factors, such as activity level, health status, dental problems, allergies; access/transportation to grocery stores; eating habits, self-imposed dietary restrictions; body image; nutritional knowledge; finances.
History: Any history of eating disorders? Any family history of ulcer, GI cancer, inflammatory bowel disease, obesity?
Abdominal Pain
Characteristics: Can you describe the pain (sharp, dull, superficial, or deep)? Is the pain intermittent or continuous? Was the onset sudden or gradual? Can you point to where the pain is located? What makes the pain better, worse?
Associated factors: Are there other symptoms associated with the pain—fever, chills, night sweats, nausea, vomiting, diarrhea, constipation, anorexia, weight loss, dyspepsia, black tarry stools or blood in the stool?
History: Any family history of GI cancer, ulcer disease, inflammatory bowel disease? Any previous history of tumors, malignancy, ulcers?
Indigestion (Dyspepsia)
Characteristics: Have you experienced any of the following symptoms—a feeling of fullness, heartburn, excessive belching, flatus, nausea, a bad taste, mild or severe pain? How is your appetite? If pain or tenderness, where is it located? Does the pain radiate to any other areas? What precipitating factors are associated with the pain? What makes the symptoms better, worse? Are the symptoms associated with food intake? If associated with food, the amount and type?
Associated factors: Is there nausea, vomiting, dysphagia, blood in bowel movements, or diarrhea? Is there a history of alcohol, nonsteroidal anti-inflammatory drug (NSAID), bisphosphonate, or aspirin use?
History: Any family history of cancer, inflammatory bowel disease? Any history of bowel obstruction? Any previous abdominal surgeries?
Nausea and Vomiting
Characteristics: Is the nausea or vomiting associated with certain stimuli, such as specific foods, odors, activity, or a certain time of day? Does it occur before or after food intake? How many times per day does vomiting occur? What specific fluids/foods can be tolerated when vomiting occurs? What is the amount, color, odor, and consistency of the vomitus (see Table 18-1)?
Associated factors: Is there fever, headache, dizziness, weakness, or diarrhea? Missed menstrual period? Any weight loss? Any new medications? Any psychological stress, depression, or emotional problems?
History: Any history of gallbladder disease? Ulcer disease? GI cancer? Unprotected intercourse?
Diarrhea
Characteristics: How long has the diarrhea been present? Determine the frequency, consistency, color, quantity, and odor of stools. Are there blood, mucus, pus, or food particles in the stools? Does this represent a change in bowel habits? Any nocturnal diarrhea? What makes the diarrhea worse, better? Any associated weight loss? (see Box 18-1).
Associated factors: Any fever, nausea, vomiting, abdominal pain, abdominal distention, flatus, cramping, urgency with straining? Is the patient taking antibiotics? Has there been any recent travel to foreign countries? (Mexico, South America, Africa, and Asia are countries with the highest risk of traveler’s diarrhea.) Is the patient experiencing emotional stress or anxiety? Are there any recently prescribed medications?
History: Is there a history of celiac disease, colon cancer, ulcerative colitis, Crohn’s disease, malabsorption syndrome? Has the patient undergone surgery recently (eg, bariatric surgery)?
Table 18-1 Nature of Vomitus
COLOR/TASTE/CONSISTENCY
POSSIBLE SOURCE
Yellowish or greenish
• May contain bile
• Medication—senna
Bright red (arterial)
• Hemorrhage, peptic ulcer
Dark red (venous)
• Hemorrhage, esophageal or gastric varices
“Coffee grounds”
• Digested blood from slowly bleeding gastric or duodenal ulcer
Obtain history of over-the-counter (OTC), herbal, or “natural” products the patient may be taking. Ginger is commonly used as an antiemetic and, although generally safe, it can cause heartburn. Licorice root is used for upset stomach and to soothe ulcers, but can cause sodium and fluid retention and loss of potassium. Goldenseal is used as an antidiarrheal, but can cause a number of adverse reactions, including skin and mucous membrane irritation, interference with anticoagulation, and cardiac and nervous system excitability. Also, many herbs can impair absorption of other medicines. Remind patients that herbal products are not found naturally in the body or in significant amounts in the daily diet, so should be treated like drugs.
Constipation
Characteristics: What is the frequency, consistency, color of the stools? Is this a change in bowel habits? If a change, has this been gradual or sudden? What is the size of the stools? Have there been dietary changes? Is there blood or mucus in the stools? Any laxative use?
Associated factors: Are there periods of diarrhea? Is there abdominal pain or distention? Is the patient experiencing stress? Is there a change in activity level? Does the patient have a regular time for defecation? Does the patient use antacids containing calcium or an anticholinergic? Have there been any fevers, chills, night sweats, or weight loss?
History: Any family history of colorectal cancer? Any history of depression or metabolic disorders, such as hypothyroidism or hypercalcemia?
Dysphagia
Characteristics: Is the onset acute or gradual? Is the problem with swallowing intermittent or continuous? Is this associated with solid foods, liquids, or both? Has there been any nasal regurgitation? Where does the food stick: neck (cricopharyngeal), midesophagus, or sternal xiphoid process?
Associated factors: Is there any regurgitation, heartburn, chest or back pain, weight loss? Any hoarseness, voice change, or sore throat? Have there been any fevers, chills, night sweats, or weight loss?
History: Is there a family history of esophageal cancer? Is there a history of stroke, palsy, or any other neurologic conditions? Is there a history of alcohol or tobacco intake?
Physical Examination
When performing a physical examination of the abdomen, include the following: inspection of the abdomen, auscultation of all four abdominal quadrants, percussion for tympany or dullness, light and deep palpation.
NURSING ALERT
Auscultation should be performed before percussion and palpation, which may stimulate bowel sounds. Deep palpation in noted areas of tenderness or pain should be performed last.
Key Findings
Tenting of the skin when skin is rolled between thumb and index finger. Tenting may indicate dehydration.
Mouth lesions, missing teeth, swollen or bleeding gums may contribute to weight loss and nutritional deficiencies.
Body weight may indicate obesity or such problems as anorexia nervosa or malignancy.
Palpable mass may indicate an enlarged organ, inflammation, malignancy, hernia.
Rebound tenderness, guarding, and rigidity may indicate appendicitis, cholecystitis, peritonitis, pancreatitis, duodenal ulcer.
Protuberant or bulging abdomen or flanks can indicate ascites. Two physical assessment skills that may help to confirm the presence of ascites are testing for shifting dullness and testing for a fluid wave.
Distention and absence of bowel sounds may indicate intestinal obstruction.
Characteristics of Stool
The appearance of blood in stool may be characteristic of its source.
Upper GI bleeding—tarry black (melena).
Lower GI bleeding—bright red blood.
Lower rectal or anal bleeding—blood streaking on surface of stool or on toilet paper.
Other characteristics of stool may indicate a particular GI problem.
Laboratory tests for GI disorders include a variety of stool studies and blood tests.
Evidence Base
Rex, D. K., Johnson, D. A., Anderson, J. C., et al. (2009). American College of Gastroenterology guidelines for colorectal cancer screening 2009 (corrected). American Journal of Gastroenterology, 104, 739-750.
Fecal Immunochemical Test (FIT) for Occult Blood Detection
Description
An immunochemical test card has antibodies that detect human hemoglobin in stool. This test is used to screen for colon cancer and is preferred over the stool guaiac tests due to higher sensitivity and ease of use (eg, no dietary restrictions).
Nursing and Patient Care Considerations
Advise patient not to collect specimen during menstruation or if hemorrhoidal bleeding is present. Usually, at least 2 stool specimens need to be collected, on separate occasions.
Collect specimen or advise patient regarding proper collection of specimen.
Place collection paper on top of water in toilet.
Sit on toilet and proceed with bowel movement so that stool will be on top of collection paper.
Use the sample probe and brush across the stool sample so that groove of probe is filled with stool (obtain sample from several different locations within the stool).
Insert probe back into sample container and tighten lid of container.
Write date on sample container label.
Put container with stool sample into plastic bag and deliver to lab within 7 days (or if point-of-service test, follow manufacturer instructions for processing).
Stool Guaiac Tests for Occult Blood
Description
Commercially available guaiac-impregnated slides or wipes test feces for blood. May be used as another option for colon cancer screening.
Nursing and Patient Care Considerations
Advise patient about the test preparation procedure. Common practices are listed below. For 3 days before the test and during the stool collection period:
Diet should have a high fiber content.
Avoid red meat in the diet.
Avoid foods with a high peroxidase content, such as turnips, cauliflower, broccoli, horseradish, and melon.
Avoid iron preparations, iodides, bromides, aspirin, NSAIDs, or vitamin C supplements greater than 250 mg/day.
Avoid enemas or laxatives before stool specimen collection.
Collect sample or advise patient on collection procedure.
A wooden applicator is used to apply a stool specimen to the slide, or a special wipe is used and placed in the packet.
Avoid urine or toilet tissue contamination.
When hydrogen peroxide (denatured alcohol-stabilizing mixture) is added to samples, any blood cells present liberate their hemoglobin, and a bluish ring appears on the electrophoretic paper. Read precisely at 30 seconds.
Three stool samples are taken because of the possibility of intermittent bleeding and false-negative results.
A single positive test is an indication for further diagnostic evaluation for GI lesions.
False-positive results occur in about 10% of tests.
Test may become false-negative in 10% of specimens tested 4 or more days after streaking on paper.
Stool DNA Test
Description
This test detects DNA associated with colon cancer. Cells are shed from the tumor into the intestinal lumen as stool passes through. Procedure is similar to guaiac tests.
Other Common Stool Studies
Description
There are multiple types of stool analyses that are helpful in detecting conditions affecting the GI tract, liver, and pancreas. Basic stool examination is for amount, consistency, and color. Normal color varies from light to dark brown, but various foods and medications may affect stool color. Additional testing may include tests for ova and parasistes; stool cultures that can identify viruses and bacteria; fecal leukocytes; fecal fat, which can help in the diagnosis of malabsorption syndromes; and stool for Helicobacter pylori, which is performed about 4 weeks after treatment to confirm eradication.
Nursing and Patient Care Considerations
Use a tongue blade to place a small amount of fresh stool in a container. The container may be sterile or may have a preservative depending on which test has been ordered. Remind patient not to mix urine or toilet paper in specimen.
Save a sample of fecal material if unusual in appearance, contains worms or blood, blood streaked, unusual in color, or has excess mucus; show to health care provider.
For accurate specimen results, the vials must be sent to the laboratory as soon as possible. Certain stool studies allow for refrigeration of the sample, but this is test dependent.
Send specimens to be examined for parasites to the laboratory immediately so the parasites may be observed under a microscope while viable, fresh, and warm.
Test for occult blood or to confirm grossly visible melena or blood—Hemoccult guaiac test.
Consider that barium, bismuth, mineral oil, and antibiotics may alter the results.
Hydrogen Breath Test
Description
The hydrogen breath test is used to evaluate carbohydrate malabsorption and maldigestion, detect the presence of excess bacteria in the small intestine, and to estimate small bowel transit time.
A substance, such as lactulose, lactose, or another carbohydrate is ingested and, after a certain time period, exhaled gases are measured.
The test measures the amount of hydrogen, methane, and carbon dioxide produced in the colon, absorbed in the blood, and then exhaled in the breath. The levels of hydrogen and methane are indicators of bacterial metabolism in the small intestine.
This test is diagnostic for lactose intolerance, other carbohydrate malabsorption syndromes, and small intestine bacterial overgrowth (SIBO).
Nursing and Patient Care Considerations
Patient should have nothing-by-mouth (NPO) for 12 hours before the procedure.
Patient should not smoke after midnight before the test.
Antibiotics and laxatives/enemas should not be used for 1 week before the test. These products may alter the laboratory results.
Appropriate diet instructions should be given before discharge if the test is positive.
Helicobacter pylori Testing
Description
Diagnostic tests for H. pylori include a serum antibody test, urea breath test, and fecal antigen test. Alternatively, if an endoscopy is being performed, then biopsies of the gastric mucosa can be evaluated for H. pylori with rapid urea testing, histology review by a pathologist, or culture, or polymerase chain reaction testing.
A positive serum antibody test may not differentiate between current or past disease.
The urea breath test and fecal antigen test are useful in detecting active H. pylori prior to treatment with antibiotics. Both of these tests can be used to confirm eradication after antibiotic therapy has been completed.
Nursing and Patient Care Considerations
Symptomatic patients and patients with an active or past history of ulcer disease or with gastric MALT lymphoma should be tested for H. pylori. Endoscopy may be necessary for patients with symptoms of weight loss, anemia, or occult blood loss and for patients older than age 50.
It is recommended that negative H. pylori test results in a patient with ulcer-related complications be confirmed by a second test.
Describe the procedure for urea breath testing to the patient.
Antibiotics, proton-pump inhibitors, and bismuth preparations must be held for 2 weeks prior to testing.
Food and fluids should be held for at least 1 hour prior to testing.
A baseline breath sample will be taken by having the patient breathe into a container, then patient will ingest a carbon-labeled urea substance, and a final breath sample will be taken shortly after ingestion.
The whole process takes about 40 minutes.
When confirming eradication of H. pylori, testing should not be done earlier than 4 weeks posttreatment.
False-positive results from H. pylori breath testing may be caused by achlorhydria or urease production associated with other GI disorders.
Upper GI series and small-bowel series are fluoroscopic x-ray examinations of the esophagus, stomach, and small intestine after the patient ingests barium sulfate.
As the barium passes through the GI tract, fluoroscopy outlines the GI mucosa and organs.
Spot films record significant findings.
Double-contrast studies administer barium first, followed by a radiolucent substance, such as air, to produce a thin layer of barium to coat the mucosa. This allows for better visualization of any type of lesion.
Nursing and Patient Care Considerations
Explain procedure to patient.
Instruct patient to maintain low-residue diet for 2 to 3 days before test and a clear liquid dinner the night before the procedure.
Emphasize NPO after midnight before the test.
Encourage patient to avoid smoking before the test.
Explain that the health care provider may prescribe all opioids and anticholinergics to be withheld 24 hours before the test because they interfere with small-intestine motility. Other medications may be taken with sips of water, if ordered.
Explain that the patient will be instructed at various times throughout the procedure to drink the barium (480 to 600 mL).
Explain that a cathartic will be prescribed after the procedure to facilitate expulsion of barium.
Instruct patient that stool will be light in color for the next 2 to 3 days from the barium.
Instruct patient to notify health care provider if he has not passed the barium in 2 to 3 days because retention of the barium may cause obstruction or fecal impaction.
Note that a water-soluble iodinated contrast agent (eg, Gastrografin) may be used for a patient with a suspected perforation or colonic obstruction. Barium is toxic to the body if it leaks into the peritoneum with perforation. It can also worsen an obstruction, thus it is not used if an obstruction is suspected.
Barium Enema
Description
Fluoroscopic x-ray examination visualizing the entire large intestine is administered after the patient is given an enema of barium sulfate.
Can visualize structural changes, such as tumors, polyps, diverticula, fistulas, obstructions, and ulcerative colitis.
Air may be introduced after the barium to provide a doublecontrast study.
Nursing and Patient Care Considerations
Explain to patient:
What the x-ray procedure involves.
That proper preparation provides a more accurate view of the tract and that preparations may vary.
That it is important to retain the barium so all surfaces of the tract are coated with opaque solution.
Instruct patient on the objective of having the large intestine as clear of fecal material as possible:
Patient may be given a low-fiber, low-fat diet 1 to 3 days before the examination.
The day before examination, intake may be limited to clear liquids (no drinks with red dye).
The day before the examination, an oral laxative, suppository, and/or cleansing enema may be prescribed.
Patient will be NPO after midnight the day of the procedure.
An enema or cathartic may be ordered after the barium enema to cleanse bowel of barium and prevent impaction.
Inform patient that barium may cause light-colored stools for several days after the procedure.
NURSING ALERT
If barium enema and upper GI series are both ordered, the upper GI series is done last so that barium traveling down the digestive tract does not interfere with the results of the barium enema.
Ultrasonography (Ultrasound)
Description
A noninvasive test that focuses high-frequency sound waves over an abdominal organ to obtain an image of the structure.
Ultrasound can detect small abdominal masses, fluid-filled cysts, gallstones, dilated bile ducts, ascites, and vascular abnormalities.
Doppler ultrasonography may be ordered for vascular assessment.
Nursing and Patient Care Considerations
An ultrasound should be done prior to barium studies, or at least 24 hours after barium administration because it may interfere with the images.
Abdominal ultrasound usually requires patient to be NPO for at least 6 hours before the procedure.
Change position of patient, as indicated, for better visualization of certain organs.
Computed Tomography (CT)
Description
CT is an x-ray technique that provides excellent anatomic definition and is used to detect tumors, cysts, and abscesses.
The CT scan can also reveal masses, dilated bile ducts, pancreatic inflammation, and some gallstones.
It identifies changes in intestinal wall thickness and mesenteric abnormalities.
Ultrasound and CT can be used to perform guided needle aspiration of fluid or cells from lesions anywhere in the abdomen. The fluid or cells are then sent for laboratory tests (eg, cytology or culture).
Nursing and Patient Care Considerations
Instruct patient to fast for 4 hours before the procedure. Patient can take usual medications with a sip of water, but should hold diabetic medications.
A pregnancy test should be obtained on females of childbearing potential. If pregnant, do not proceed with scan and notify health care provider.
Ask if there are known allergies to iodine or contrast media. Intravenous (IV) administration of contrast medium may be performed to provide better visualization of body parts. If allergic, notify the technician and health care provider immediately.
Instruct patient to report symptoms of itching or shortness of breath if receiving contrast media, and observe patient closely.
Endoscopic Procedures
Evidence Base
Scholten, S. R. (2010). Endoscopy: A guide for the registered nurse. Critical Care Nursing Clinics of North America, 22(1), 19-32.
Endoscopy is the use of a flexible tube (the fiber-optic endoscope) to visualize the GI tract and to perform certain diagnostic and therapeutic procedures. Images are produced through a video screen or telescopic eyepiece. The tip of the endoscope moves in four directions, allowing for wide-angle visualization. The endoscope can be inserted through the rectum or mouth, depending on which portion of the GI tract is to be viewed. Capsule endoscopy utilizes an ingestible camera device rather than an endoscope.
Endoscopes contain multipurpose channels that allow for air insufflation, irrigation, fluid aspiration, and the passage of special instruments. These instruments include biopsy forceps, cytology brushes, needles, wire baskets, laser probes, and electrocautery snares.
Endoscopic functions other than visualization include biopsy or cytology of lesions, removal of foreign objects or polyps, control of internal bleeding, and opening of strictures.
Capsule Endoscopy
Description
Adjunctive diagnostic tool used to detect abnormalities of the small bowel (angiodysplasias, areas of active bleeding, polyps, ulcerations, tumors or causes of diarrhea, and nutritional malabsorption).
The procedure involves swallowing a capsule (camera device), which passes through the digestive system while taking pictures of the intestine.
Images are transmitted to sensor array abdominal leads, which are attached to a Walkman-like recording device belted to the patient’s waist.
After approximately 8 hours, the recording device is removed and is connected to a computer to download the images for review. The capsule will be excreted naturally through the digestive tract.
NURSING ALERT
Capsule endoscopy is contraindicated for patients with small bowel obstruction, dysphagia, fistulas, severe delayed gastric emptying, gastrectomy with gastrojejunostomy, or GI stricture. There is a risk of trapping the capsule, delayed passage, or impaired peristalsis. Pacemakers or implanted defibrillators may alter the quality and quantity of study information.
Nursing and Patient Care Considerations
Give patient instructions on bowel prep. Inform patient that a good bowel prep allows for better pictures. Patient will be NPO for about 12 hours before swallowing the camera.
Oral medications are discontinued 2 hours before the study. Antispasmodics, bismuth preparations, and antidiarrheal medications should be held for 24 hours before the study. Iron preparations and Carafate should be held 5 days before the study to prevent mucosal staining.
Instruct patient not to smoke 24 hours before the procedure to prevent mucosal staining.
Instruct patient to avoid strenuous activity, heavy lifting, bending or stooping, or immersion in water while wearing the leads and recorder. This is to prevent detachment of the leads or damage of the recorder.
After ingesting the capsule, patient is instructed not to eat or drink for at least 2 hours, then can advance to clear liquids. After 4 hours, patient can have a light snack and medications. When the procedure is completed, patient can resume a normal diet.
During the capsule endoscopy procedure, instruct the patient to check the blinking light on the top of the data recorder every 15 minutes. Avoid radio equipment (ham radio or broadcasting towers), which may interfere with the capsule’s signal.
The capsule is naturally excreted within 1 to 3 days. Patient should be instructed to call the physician for the following symptoms: abdominal bloating or pain, chest pain, vomiting, or fever. These symptoms may indicate that the capsule has obstructed the GI tract.
NURSING ALERT
The patient should verify excretion of the capsule before undergoing MRI.
Esophagogastroduodenoscopy (EGD)
Description
Allows for visualization of the esophagus, stomach, and duodenum.
EGD can be used to diagnose acute or chronic upper GI bleeding, esophageal or gastric varices, polyps, malignancy, ulcers, gastritis, esophagitis, esophageal stenosis, and gastroesophageal reflux.
Instruments passed through the scope can be used to perform a biopsy or cytologic study, remove polyps or foreign bodies, control bleeding, or open strictures.
Nursing and Patient Care Considerations
Ensure that patient is NPO for 6 to 12 hours before the procedure to prevent aspiration and allow for complete visualization of the stomach.
Remove dentures and partial plates to facilitate passing the scope and preventing injury.
As an outpatient, advise that someone must accompany the patient to drive home due to the patient being sedated.
Inform the health care provider of any known allergies and current medications. Medications may be held until after the test is completed.
Obtain prior x-rays, and send with patient.
Describe what will occur during and after the procedure:
The throat will be anesthetized with a spray or gargle.
An IV sedative will be administered.
Patient will be positioned on the left side with a towel or basin at the mouth to catch secretions.
A plastic mouthpiece will be used to help relax the jaw and protect the endoscope. Emphasize that this will not interfere with breathing.
Patient may be asked to swallow once while the endoscope is being advanced. Then patient should not swallow, talk, or move tongue. Secretions should drain from the side of the mouth, and the mouth may be suctioned.
Air is inserted during the procedure to permit better visualization of the GI tract. Most of the air is removed at the end of the procedure. Patient may feel bloated, burp, or pass flatus from remaining air.
Keep patient NPO according to protocol until patient is alert and gag reflex has returned.
May resume regular diet after gag reflex returns and fluids are tolerated.
May experience a sore throat for 24 to 36 hours after the procedure. When the gag reflex has returned, throat lozenges or warm saline gargles may be prescribed for comfort.
Monitor vital signs every 30 minutes for 3 to 4 hours, and keep the side rails up until patient is fully alert.
Monitor patient for abdominal or chest pain, cervical pain, dyspnea, fever, hematemesis, melena, dysphagia, light-headedness, or a firm distended abdomen. These may indicate complications.
Instruct patient on the above listed signs and symptoms and advise to report immediately should any occur, even after discharge.
Possible complications include perforation of the esophagus or stomach, pulmonary aspiration, hemorrhage, respiratory depression or arrest, infection, cardiac arrhythmias or arrest.
NURSING ALERT
Perforation of the GI tract is a complication of endoscopy. Assess for abdominal or chest pain, dyspnea, fever, tachycardia, lightheadedness, and distended abdomen. Report immediately.
Flexible Sigmoidoscopy and Colonoscopy
Sigmoidoscopy is the visualization of the anal canal, rectum, sigmoid colon, and proximal colon through a fiber-optic sigmoidoscope.
Colonoscopy is the visualization of the entire large intestine, sigmoid colon, rectum, and anal canal. It is used as a screening test for colon cancer because it can be used to identify and remove potentially precancerous and cancerous polyps.
Sigmoidoscopy or colonoscopy can be used to diagnose malignancy, polyps, inflammation, or strictures.
Colonoscopy is used for surveillance in patients with a history of chronic ulcerative colitis, previous colon cancer, or colon polyps.
Lower GI endoscopy can be used to perform biopsy, remove foreign objects, or obtain diagnostic specimens.
Colonoscopy requires bowel preparation for a couple of days before the procedure and use of conscious sedation during the procedure. The bowel preparation includes approximately 1 gallon of iso-osmolar electrolyte solution to consume over a 3- to 4-hour period the day before the procedure, a clear liquid diet the day before, and an oral laxative the night before (protocols vary). See Patient Education Guidelines for a sample preparation. If unable to tolerate CoLyte, GoLYTELY, or NuLytely, an alternate prep may be used.
PATIENT EDUCATION GUIDELINES
Colonoscopy Instructions
You have been scheduled for a colonoscopy to examine your large bowel (colon). It will be necessary for you to prepare your bowel before the procedure by drinking a substance called CoLyte, GoLYTELY, or NuLytely. It is not absorbed by your body; rather, it rinses solid matter from your colon. You should expect to empty your bowel frequently.
During the procedure, you will receive medication to keep you comfortable. You will be ready to leave the facility in 1 to 3 hours. The medication you will receive may affect your memory. You must bring a competent adult driver with you. Your driver will be responsible for signing you out and must receive the discharge instructions.
Do not take aspirin, aspirin-containing products, or iron supplements for 7 days before your exam. If you take a bloodthinning medication, such as Coumadin, call the health care provider who prescribed it for you for further instructions.
The day before your procedure
Begin clear liquid diet for the entire day (see below). NO SOLID FOOD. Make sure to drink plenty of fluids so you do not get dehydrated.
At 3 PM, start drinking one gallon of bowel prep (CoLyte, GoLYTELY, or NuLytely). You may have it on ice or refrigerated. You may add one package of lemon-lime Crystal Light to the entire gallon. Drink one glass every 10 to 15 minutes, completing the entire gallon in 2 hours. Slow down if you begin to feel bloated or nauseated (sick to your stomach). It is normal to feel chills while drinking the prep. Warm clothing may help. If you cannot drink the prep, call your health care provider for instructions.
You may continue to take clear liquids until midnight.
Do not eat or drink anything after midnight.
The day of your procedure
Take your heart and blood pressure medications with a small sip of water.
Insulin doses should be cut in half. If you are on a sliding scale, please bring your insulin with you.
Do not forget to bring an adult driver with you.
CT colonography, also known as virtual colonoscopy, is evolving as a noninvasive screening method.
CLEAR LIQUID DIET
Remember: NO SOLID FOOD
Food Group
Foods Included
Foods Excluded
Fruit Juices
All clear or strained fruit juices
• Red or orange juices
• Juices with pulp or that you cannot see through
Soup
Clear broth, bouillon, and consommé
• All other soups or stews
Desserts
Clear flavored gelatin, ice pops, fruit-flavored ices, hard candy
• Red or orange desserts, pudding, gelatin with fruit or whipped cream
Beverages
Coffee, tea, carbonated beverages, beverages, such as Kool-aid and Gatorade
• Red or orange beverages, dairy products, or other beverages
Adapted from SHANDS at the University of Florida.
DRUG ALERT
Sodium phosphate preps should be avoided in people with congestive heart failure, renal impairment, and in others that may be more sensitive to electrolyte imbalances.
Endoscopic Ultrasound (EUS)
Description
This procedure is a combination of endoscopy and ultrasonography to visualize the GI tract and can be used to evaluate the upper GI tract or the lower GI tract.
An ultrasonic transducer is built into the distal end of the endoscope.
This procedure allows for high-quality resolution and imaging of the walls of the esophagus, stomach, duodenum, small intestines, and colon. Adjacent abdominal structures can also be studied.
EUS is also indicated to evaluate and stage lesions of the GI tract.
Nursing and Patient Care Considerations
Verify patient’s compliance with the pretest bowel preparation the day before the procedure, usually an oral laxative (such as magnesium citrate) and a clear liquid diet.
Patient must be NPO after midnight.
Explain to patient that a feeling of fullness will occur when water is introduced into the GI tract. This eliminates air space and provides for high resolution.
If an upper EUS is performed, maintain the NPO status until the gag reflex returns. A lower EUS can be performed using a rectal approach.
Observe patient for a change in vital signs, bleeding, pain, vomiting, and abdominal distention or rigidity.
Make sure that patients who have had endoscopic procedures requiring sedation have a caregiver to drive them home after the procedure.
GENERAL PROCEDURES AND TREATMENT MODALITIES
Relieving Constipation and Fecal Impaction
One method of evacuating the lower bowel is an enema, the installation of a solution into the rectum and sigmoid colon. See Procedure Guidelines 18-1. If fecal impaction is discovered on exam, manual disimpaction may be performed to remove stool and promote bowel elimination (see Figure 18-1). However, it is best to try to prevent constipation by using fiber, laxatives, or stool softeners so that enemas and manual disimpaction are not needed.
PROCEDURE GUIDELINES 18-1
Administering an Enema
EQUIPMENT
Prepackaged enema or enema container
Disposable gloves
Water-soluble jelly
Waterproof pad
Bath blanket
Bedpan or commode
Washcloth and towel
Basin
Toilet tissue
PROCEDURE
Nursing Action
Rationale
Preparatory phase
1.
Assess the patient’s bowel habits (last bowel movement, laxative usage, bowel patterns) and physical condition (hemorrhoids, mobility, external sphincter control).
1.
Helps distinguish chronic constipation from new or acute condition. Enema should not be given if there is a suspicion of appendicitis or bowel obstruction.
2.
Provide for privacy and explain procedure to patient.
2.
Provides comfort and cooperation.
Performance phase
1.
Wash hands.
1.
Promotes hygiene.
2.
Place patient on left side with right knee flexed (Sims’ position). Place waterproof pad underneath patient and cover with bath blanket.
2.
Allows for enema solution to flow by gravity along the natural curve of the sigmoid colon and rectum.
3.
Place bedpan or bedside commode in position for patients who cannot ambulate to the toilet or who may have difficulty with sphincter control.
3.
Allows for easy accessibility.
4.
Remove plastic cover over tubing, and lubricate tip of enema tubing 3-4 inches (7.5-10 cm) unless prepackaged (tip is already lubricated). Even prepackaged enema may need more lubricant.
4.
Prevents trauma and eases application.
5.
Apply disposable gloves.
5.
Standard precautions.
6.
Separate buttocks and locate rectum.
7.
Instruct patient that you will be inserting tubing and to take slow, deep breaths.
7.
Allows for patient relaxation and readiness.
8.
Insert tubing 3-4 inches for adult patients.
8.
Prevents tissue trauma of rectum.
9.
Slowly instill the solution using a clamp and the height of the container to adjust flow rate if using an enema bag and tubing. For high enemas, raise enema container 12-18 inches (30.5-45.5 cm) above anus; for low enemas, 12 inches. If using a prepackaged enema, slowly squeeze the container until all solution is instilled.
9.
Rapid infusion can cause colon distention and cramping. Container elevated past 12-18 inches and controller on tubing not regulated contribute to rapid infusion.
10.
Lower container or clamp tubing if patient complains of cramping.
10.
Slows instillation and allows fluid time to disperse.
11.
Withdraw rectal tubing after all enema solution has been instilled and instruct patient to hold solution as long as possible and that a feeling of distention may be felt.
11.
Promotes better results.
12.
Discard supplies in the appropriate trash receptacle.
Assist patient on the bedpan or to the bedside commode or toilet when urge to defecate occurs.
13.
Prompt action will prevent soiling.
14.
Observe enema return for amount, fecal content. Instruct patient not to flush toilet until the nurse has seen the results.
14.
If enema has not had sufficient time to absorb, result may be mostly clear with little fecal material. One or two repeat enemas may be ordered, if much fecal matter is expected, and discontinued when return turns clear.
Follow-up phase
1.
Document the type of enema given, volume, and results on the appropriate chart forms.
1.
For continuity of care.
2.
Assess and document presence or absence of abdominal distention after enema was given.
2.
Relief of abdominal distention indicates success of gas relief.
3.
Assist the patient with washing perineum and rectal area, if indicated; may also need a clean gown or linen change.
3.
Fecal soiling may result, especially in bedridden patients.
NURSING ALERT Enemas should not be given routinely to treat constipation because they disrupt normal defecation reflexes, and the patient becomes dependent.
Purposes of Enema Administration
Bowel preparation for diagnostic tests or surgery to empty the bowel of fecal content.
Delivery of medication into the colon (such as enemas containing steroids to treat ulcerative proctitis or a sodium polystyrene sulfonate enema to decrease the serum potassium level).
To soften the stool (oil-retention enemas).
To relieve gas (tidal, milk and molasses, or Fleet’s enemas).
To promote defecation and evacuate feces from the colon for patients with constipation or an impaction (not a first-line therapy).
Figure 18-1. Fecal Impaction. (A) Note shaded area inside rectal sphincter, which indicates fecal impaction. (B) By gently stimulating the rectal wall with a gloved index finger and using a circular motion, it is possible to loosen fecal material. (C) It may be necessary to gently insert two fingers in an attempt to crush the fecal mass. A scissorlike motion is used.
Nursing and Patient Care Considerations
Consider manual removal of fecal impaction in the following patients at risk:
Older adults with chronic constipation or insufficient hydration, or who are inactive.
Orthopedic patients who have been in traction or in body casts.
When barium has not been adequately removed after radiologic examination.
Patients with neurologic or psychotic disorders.
Fecal impaction can occur with a descending/sigmoid colostomy. The fingers may be used to break up feces through the stoma, followed by cleansing irrigation.
Contraindications of manual removal of fecal impaction include:
Pregnancy.
After genitourinary, rectal, perineal, abdominal, or gynecologic surgery.
Be aware that manual removal of fecal impaction may cause syncope due to stimulation of the vagus nerve.
Nasogastric and Nasointestinal Intubation
Evidence Base
Niv, E., Fireman, Z., & Vaisman, N. (2009). Post-pyloric feeding. World Journal of Gastroenterology, 15(11), 1281-1288.
Nasogastric (NG) intubation refers to the insertion of a tube through the nasopharynx into the stomach (see Procedure Guidelines 18-2 and Procedure Guidelines 18-3, pages 652 to 655). NG intubation has multiple purposes including stomach decompression, stomach lavage (irrigation due to active bleeding or poisoning), medication administration, and short-term feeding.
Nasointestinal (NI) intubation is performed by inserting a small-bore, weighted tube that is carried by way of peristalsis into the duodenum or jejunum. Insertion of this type of tube can be done manually, endoscopically, or fluoroscopically. Using fluoroscopy is considered the “gold standard” or preferred method of insertion. NI intubation is primarily used for administering feedings and maintaining nutritional intake (see Procedure Guidelines 18-4, page 656).
Nursing and Patient Care Considerations
If patient is unconscious, advance the tube between respirations to make sure it does not enter the trachea.
You will need to stroke the unconscious patient’s neck to facilitate passage of the tube down the esophagus.
Watch for cyanosis while passing the tube in an unconscious patient. Cyanosis indicates the tube has entered the trachea.
If patient has a nasal condition that prevents insertion through the nose, the tube is passed through the mouth.
Remove dentures, slide the distal end of the tube over the tongue, and proceed the same way as a nasal intubation.
Make sure to coil the end of the tube and direct it downward at the pharynx.
Pain or vomiting after the tube is inserted indicates tube obstruction or incorrect placement.
If the NG tube is not draining, the nurse should reposition tube by advancing or withdrawing it slightly (with a physician’s order). After repositioning, always check for placement.
Recognize the complications when the tube is in for prolonged periods: nasal erosion, sinusitis, esophagitis, esophagotracheal fistula, gastric ulceration, and pulmonary and oral infections.
Extended-use NG tubes are made of a flexible, soft plastic material with manufacturer’s recommendations that may include leaving the tube in place for up to 30 days before changing the tube.
Assess the color, consistency, and odor of gastric contents. Coffee ground-like contents may indicate GI bleeding. Report findings immediately.
The tube should be irrigated before and after medication administration through the tube.
Medications should be given in liquid form, if possible.
Clamp the tube for 30 to 45 minutes to ensure medication absorption before reconnecting to suction, if ordered.
Check GI function by auscultating for bowel sounds on a regular basis after the tube has been clamped for 30 minutes.
PROCEDURE GUIDELINES 18-2
Nasogastric Intubation
EQUIPMENT
Nasogastric (NG) tube—usually single-lumen Levin or double-lumen Salem sump tube
Anesthetic jelly or spray or watersoluble lubricant
Suction equipment, if ordered
Clamp for tubing
Towel, tissues, and emesis basin
Glass of water and straw
Hypoallergenic tape: ½ inch and 1 inch
Bio-occlusive transparent dressing
60 mL syringe
pH paper
Penlight
Disposable gloves and face shield
Normal saline
PROCEDURE
Nursing Action
Rationale
Preparatory phase
1.
Ask if patient has ever had nasal surgery, trauma, a deviated septum, or bleeding disorder.
1.
Nasogastric tubes may be contraindicated in patients with nasopharyngeal or esophageal obstruction, severe uncontrolled coagulopathy, or severe maxillofacial trauma.
2.
Explain procedure to the patient, and tell how mouth breathing, panting, and swallowing will help in passing the tube.
2.
Improves comfort and compliance.
3.
Place the patient in a sitting or high-Fowler’s position; place a towel across chest.
3.
Facilitates passage of tube into esophagus.
4.
Determine with the patient what sign he might use, such as raising the index finger, to indicate “wait a few moments” because of gagging or discomfort.
4.
Provides a method of communication, which is reassuring to the patient.
5.
Remove dentures; place emesis basin and tissues within the patient’s reach.
5.
Dentures may become loose and interfere with tube insertion.
6.
Inspect the tube for defects; look for partially closed holes or rough edges.
6.
Irrigation and suction may be affected by defective tube.
7.
Determine the length of the tube needed to reach the stomach (see accompanying figure).
7.
Prevents coiling of tube in stomach or tube ending in esophagus.
8.
Have the patient blow nose to clear nostrils.
8.
Facilitates passage through the nose.
9.
Inspect the nostrils with a penlight, observing for any obstruction. Occlude each nostril, and have the patient breathe.
9.
Helps determine which nostril is more patent.
10.
Wash your hands. Put on disposable gloves (face shield should also be considered).
10.
Protects nurse from patient’s secretions.
11.
Hold the end of the NG tube at the tip of the patient’s nose, extend the tube to the earlobe and then down to the xiphoid process. Mark this distance on the tubing with tape.
11.
The measurement will help ensure that the end of the tube reaches the stomach.
Measuring nasogastric tube length.
Performance phase
1.
Lubricate the first 2 to 3 inches of the tube with watersoluble lubricant. Avoid occluding the tube’s holes with lubricant.
1.
Lubrication reduces friction between the mucous membranes and tube and prevents injury to the nasal passages. Using a water-soluble lubricant prevents oil aspiration pneumonia if the tube accidentally slips into trachea.
2.
With patient’s head in a neutral position, insert tube into nostril and gently pass tube into the posterior nasopharynx, directing downward and backward toward the ear.
2.
The passage of the tube is facilitated by following the natural contours of the body. The slower the advancement of the tube at this point, the less likelihood of putting pressure on the turbinates, which could cause pain and bleeding.
3.
When tube reaches the pharynx, the patient may gag; allow patient to rest for a few moments.
3.
Gag reflex is triggered by the presence of the tube.
4.
Have the patient tilt head slightly forward. Offer several sips of water through a straw, or permit patient to suck on ice chips, unless contra indicated. Advance tube as patient swallows.
4.
Flexed head position partially occludes the airway, and the tube is less likely to enter trachea. Swallowing closes the epiglottis over the trachea and facilitates passage of tube into the esophagus. Actually, when the tube passes the cricopharyngeal sphincter into the esophagus, it can be slowly and steadily advanced even if the patient does not swallow.
5.
Gently rotate the tube 180 degrees to redirect the curve.
5.
Prevents the tube from entering the patient’s mouth.
6.
Continue to advance tube gently each time the patient swallows.
6.
Facilitates forward movement and prevents trauma and discomfort.
Key Decision Point
Be especially cautious with tube insertion in patients with craniofacial trauma, reduced cough and gag reflexes, confusion, presence of endotracheal tube, decreased consciousness, and uncooperative behavior. If obstruction appears to prevent tube from passing, do not use force. Rotating tube gently may help. If unsuccessful, remove tube and try another nostril.
If there are any signs of distress while passing the tube, such as gasping, coughing, or cyanosis, immediately remove tube. The tube may have entered the trachea.
7.
Continue to advance the tube when the patient swallows, until the tape mark reaches the patient’s nostril.
7.
Reference point where the tube was measured.
8.
To check whether the tube is in the stomach:
8.
a.
Ask the patient to talk.
a.
If the patient cannot talk, the tube may be coiled in throat or passed through vocal cords.
b.
Obtain aspirate with 60-mL syringe and check for gastric fluid characteristics. If stomach contents cannot be aspirated, reposition the patient. Attempt to aspirate again.
b.
Gastric fluid characteristics: pH ≤ 5 and gastric fluid characteristics of grassy green, clear and colorless, or brown.
c.
X-rays may be obtained to confirm tube placement.
c.
Consider x-ray confirmation of tube placement in patients with risk factors for malpositioning of tubes.
NURSING ALERT Never place the end of the tube in water while checking placement. If the tube is in the trachea, the patient could aspirate.
9.
After tube is passed and the correct placement is confirmed, attach the tube to suction or clamp the tube.
9.
Clamping can be done using a clamp, plastic plug, or folding the tube over and slipping the bend into the tube end.
10.
Anchor tube with:
10.
Prevents the patient’s vision from being disturbed; prevents tubing from rubbing against nasal mucosa. This will ensure tape being secure. Do not tape to forehead, which could cause necrosis of the nostril.
a.
Hypoallergenic tape; split lengthwise and only halfway, attach unsplit end of tape to nose, and cross split ends around tubing. Apply another piece of tape to bridge of nose.
b.
Bio-occlusive transparent dressing where it exits the nose.
11.
Anchor the tubing to the patient’s gown. Use a rubber band to make a slipknot to anchor the tubing to the patient’s gown. Secure the rubber band to the patient’s gown using a safety pin.
11.
Permits mobility of patient. This prevents tugging on the tube when the patient moves.
12.
Clamp the tube until the purpose for inserting the tube takes place.
13.
Attach the larger lumen of the Salem sump tube to suction equipment if ordered. Low continuous suction or high intermittent suction may be used with the Salem sump tube. If the Levin tube is used, low intermittent suction is recommended.
13.
Prevents gastric mucosal damage, if a vacuum forms and the tube adheres to the gastric wall.
Follow-up phase
1.
Assure the patient that most discomfort will lessen with time.
2.
Irrigate the tube at regular intervals (every 4 hours unless otherwise indicated) with small volumes of prescribed fluid. Remember to always check placement first.
2.
Ensures tube patency.
a.
If the tube is a Salem sump, it will require periodic placing of 10 to 20 cc of air through the vent port (blue port or smaller lumen). Do not instill water into the vent and, if the vent is draining fluid, instill air to clear it.
b.
Check the Salem sump tube patency by placing the vent port next to your ear.
b.
A soft hissing sound is heard if the tube is patent. If the port hangs downward and the tube backs up, stomach contents will spill over the patient.
3.
Cleanse nares and provide mouth care every shift.
3.
Promotes patient comfort and decreases risk of infection.
4.
Apply petroleum jelly to nostrils, as needed, and assess for skin irritation or breakdown.
4.
Keeps tissue soft and prevent crusting and skin breakdown.
5.
Keep head of bed elevated at least 30 degrees.
5.
Minimizes gastroesophageal reflux.
6.
Record the time, type, and size of tube inserted. Document placement checks after each assessment, along with amount, color, consistency of drainage.
6.
Ensures proper tube and placement at all times, and assists in evaluation of tube effectiveness.
Evidence Base Simons, S. R., & Abdallah, L. M. (2012). Bedside assessment of enteral tube placement: Aligning practice with evidence. American Journal of Nursing, 112(2), 40-46.
Caring for the Patient Undergoing Gastrointestinal Surgery
Total gastrectomy—complete excision of the stomach with esophageal—jejunal anastomosis.
Subtotal or partial gastrectomy—a portion of the stomach excised:
Billroth I procedure—gastric remnant anastomosed to the duodenum.
Billroth II procedure—gastric remnant anastomosed to the jejunum.
Gastrostomy (Janeway or Spivak)—rectangular stomach flap created into abdominal stoma, used for intermittent tube feedings.
PROCEDURE GUIDELINES 18-3
Nasogastric Tube Removal
EQUIPMENT
Towel
Disposable gloves
Lip pomade
Mouth hygiene materials
PROCEDURE
Nursing Action
Rationale
Preparatory phase
1.
Make sure that gastric or small bowel drainage is not excessive in volume.
1-3.
Tube may not be discontinued unless drainage is minimal, bowel sounds are present, and patient is passing flatus.
2.
Make sure, by auscultation, that audible peristalsis is present.
3.
Determine whether the patient is passing flatus, which indicates peristalsis.
4.
Verify the health care provider’s order for removal.
4.
Complies with the Joint Comission National Patient Safety Goals.
Performance phase
1.
Place a towel across the patient’s chest and inform about the withdrawal.
1.
No doubt, the patient will be happy to have progressed to this stage.
2.
Apply disposable gloves.
2.
Provides protection from contaminated body fluids.
3.
Turn off suction; disconnect and clamp tube.
3.
Prevents fluids from leaking from tube.
4.
Remove the tape from the patient’s nose.
5.
Instruct the patient to take a deep breath and hold it.
5.
This maneuver closes the epiglottis.
6.
Slowly, but evenly, withdraw tubing and cover it with a towel as it emerges. (As the tube reaches the nasopharynx, you can pull quickly.)
6.
Covering the tubing helps dispel patient’s nausea.
7.
Provide the patient with materials for oral care and lubricant for nasal dryness.
7.
Mouthwash and a nasal lubricant will be appreciated by the patient.
8.
Dispose of equipment in appropriate receptacle.
9.
Document time of tube removal and the patient’s reaction.
10.
Document tube removal and color, consistency, and amount of drainage in suction canister.
9-10.
For continuity of care.
11.
Continue to monitor the patient for signs of GI difficulties.
11.
Recurrence of nausea or vomiting may require reinsertion of nasogastric tubing. Changes in vital signs may suggest infection.
Hernia Surgeries
Herniorrhaphy—surgical repair of a hernia with suturing of the abdominal wall.
Hernioplasty—reconstructive hernia repair with mesh sewn over the defect for reinforcement.
Bowel Surgeries
Appendectomy—excision of the vermiform appendix.
Bowel resection—segmental excision of small and/or large bowels with varied approaches:
Anastomosis of proximal and distal ends of bowel.
Anastomosis of proximal and distal ends of bowel with temporary diverting loop ostomy.
Both ends of bowel exteriorized to the abdominal wall with proximal ostomy and distal mucous fistula.
Hartmann’s procedure—proximal large bowel as ostomy; distal end of large bowel oversewn inside abdomen as Hartmann’s pouch.
Low-anterior resection—subtotal resection of the rectum with colorectal or coloanal anastomosis.
Abdominoperineal resection—a combined abdominal and perineal approach for removal of the rectum and anus with permanent colostomy.
Subtotal colectomy—partial removal of the large bowel or colon.
Total colectomy—complete removal of the large bowel or colon with varied approaches:
Ileorectal anastomosis—colon removal with ileum anastomosed to rectum.
Proctocolectomy—colon removal including the rectum and anus with permanent ileostomy.
Ileal reservoir—anal anastomosis. (Colon removal, subtotal proctectomy, possible distal rectal mucosectomy, creation of pelvic reservoir from two, three, or four loops of ileum with anastomosis at anal canal. Usually a temporary loop ileostomy is performed as fecal diversion to protect the reservoir and the ileal—anal anastomosis. After takedown of temporary loop ileostomy [2 to 3 months postoperatively], the reservoir stores feces and patient eliminates under voluntary control through the anus [see page 694].)
Kock or Barnett continent internal reservoir (BCIR) procedures—proctocolectomy, creation of a continent small bowel reservoir with nipple valve abdominal stoma used for stool removal through routine intubation. (Continence is provided through the nipple valve.)
Roux-en-Y jejunostomy—jejunum severed with distal end exteriorized as permanent stoma for intermittent tube feedings; proximal end reanastomosed to GI tract distal to stoma to reestablish pathway.
Intestinal feeding tubes are soft, flexible, small-diameter (8 or 12 French) tubes with a longer length than gastric feeding tubes (measuring up to 47 inches [120 cm] as compared with approximately 30 inches [76 cm] for a gastric feeding tube). Some tubes are weighted at the distal end of the tube. All tubes should be routinely pretested for patency and function before passage.
PROCEDURE
Nursing Action
Rationale
Preparatory and performance phases (by health care provider—nurse assisted)
1.
Tube preparation:
1.
a.
Do not ice plastic tubes.
a.
Become too stiff to work with.
b.
Inject 10 mL of water into the tube.
b.
Removes air that may cause gas.
c.
Insert guide wire or stylet into tube, making sure it is positioned snugly against tube.
After the tube enters the stomach, it passes by peristalsis and gravity into the small intestine. Change patient’s position from Fowler’s to a position in which the patient is lying on his or her right side.
3.
Assists in advancing the tubing to and through the pylorus; tilting to the right is helpful.
4.
Obtain an x-ray of the abdomen after tube insertion. Stylet should remain in place until position is confirmed.
4.
Confirms placement.
5.
When tube placement has been confirmed, mark the tube at the nare exit site.
5.
Helpful in reassessment of tube position. Check that the mark on the tube remains at the exit site.
Nursing/patient care considerations
1.
Be aware of risk of aspiration in an unconscious patient.
1.
Inserted tube prevents total closure of airway.
2.
Instruct patient on complications associated with tube feedings, such as nausea, vomiting, diarrhea.
2.
Feedings that are too large or too fast cause these symptoms.
3.
A continuous drip infusion delivered with an infusion pump may lessen the risk of aspiration, abdominal distention, and/or diarrhea.
3.
Controls the volume and rate of infusion.
4.
If abdominal distention, vomiting, or diarrhea occurs, notify the health care provider; the rate of infusion may need to be adjusted.
4.
May indicate paralytic ileus.
Laparoscopic Surgery
GI surgical procedures are increasingly being assisted by the use of a laparoscope, either partially or totally. The laparoscope is usually inserted through a 1-cm umbilical incision with additional trocars used for visualization and assistance. Dissection is performed with endocautery, scissors, or laser.
Advantages may include reduction in postoperative pain, shorter hospital and recuperative periods, decreased risk of infection, and improved cosmetic outcome. The direct cost of a laparoscopic procedure may be greater than an open procedure; however, the overall cost of the procedure and recuperative period may be lower due to a more rapid recovery.
Contraindications may include obesity, internal adhesions, and bowel obstruction with distention.
Cholecystectomies and appendectomies are routinely done through laparoscopy; hernia repairs can be done using the laparoscope. Other GI surgeries, including ostomies and bowel resections (may include select cancer patients), are increasingly being done through this surgical approach.
Preoperative Management
All diagnostic tests and procedures are explained to promote cooperation and relaxation.
The patient is prepared for the type of surgical procedure as well as postoperative care (IV, patient-controlled analgesia pump, NG tube, surgical drains, incision care, possibility of ostomy).
Measures to prevent postoperative complications are taught, including coughing, turning, and deep breathing; using the incentive spirometer; and splinting the incision.
IV fluids or total parenteral nutrition (TPN) before surgery may be ordered to improve fluid and electrolyte balance and nutritional status.
Intake and output is monitored.
Preoperative laboratory studies are obtained.
Bowel cleansing will be initiated 1 to 2 days before surgery for better visualization. Preparation may include diet modifications, such as liquid or low residue, oral laxatives, suppositories, enemas, or polyethylene glycoelectrolyte solution (CoLyte, GoLYTELY).
Antibiotics are ordered to decrease the bacterial growth in the colon.
An ostomy specialty nurse is consulted if patient is scheduled for an ostomy to initiate early understanding and management of postoperative care.
Patient may not have anything by mouth after midnight the night before surgery. Medications may be withheld, if ordered. This will keep the GI tract clear.
Postoperative Management and Nursing Care
Physical assessment is completed at least once per shift, or more frequently, as indicated.
Monitor vital signs for signs of infection and shock— fever, hypotension, tachycardia.
Monitor intake and output for signs of imbalance, dehydration, and shock. Include all drains in evaluating intake and output.
Assess abdomen for increased pain, distention, rigidity, and rebound tenderness because these may indicate postoperative complications. Report abnormal findings.
Expect diminished or absent bowel sounds in the immediate postoperative phase.
Evaluate dressing and incision. Check for purulent or bloody drainage, odor, and unusual tenderness or redness at incision site, which may indicate bleeding or infection.
Evaluate for passing of flatus or feces.
Monitor for nausea and vomiting. Note the presence of fecal smell or material in vomitus because it may indicate an obstruction.
Check NG aspirate, vomitus, and stools for signs of bleeding. Record and report findings if present.
Laboratory values are monitored and patient is evaluated for signs and symptoms of electrolyte imbalance.
Wound drains, IV lines, and all other catheters are monitored and evaluated for signs of infection or infiltration.
To maintain patency of NG tube, the tube may be irrigated with 30 mL of normal saline solution every 2 hours and as needed. If there are large amounts of NG output, IV replacement may be necessary.
Subcutaneous heparin may also be ordered to prevent embolus. Antiembolism stockings may be used.
Turning, coughing, deep breathing, and incentive spirometry are performed every 2 hours. Dangling at bedside is encouraged the night of surgery and an attempt at ambulation the first postoperative day is made, unless ordered otherwise.
Patient-controlled analgesia for pain control or other analgesics, as ordered, are administered to promote comfort.
Wound dressing is changed every day or as needed, maintaining aseptic technique.
Diet is advanced, as ordered, after presence of bowel sounds indicates GI tract has regained motility. After 1 to 2 days of NPO postoperatively, the usual diet progression is ice chips, sips of water, clear liquids, full liquids, soft or regular diet.
Dietary education includes fiber, avoiding gas-producing foods, and maintaining adequate fluid intake.
Reinforcement of teaching and assistance with ostomy care, if indicated.
Administration of medications, as ordered, which may include a stool softener or laxative when bowel function has returned.
NURSING ALERT
Due to the type of abdominal surgery and location of the suture line, the health care provider may order not to irrigate or manipulate the NG tube.
Complications
Paralytic ileus or obstruction.
Peritonitis or sepsis.
Anastomotic leakage, which may result in peritonitis.
Nursing Diagnoses
Acute Pain related to surgical incision.
Imbalanced Nutrition: Less Than Body Requirements related to dietary modifications after surgery.
Impaired Skin Integrity related to surgical incision.
Constipation related to surgery.
Risk for Infection related to surgical incision.
Deficient Fluid Volume related to surgical procedure.
Nursing Interventions
Promoting Comfort
Assess pain location, intensity, and characteristics, and make sure they are appropriate for postoperative stage.
Administer prescribed pain medications, and provide instructions if using a patient-controlled analgesia pump, to keep patient comfortable.
Assess the effectiveness of the pain medications. If ordered, promethazine can potentiate the effectiveness of pain medication.
Encourage the patient to change positions frequently and to splint incision when turning, coughing, or deep breathing to minimize discomfort.
Improving Nutritional Status
Monitor intake and output each shift, or more frequently if indicated, to maintain fluid balance.
Advance diet as tolerated.
Weigh the patient daily to ensure adequate calorie intake.
Provide snacks or high-protein, high-calorie supplements and assist in menu selection, if needed.
Instruct the patient to avoid gas-producing foods, and encourage ambulation.
Improving Skin Integrity
Assess wound for signs of erythema, swelling, and purulent drainage, which may indicate infection.
Change surgical dressing every 24 hours, and as needed, to protect skin from drainage and decrease risk of infection.
Apply dressings around drains and tubes to protect skin from leakage, if indicated.
Turn the patient frequently or encourage position changes to prevent skin breakdown over bony prominences.
Promoting Bowel Elimination
Assess for presence of bowel sounds to evaluate return of bowel function.
Ask the patient if passing flatus rectally or through an ostomy—also indicative of return of bowel function.
Evaluate for abdominal distention, nausea, or vomiting, which may indicate obstruction.
Monitor stool for frequency, amount, and consistency.
Administer stool softener or laxative, as ordered, to promote comfort with elimination.
Encourage diet with adequate fiber and fluid content for natural laxative effect.
Encourage and assist with ambulation to promote peristalsis.
Preventing Infection
Monitor temperature every shift or as ordered, and review previous readings to recognize early increases.
Change surgical dressings every 24 hours, or more frequently, as indicated. Maintain aseptic technique to avoid contamination.
Monitor wound for signs and symptoms of infection, such as redness, swelling, purulent drainage, odor, and pain.
Obtain a wound culture, as ordered.
Monitor the patient with a Foley catheter for signs and symptoms of urinary tract infection (UTI), such as concentrated, cloudy urine; hematuria; fever. If Foley discontinued, monitor for the above plus complaints of burning and frequency.
Assist the patient in washing perineum daily and as needed if incontinence is present, for increased comfort and hygiene.
Assess breath sounds and monitor for crackles.
Instruct the patient to turn, cough, deep-breathe, and use incentive spirometer every 2 hours to minimize complications.
Encourage early ambulation to initiate bowel function and reduce risk of embolus.
Administer antibiotics, as ordered, to maintain constant blood level.
Maintaining Fluid Volume
Monitor intake and output every 8 hours, or more frequently, if ordered, to assess recent status. Include amount of wound drainage from dressing changes and drains that may be in place.
Assess the patient for signs of dehydration—flushed, dry skin; tenting of skin; oliguria; tachycardia, hypotension, and rapid respirations; increase in hematocrit, blood urea nitrogen (BUN), electrolytes; fever; weight loss.
Monitor laboratory results and report abnormal findings.
Assess the patient for signs of electrolyte imbalance—nausea or vomiting, cardiac dysrhythmia, tremor, seizures, anorexia, malaise, weakness, irregular pulse; changes in behavior, mental status.
Weigh the patient daily to ensure adequate caloric intake.
Administer parenteral fluids, enteral feedings, and blood products, as ordered, to maintain volume during period of decreased oral intake.
Community and Home Care Considerations
Reinforce discharge instructions and the importance of postoperative regimen to include health provider follow-up appointments and laboratory and other scheduled tests or therapies.
A person who has undergone a total gastrectomy needs lifelong parenteral administration of vitamin B12 to prevent pernicious anemia. This may also apply to people with the terminal ileum removed, and sometimes for those with ileostomies.
Change dressing and reinforce ostomy care as directed by health care provider. Report any signs of infection—unusual drainage, redness, warmth, increased pain, swelling.
Instruct to gradually increase activities of daily living. No heavy lifting (more than 10 lb), pushing, pulling, or driving for 6 to 8 weeks postoperatively.
Referral to additional community resources if applicable (support groups, meal programs, social services).
Patient Education and Health Maintenance
Review signs and symptoms of wound infection so early intervention may be instituted.
Explain signs and symptoms of other postoperative complications to report—elevated temperature, nausea or vomiting, abdominal distention, changes in bowel function and stool consistency or color.
Instruct the patient to report promptly blood in the stool or the coughing up of blood.
Teach the patient regarding wound and/or ostomy care, if applicable, to promote healing and self-confidence.
Encourage the patient to turn, cough, deep-breathe; to use incentive spirometer; and ambulate. Discuss the importance of these functions during the recovery period.
Review dietary changes, such as increased fiber content and fluid intake, and their importance in improving bowel function.
Review actions and adverse effects of prescribed medications to encourage compliance and understanding of management.
Assess the need for home health follow-up and initiate appropriate referrals if indicated.
Evaluation: Expected Outcomes
Verbalizes increased comfort (using a 0-to-10 pain scale, with 0 being no pain and 10 being the highest score to measure pain).
Consumes 50% to 75% of each meal; no weight loss.
Incisional flaps approximated and healing ridge present.
Passing flatus and stool.
No signs and symptoms of infection.
Vital signs stable, fluid and electrolytes in balance.
A surgically created opening between the colon and the abdominal wall to allow fecal elimination. It may be a temporary or permanent diversion.
A colostomy may be placed in any segment of the large intestine (colon), which will influence the nature of fecal discharge. The more right-sided the colostomy, the looser the stool. Transverse and descending/sigmoid colostomies are the most common types.
A colostomy may be performed as part of an abdominoperineal resection for rectal cancer; a fecal diversion for unresectable cancer; a temporary measure to protect an anastomosis; or surgical treatment for inflammatory bowel diseases, trauma, perforated diverticulitis, ischemic bowel, cancer, and congenital conditions.
STANDARDS OF CARE GUIDELINES 18-2
Care of the Patient with an Ostomy
Prepare patient and patient’s family preoperatively by explaining the surgical procedure, stoma characteristics, and ostomy management with a pouching system.
Have ostomy specialty nurse mark an optimal stoma site.
Postoperatively, monitor the stoma color and amount and color of stomal output every shift; document and report any abnormalities.
Periodically change a properly fitting pouching system over the ostomy to avoid leakage and protect the peristomal skin. Use this time as an opportunity forteaching.
Assess peristomal skin with each pouching system change, document findings, and treat any abnormalities (skin breakdown due to leakage, allergy, or infection) as indicated.
Teach patient and/or caregiver self-care skills of routine pouch emptying, cleansing skin and stoma, and changing of the pouching system until independence is achieved.
Instruct patient and family in lifestyle adjustments regarding gas and odor control; procurement of ostomy supplies; and bathing, clothing, and travel tips.
Encourage patient to verbalize feelings regarding the ostomy, body image changes, and sexual issues.
Inform patient of community resources, such as United Ostomy Association, local and mail-order ostomy supply dealers, ostomy specialty nurses, American Cancer Society, and Crohn’s & Colitis Foundation.
This information should serve as a general guideline only. Each patient situation presents a unique set of clinical factors and requires nursing judgment to guide care, which may include additional or alternative measures and approaches.
Figure 18-2. A diagrammatic representation of the placement of fecal ostomies and nature of discharge at these sites.
Ileostomy
A surgically created opening between the ileum of the small intestine and the abdominal wall to allow elimination of small bowel effluent.
An ileostomy is usually formed at the terminal ileum of the small bowel and is usually placed in the right lower quadrant of the abdomen. Stool from an ileostomy drains frequently (average four to five times per day) and contains proteolytic enzymes, which can be harmful to skin.
Diagnoses that may require a temporary or permanent ileostomy include ulcerative colitis, Crohn’s disease, familial polyposis, cancer, congenital defects, and trauma.
Characteristics of Stomas
A stoma is the part of the intestine (small or large) that is brought above the abdominal wall to become the outlet for discharge of intestinal waste. Stoma is often used interchangeably with “ostomy.”
Normal stomal characteristics: pink-red, moist, bleeds slightly when rubbed, no feeling to touch, stool functions involuntary, and postoperative swelling gradually decreases over several months.
Stoma classifications:
End stoma: After bowel is divided, the proximal bowel is exteriorized to abdominal wall, everted (which exposes mucosal lining), and sutured to dermis or subcutaneous tissue. There is only one opening that drains stool. The distal bowel is either surgically removed or sutured closed within abdominal cavity.
Double-barrel stoma: After bowel is divided, the proximal and distal ends of bowel are exteriorized to abdominal wall, everted, and sutured to the dermis or subcutaneous tissue. If the stomas are brought up next to each other requiring them to be pouched together, they are referred to as a double-barrel stoma; if the stomas are apart to be pouched separately, they may be referred to as an end stoma (proximal), which drains stool, and a mucous fistula (distal), which drains mucus. This type of stoma is usually temporary.
Loop stoma: A bowel loop is brought to the abdominal wall through an incision and stabilized temporarily with a rod, catheter, or a skin or fascial bridge. The anterior wall of bowel is opened surgically or by electrocautery to expose the proximal and distal openings. The posterior wall of bowel remains intact and separates the functioning proximal opening and the nonfunctioning distal opening. This type of stoma is usually temporary.
Preoperative Management and Nursing Care
Prepare the patient for general abdominal surgery (see page 657). Have the patient see an ostomy specialty nurse.
An ostomy specialty nurse has the title of certified ostomy care nurse or certified wound, ostomy, and continence nurse (CWOCN, previously known as a certified enterostomal therapy nurse). These nurses play a vital role in the rehabilitation of patients with ostomies and related problems.
The Wound Ostomy and Continence Nurses Society has an official publication called the Journal of Wound, Ostomy, and Continence Nursing (www.wocn.org).
Administer replacement fluid, as ordered, before surgery due to possible increased output during the postoperative phase.
Provide low-residue diet before NPO status.
Explain that the abdomen may be marked by the ostomy specialty nurse or surgeon to ensure proper positioning of the stoma. Note: The abdominal location of the stoma is usually determined by anatomical location of the bowel segment (eg, a sigmoid colostomy is ideally located in left lower abdominal quadrant).
Other considerations when selecting a stoma include:
Positioning within rectus muscle.
Avoidance of bony prominences, such as iliac crest and costal margin.
Clearance from umbilicus, scars, and deep creases, observed in lying, sitting, and standing positions.
Positioning on a flat pouching surface.
Avoidance of beltline when possible.
Positioning within patient’s visibility to optimize independent ostomy care.
Support the patient and family with the many psychosocial considerations of ostomy surgery.
Postoperative Management and Nursing Care
Administer general abdominal surgery care (see page 657).
Assess stoma every shift for color and record findings:
Normal color: pink-red.
Dusky: dark red; purplish hue (ischemic sign).
Necrotic: brown or black; may be dry (notify health care provider to determine extent of necrosis).
Apply pouching system as close to stoma as possible without it being rubbed. It is acceptable to have a -to 1/8-inch clearance to prevent constriction, which can contribute to edema (see Box 18-2).
Check for abdominal distention, which reduces blood flow to stoma through mesenteric tension.
Evaluate and empty drains and ostomy pouch frequently to promote patency and maintain seal.
Monitor intake and output with extreme accuracy because output may remain high during early postoperative period.
Suction and irrigate NG tube frequently, as ordered, to relieve pressure and decrease gastric contents.
Offer continued support to patient and family.
Complications
Mucocutaneous separation (between skin and stoma).
Stomal ischemia.
Stomal stricture or stenosis (usually a long-term complication).
Stomal prolapse.
Peristomal hernia.
Peristomal skin breakdown from exposure to fecal output, allergic reaction to products, or infection, such as candidiasis.
BOX 18-2 Fecal Ostomy Pouching Systems
Pouching systems are varied according to manufacturer and patient needs. Systems are classified as one-piece or two-piece and disposable or reusable. A disposable, onepiece pouch is commonly used with backing as adhesive tape, skin barrier, or both. A disposable two-piece system consists of a skin barrier wafer with or without a tape border and a pouch. Disposable systems are popular and are discarded after one use. Reusable systems are declining in use and are made of heavier material, allowing use for weeks to months. They require the use of double-backed adhesive disks, cement, or belt to provide a seal.
Pouching systems are available in precut sizes and cut-to-fit options as well as with a flat backing versus degrees of convexity. Convex pouching systems are used with flush or retracted stomas to increase stomal protrusion and reduce undermining of feces.
Fecal pouches are available in closed-end and drainable styles. Drainable pouches require the use of a tail closure and may be used more than once. Closed-end pouches may contain a built-in filter to release gas and require no tail closure. A closed-end pouch is discarded after one use. Pouch selection depends on the patient’s preference or ability to manipulate the volume and frequency of fecal output.
Many accessory products are available to assist in the management of a fecal ostomy. They include skin sealants, skin barrier powders, pastes, washers, adhesive removers, tapes, belts, pouch covers, and deodorants.
The goal is to change a pouching system on a routine basis to prevent leakage. Usually, this is every 3 to 7 days and will vary per individual needs. Routine changes allow for examination of the peristomal skin for breakdown. Schedule the change when the bowel is least active, usually early morning before breakfast, 2 to 4 hours after a meal, or before bedtime. At times, the pouching system may need to be changed immediately if leakage is imminent, itching or burning of peristomal skin is present, odor is detected with a closed system, or the wafer is dissolving.
Nursing Diagnoses
Deficient Knowledge related to surgical procedures and ostomy management.
Disturbed Body Image related to change in structure, function, and appearance.
Anxiety related to loss of bowel control and autonomy.
Impaired Skin Integrity related to irritation of peristomal skin by drainage and equipment.
Imbalanced Nutrition: Less Than Body Requirements related to increased output and inadequate intake.
Sexual Dysfunction related to altered body structure.
Nursing Interventions
Educating the Patient
Review the surgical procedure with the patient and discuss the information that the surgeon and other providers have given. Clarify any misunderstandings.
Avoid overwhelming the patient with information.
Include family in discussions, when appropriate.
Use available educational materials, including pictures and drawings, if the patient is receptive.
Involve the ostomy specialty nurse (CWOCN) in ostomy teaching and reinforce information, including lifestyle modifications.
Use a team approach; the need for information may come from many disciplines.
Assess the patient’s response to teaching. If the patient is not interested, provide alternative times for teaching and review.
Consider the psychosocial issues of the patient and their effect on learning.
Promoting a Positive Self-Image
Encourage the patient to verbalize feelings about the surgical outcome.
Provide support during initial viewing of the stoma and encourage the patient to touch the area.
Encourage spouse or significant other to view the stoma.
Arrange a visit by a United Ostomy Association ostomy visitor if the patient desires. This is preferably done preoperatively.
Offer counseling, as necessary, and encourage the patient to use normal support systems, such as family, church, community groups.
Reducing Anxiety
Provide information regarding expected outcomes, such as the type and consistency of bowel function.
Introduce gradual steps toward achieving independent ostomy management. The patient may progress through the following steps:
Observe stoma, pouch change, and emptying procedure.
Review that irrigating involves inserting an enema into a descending or sigmoid colostomy.
Reinforce its purposes of cleansing the colon and stimulating the colon to move at a desired time regularly to regain control of fecal elimination.
It is a patient preference whether colostomy irrigations are attempted for control. Irrigation may occur every day or every other day depending on bowel pattern. It usually takes 1 to 2 months to establish control. Patients with a preoperative history of regular, formed bowel movements are more likely to realize success.
Disadvantages to colostomy irrigation: it is time-consuming, requires consistency, and bowel dependence may occur.
Only a patient with a descending or sigmoid colostomy is an irrigation candidate for fecal control. A colostomy more proximal than descending has too much liquid and too high a volume of fecal output to be managed through irrigation.
If a patient discontinues colostomy irrigations after months or years of performance, due to illness, hospitalization, or preference, a bulk laxative or other stimulant may be routinely necessary to maintain regular bowel function.
Acknowledge that it is normal to have negative feelings toward ostomy surgery; empathize with the patient.
Describe behaviors to attain a sense of control such as resuming activities of daily living (ADLs).
PROCEDURE GUIDELINES 18-5
Changing a Two-Piece Drainable Fecal Pouching System
EQUIPMENT
Duplicate wafer and pouch
Washcloth and towel
Tail closure
Mild, nonoily soap (optional)
Accessory products prescribed for patient
PROCEDURE
Nursing Action
Rationale
Preparatory phase
1.
Have patient assume a relaxed position and provide privacy. The best position may be sitting, reclining, or standing.
1.
Patient must see stoma site to learn care.
Performance phase
1.
To remove pouching system:
1.
a.
Wear nonsterile gloves.
a.
Maintains universal precautions.
b.
Push down gently on skin while lifting up on the wafer (ostomy adhesive remover may be used).
b.
Minimizes skin trauma.
c.
Discard soiled pouch and wafer in odorproof plastic bag. Save tail closure for reuse.
c.
Removes room odor and maintains universal precautions.
2.
To cleanse skin:
2.
a.
Use toilet tissue to remove feces from stoma and skin if needed.
a.
Stoma may function during the change.
b.
Cleanse stoma and peristomal skin with soft cloth and water, soap optional. The patient may shower with or without pouching system in place. Clip or shave peristomal hair if appropriate.
b.
Minimizes skin breakdown and promotes hygiene.
c.
Rinse and dry skin thoroughly after cleansing. It is normal for the stoma to bleed slightly during cleaning and drying.
c.
Removes residue, which may interfere with adhesion of wafer.
3.
To apply wafer:
3.
a.
Use measuring guide or pattern to determine stoma size.
a.
This step is omitted when stomal shrinkage is complete, about 2 months postoperatively.
b.
Trace correct size onto back of wafer and cut to stoma size. It is acceptable to cut 1/16 to 1/18 inch larger than stoma.
b.
Avoids wafer rubbing stoma; omit this step if the wafer is precut.
c.
Apply a line of skin barrier paste around stoma or on lip of wafer opening. Allow to set according to manufacturer’s instructions. (Other barrier may be used in place of paste, such as strips or washer. Some may find the paste too difficult to see or have developed an allergy to the alcohol within the paste.)
c.
Extra skin protection is imperative for ileostomy and right-sided colostomy. A left-sided colostomy may not need a secondary barrier because formed stool is less harmful to skin. Paste acts as “caulking” to prevent undermining of feces.
d.
Remove paper backing from the wafer, center opening over stoma, and press wafer down onto peristomal skin.
d.
Ensures adherence.
4.
Snap pouch onto the flange of the wafer according to manufacturer’s directions (see accompanying figure).
4.
If attached properly, there will be no leakage or odor.
5.
Apply tail closure to pouch tail.
5.
Proper closure controls odor.
(A)A wafer with flange (1 ½”, 1 ½”, 2¼”, 2¾”, 4”) is applied after cleaning and drying of peristomal skin.(B)A transparent or opaque drainable pouch is positioned over stoma at desired angle.(C)Pouch may be removed without removal of wafer.(D)Stoma may be assessed without removing wafer. (Adapted with permission from Convatec, a Bristol-Myers, Squibb Company.)
Follow-up phase
1.
Dispose of plastic bag with waste materials.
1.
Complies with universal precautions.
2.
Clean drainable pouch with soap and water, if appropriate. Drainable pouches may be reused several times.
2.
Controls odor; reduces cost.
3.
A commercial deodorant can be placed in the pouch to reduce odor.
4.
Gas can be released from the pouch by releasing the tail closure or by snapping off an area on the pouch flange. Never make a pinhole in the pouch to release gas.
4.
Destroys the odorproof seal.
Only gold members can continue reading. Log In or Register to continue
 DRUG ALERT
DRUG ALERT NURSING ALERT
NURSING ALERT Evidence Base
Evidence Base Evidence Base
Evidence Base NURSING ALERT
NURSING ALERT Evidence Base
Evidence Base NURSING ALERT
NURSING ALERT NURSING ALERT
NURSING ALERT NURSING ALERT
NURSING ALERT DRUG ALERT
DRUG ALERT NURSING ALERT Enemas should not be given routinely to treat constipation because they disrupt normal defecation reflexes, and the patient becomes dependent.
NURSING ALERT Enemas should not be given routinely to treat constipation because they disrupt normal defecation reflexes, and the patient becomes dependent.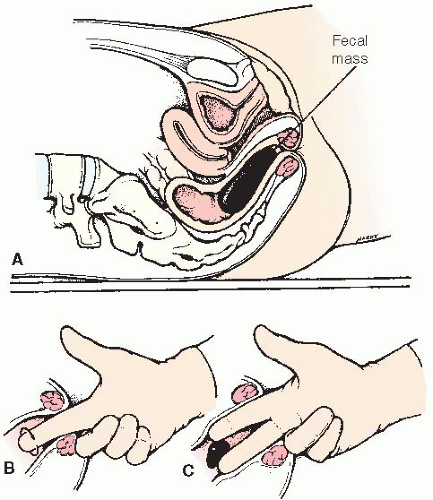
 NURSING ALERT
NURSING ALERT Evidence Base
Evidence Base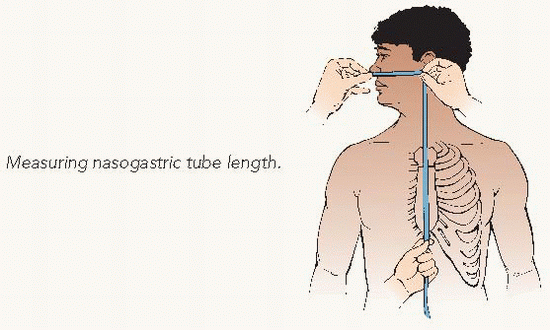 Measuring nasogastric tube length.
Measuring nasogastric tube length. Key Decision Point
Key Decision Point NURSING ALERT Never place the end of the tube in water while checking placement. If the tube is in the trachea, the patient could aspirate.
NURSING ALERT Never place the end of the tube in water while checking placement. If the tube is in the trachea, the patient could aspirate. Evidence Base Simons, S. R., & Abdallah, L. M. (2012). Bedside assessment of enteral tube placement: Aligning practice with evidence. American Journal of Nursing, 112(2), 40-46.
Evidence Base Simons, S. R., & Abdallah, L. M. (2012). Bedside assessment of enteral tube placement: Aligning practice with evidence. American Journal of Nursing, 112(2), 40-46. NURSING ALERT
NURSING ALERT NURSING ALERT
NURSING ALERT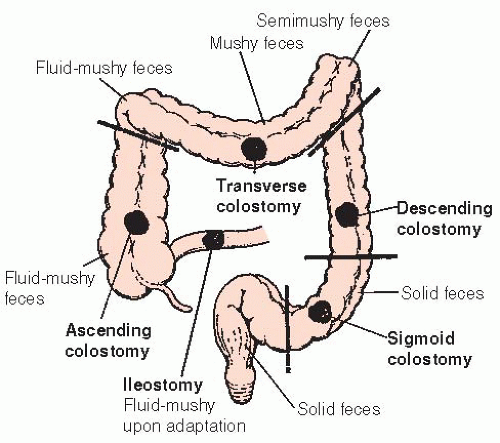
 -to 1/8-inch clearance to prevent constriction, which can contribute to edema (see Box 18-2).
-to 1/8-inch clearance to prevent constriction, which can contribute to edema (see Box 18-2).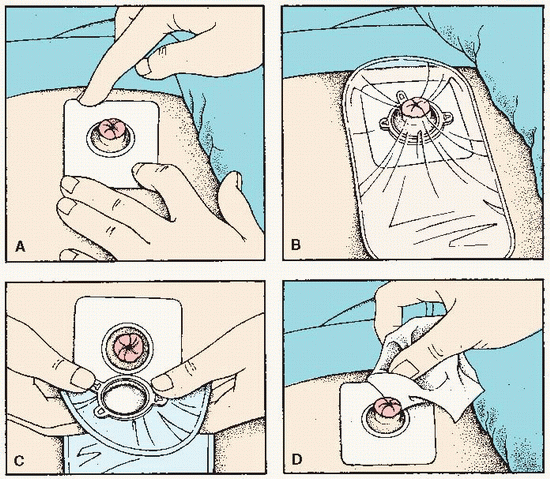 (A) A wafer with flange (1 ½”, 1 ½”, 2¼”, 2¾”, 4”) is applied after cleaning and drying of peristomal skin. (B) A transparent or opaque drainable pouch is positioned over stoma at desired angle. (C) Pouch may be removed without removal of wafer. (D) Stoma may be assessed without removing wafer. (Adapted with permission from Convatec, a Bristol-Myers, Squibb Company.)
(A) A wafer with flange (1 ½”, 1 ½”, 2¼”, 2¾”, 4”) is applied after cleaning and drying of peristomal skin. (B) A transparent or opaque drainable pouch is positioned over stoma at desired angle. (C) Pouch may be removed without removal of wafer. (D) Stoma may be assessed without removing wafer. (Adapted with permission from Convatec, a Bristol-Myers, Squibb Company.)


