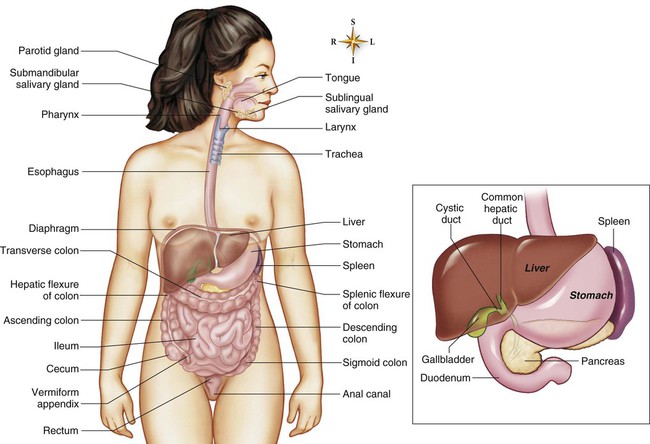
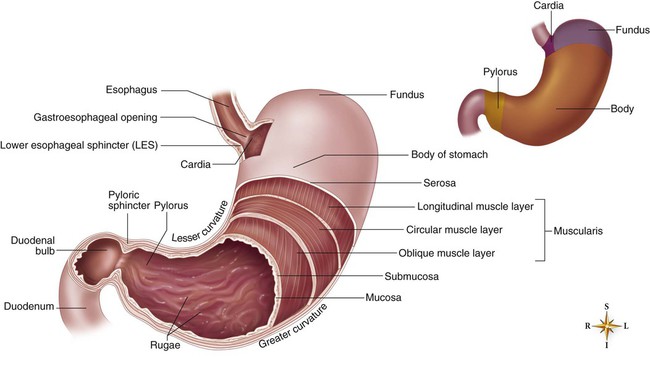
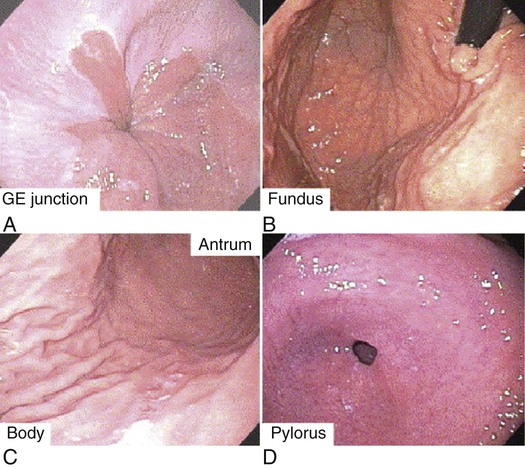
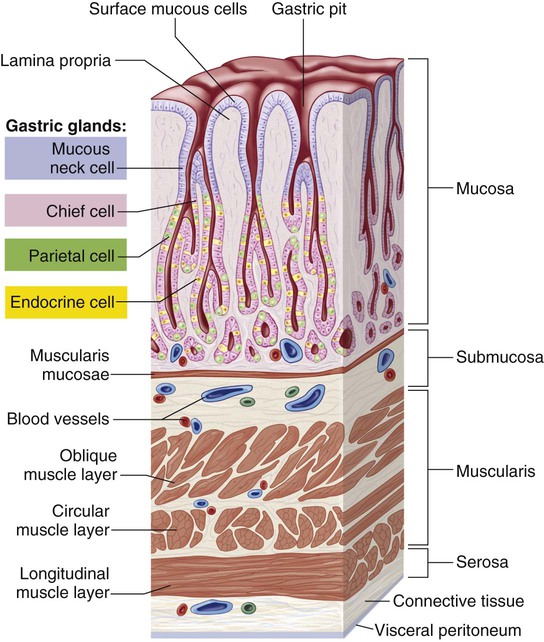
The critical care nurse must have a comprehensive knowledge of the anatomy and normal function of the GI tract to facilitate assessment, diagnosis, and intervention in patients with GI dysfunction. The GI tract consists of the mouth, the esophagus, the stomach, the small intestine, and the large intestine (Fig. 28-1). The mouth and accessory organs, which include the lips, cheeks, gums, tongue, palate, and salivary glands, perform the initial phases of digestion, which are ingestion, mastication, and salivation.1 The mouth is the beginning of the alimentary canal (see Fig. 28-1) and is the means for ingestion and entry of nutrients. The teeth cut, grind, and mix food, transforming it into a form suitable for swallowing and increasing the surface area of food available to mix with salivary secretions. Healthy dentition is vital for this process. Mucous glands located behind the tip of the tongue and serous glands located at the back of the tongue aid in the lubrication of food and in its distribution over the taste buds.2 Salivation has an important role in the first stage of digestion because saliva lubricates the mouth, facilitates the movement of the lips and the tongue during swallowing, and washes away bacteria. Saliva consists of approximately 99.5% water,3 which contains a large amount of ions such as potassium, chloride, bicarbonate,1 thiocyanate, and hydrogen;3 immunoglobulin A, which is vital for destroying oral bacteria;1 and mucus. Approximately 1000 to 1500 milliliters (mL) of saliva is produced each day by three pairs of major salivary glands: (1) the submandibular glands, (2) the sublingual glands, and (3) the parotid glands. Parotid gland secretions are enzymatic, containing amylase (ptyalin), which begins the chemical breakdown of large polysaccharides into dextrins and sugars. The mouth and pharynx also are lined with minor salivary glands that provide additional lubrication.3 The salivary glands are regulated by the autonomic nervous system, with parasympathetic effects being predominant. Increased parasympathetic stimulation results in profuse secretions of watery saliva, whereas decreased parasympathetic stimulation results in inhibition of salivation.1,3 The esophagus is a hollow muscular tube that lacks cartilage. In adults, it is 23 to 25 cm (9 to 10 inches) long and 2 to 3 cm (1 inch) wide. It is the narrowest part of the digestive tube and lies posterior to the trachea and the heart, with attachments at the hypopharynx and at the cardiac portion of the stomach below the diaphragm. It begins at the level of the C6 to T1 vertebrae and extends vertically through the mediastinum and diaphragm to the level of T11.4 The esophagus has two sphincters: (1) the upper esophageal sphincter (also known as hypopharyngeal sphincter) and (2) the lower esophageal sphincter (also known as cardioesophageal or gastroesophageal sphincter).4 The upper esophageal sphincter inhibits air from entering the esophagus during respiration. The lower esophageal sphincter controls the passage of food into the stomach and prevents reflux of gastric contents.1 The functions of the esophagus are to accept a bolus of food from the oropharynx, to transport the bolus through the esophageal body by gravity and peristalsis, and to release the bolus into the stomach through the lower esophageal sphincter. This process is known as swallowing.5 Peristalsis consists of waves of circular muscle contractions and relaxations. Peristalsis that is initiated by swallowing is known as primary peristalsis, whereas peristalsis that is initiated by esophageal distention is known as secondary peristalsis. Peristaltic waves begin in the pharynx and move distally at a rate of 2 to 6 cm per second.1 The stomach is an elongated pouch that is approximately 25 to 30 cm (10 to 12 inches) long and 10 to 15 cm (4 to 6 inches) wide at the maximal transverse diameter (Fig. 28-2). It lies obliquely beneath the cardiac sphincter at the esophagogastric junction and above the pyloric sphincter, next to the small intestine. The anatomic divisions of the stomach are the cardia (proximal end), the fundus (portion above and to the left of the cardiac sphincter), the body (middle portion), the antrum (elongated, constricted portion), and the pylorus (distal end connecting the antrum to the duodenum) (Fig. 28-3). The greater curvature, which begins at the cardiac orifice and arches backward and upward around the fundus, is in contact with the transverse colon and the pancreas at the posterior edge. The lesser curvature extends from the cardia to the pylorus. Two sphincters control the rate of food passage: (1) the lower esophageal sphincter at the esophagogastric junction and (2) the pyloric sphincter at the gastroduodenal junction.6 The stomach wall has four layers (Fig. 28-4). The outermost layer, the serous layer (serosa), consists of squamous epithelial tissue and continues as a double fold from the lower edge of the stomach to cover the intestine. The second layer, the muscular layer (muscularis), extends from the fundus to the antrum and consists of three smooth muscle layers, which are the longitudinal layer, the circular layer, and the oblique layer. The third layer, the submucous layer (submucosa), consists of connective tissue that contains blood vessels, lymphatics, and nerve plexuses. The innermost layer, the mucous layer (mucosa), consists of a muscular layer that is arranged in longitudinal folds, or rugae, that can expand as the stomach fills.6 This layer also contains glands that secrete about 1500 mL of gastric juice per day.7 The celiac artery provides the blood supply required for the motor and secretory activities of the stomach. The splenic vein provides venous drainage for the right side of the stomach, and the gastric vein provides it for the left.1 Numerous lymphatic channels arise in the submucosa and terminate in the thoracic duct. The stomach is innervated by the autonomic nervous system. Sympathetic fibers arise from the celiac plexus, and parasympathetic fibers arise from the gastric branch of the vagus nerve.6 The epithelial cells of the gastric mucosa are packed very close together and serve as a protective barrier, preventing diffusion of hydrogen ions into the mucosa. The surface epithelial cells produce alkaline mucus and secrete a bicarbonate-laden fluid. The mucus further protects the gastric mucosa by delaying back-diffusion of hydrogen ions and trapping them for neutralization by the secreted bicarbonate.7 The gastric mucosal cells can compensate for cell destruction. Epithelial cells are in a constant state of growth, migration, and desquamation, and they are shed at a rate of one half million cells per minute. The gastric mucosa also has the ability to increase blood flow, providing an additional buffer for acid neutralization and aiding in the removal of toxic metabolites and chloride ions from injured mucosa. The gastric mucosal cells synthesize a family of unsaturated fatty acids known as prostaglandins. Prostaglandins facilitate mucosal bicarbonate secretion and inhibit acid secretion by preventing the activation of parietal cells by histamine (a local biochemical mediator). Certain lipid-soluble substances such as alcohol, aspirin, and other nonsteroidal anti-inflammatory drugs, regurgitated bile, and uremic toxins, can break through the mucosal barrier and penetrate the cells, causing their destruction, edema, and eventual bleeding.7 The stomach has two types of glands—oxyntic (also known as gastric glands), and pyloric—that contain cells of various types that secrete 1500 to 2400 mL of gastric juice into the lumen per day, depending on the diet and other stimuli.7 Gastric juice is composed of hydrochloric acid (HCl), pepsin (necessary for the breakdown of protein), mucus, intrinsic factor (necessary for vitamin B12 absorption), sodium, and potassium. Pepsinogen, secreted by the chief cells of the stomach lining, is converted to its active form, pepsin, in the acidic environment of the stomach.1 The cardiac glands secrete mucus and pepsinogen. The oxyntic glands contain parietal cells, which secrete HCl and intrinsic factor, and chief cells, which secrete pepsinogen. Pyloric glands contain mucous cells, which secrete mucus and pepsinogen, and G-cells, which secrete gastrin (Table 28-1).6 Gastric glands are stimulated by the parasympathetic stimulation and gastrin and inhibited by gastric-inhibitory peptide and enterogastrone. Histamine and entero-oxyntin also stimulate the parietal cells to produce acid, and secretin stimulates the chief cells to produce pepsinogen.1 TABLE 28-1
Gastrointestinal Anatomy and Physiology
Mouth
Ingestion and Mastication
Salivation
Esophagus
Swallowing
Stomach
Gastric Secretion
SOURCE
HORMONE
STIMULUS FOR SECRETION
ACTION
Mucosa of the stomach
Gastrin
Presence of partially digested proteins in the stomach
Stimulates gastric glands to secrete hydrochloric acid and pepsinogen; growth of gastric mucosa; promotes gastric motility
Histamine
Acid in the stomach
Stimulates acid secretion
Somatostatin
Acid in the stomach
Inhibits acid and pepsinogen secretion and release of gastrin
Acetylcholine
Vagus and local nerves in stomach
Stimulates release of pepsinogen and acid secretion
Gastrin-releasing peptide (bombesin)
Vagus and local nerves in stomach
Stimulates gastrin and release of pepsinogen and acid secretion
Mucosa of the small intestines
Motilin
Presence of acid and fat in the duodenum
Increases gastrointestinal (GI) motility
Secretion
Presence of chyme (acid, partially digested proteins, and fats) in the duodenum
Stimulates pancreas to secrete alkaline pancreatic juice and liver to secrete bile; decreases GI motility; inhibits gastrin and gastric acid secretion
Cholecystokinin
Presence of chyme (acid, partially digested proteins, and fats) in the duodenum
Stimulates gallbladder to eject bile and pancreas to secrete alkaline fluid; decreases gastric motility; constricts pyloric sphincter; inhibits gastrin; delays gastric emptying
Enteroglucogon
Intraluminal fats and carbohydrates
Weakly inhibits gastric and pancreatic secretion and enhances insulin release, lipolysis, ketogenesis, and glycogenolysis; delays gastric emptying
Gastric-inhibitory peptide (GIP)
Fat and glucose in small intestine
Inhibits gastric secretion and gastric emptying, stimulates insulin release
Peptide YY
Intraluminal fat and bile acids
Inhibits postprandial gastric acid and pancreatic secretion and delays gastric and small bowel emptying
Pancreatic polypeptide
Protein, fat, and glucose in small intestine
Decreases pancreatic bicarbonate
Vasoactive intestinal peptide
Intestinal mucosa and muscle
Relaxes intestinal smooth muscle, increases blood flow ![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Gastrointestinal Anatomy and Physiology
Get Clinical Tree app for offline access
