The introduction of electronic fetal monitoring (EFM) in the late 1960s has had a far-reaching impact on perinatal care and the practice of nursing, midwifery, and medicine. Despite debate about advantages and limitations, effects on perinatal morbidity and mortality, and role in healthcare costs and malpractice litigation, EFM is used in the majority of labor and birth units in the United States and Canada today. This chapter discusses the physiologic basis for fetal heart rate (FHR) monitoring, defines FHR patterns, and reviews intrapartum management of FHR patterns.
HISTORICAL PERSPECTIVES
Publication of the discovery of fetal heart tones in 1822 marked the beginning of modern obstetric practice (Sureau, 1996; Goodlin, 1979). Jean Alexandre Le Jumeau, Vicomte de Kergaradec used a stethoscope hoping to hear the noise of the water in the uterus. Although M. Maior of Geneva was the first person credited with identifying fetal heart tones, Kergaradec was the first person astute enough to suggest in print potential clinical uses for FHR auscultation (Kennedy, 1843; Goodlin, 1979). In the early 1800s, researchers working independently in Switzerland, Ireland, Germany, France, and the United States described fetal heart tones, and in 1833, the British obstetrician William Kennedy described fetal heart sounds as a “quick double pulsation” with a usual rate of 130 to 140 beats per minute (bpm). Kennedy (1843) noted the rate was sometimes slower and sometimes much faster, depending on “inherent vital causes” (p. 107). He documented fetal heart variation in labor, including rates as high as 180 to 200 bpm in ill mothers and slowing and cessation of the FHR prior to stillbirth. In 1858, Schwartz of Germany suggested that the FHR be counted often during labor, both between and during contractions, to promote improved outcomes. Schwartz described the association between fetal bradycardia and decreased uteroplacental blood flow during contractions. In 1849, Killian proposed forceps-assisted birth for an FHR of fewer than 100 bpm or greater than 180 bpm (Goodlin, 1979). Soon after, Winckel described specific FHR criteria to be used for the diagnosis of fetal distress via auscultation (Goodlin, 1979). After the invention of the fetoscope in the early 1900s, fetal heart sounds were commonly assessed in order to document fetal viability during the prenatal period. Winckel’s criteria were used in clinical practice until the 1950s when Hon raised concern about the subjectivity of counting heartbeats during labor.
Although interest in continuous recording of fetal heart tones by various methods dates to the later years of the 19th century, the major development of modern clinical EFM occurred during the 1960s. In 1906, Cramer produced the first electrocardiographic (ECG) recording of the fetal heartbeat. Research using abdominal leads to obtain the fetal ECG continued but remained impractical for clinical use until the mid-1960s, when techniques capable of excluding the maternal ECG from the recording became available. By the 1950s, research on electronic methods of FHR monitoring escalated. In 1958, Hon published the first report of continuous fetal ECG monitoring using a device placed on the maternal abdomen. By the 1960s, Hon, Caldeyro-Barcia, and Hammacher were reporting successful attempts at developing an electronic FHR monitor that could continuously record FHR data (Caldeyro-Barcia et al., 1966; Hammacher, 1969; Hon, 1963). Although many others have contributed to what is known about fetal assessment during labor, EFM, as it is used today, is largely the result of the work of these three investigators working independently on separate continents. In 1968, the first commercially available EFMs were introduced.
Coinciding with the development of EFM technology was the emergence of data that refuted the effectiveness of intermittent auscultation (IA) with Delee or Pinard fetoscopes. The Benson, Shubeck, Deutsch-berger, Weiss, and Berendes (1968) study of more than 24,000 births, called the Collaborative Perinatal Project, concluded that FHR auscultation during labor was unreliable in determining fetal distress except in extreme cases of terminal bradycardias. Based on this report and rapid technologic advances, IA of the FHR between contractions was rapidly replaced with continuous EFM during the 1970s. Over the next three decades, EFM became the preferred method of fetal surveillance during the intrapartum period in the United States and Canada.
During the 1980s and 1990s, several randomized trials that compared IA to continuous EFM were conducted (MacDonald, Grant, Sheridan-Pereira, Boylan, & Chalmers, 1985; Thacker, Stroup, & Peterson, 1995; Vintzileos et al., 1993). Disappointingly, EFM did not decrease perinatal mortality or prevent cerebral palsy. Equally important, the women in EFM groups experienced a fourfold increase in operative birth (Thacker et al., 1995). The potential reasons why EFM did not demonstrate efficacy in the randomized trials include methodological flaws, inconsistent criteria and terminology to describe fetal status, and the use of outcome variables for which there were insufficient sample sizes to determine a significant difference between IA and continuous EFM.
The demonstrated increase in cesarean birth rates fueled reexamination of all aspects of EFM use. In 1997, the National Institute of Child Health and Human Development (NICHD) of the National Institutes of Health convened a panel of FHR monitoring experts. This group proposed quantitative definitions of FHR characteristics to serve as a basis for standardizing research that uses FHR data (NICHD, 1997). Between 1997 and 2004, there was gradual but sporadic adoption of the proposed standardized FHR definitions in clinical practice in the United States. In July 2004, the Joint Commission on Accreditation of Healthcare Organizations (JCAHO; now known as The Joint Commission [TJC]) recommended use of a standard language for communication and documentation of FHR patterns. In May 2005, the Association of Women’s Health, Obstetric and Neonatal Nurses (AWHONN) and the American College of Obstetricians and Gynecologists (ACOG) formally supported adoption of the NICHD definitions for FHR patterns as the standardized language for communicating fetal status (ACOG, 2005a; AWHONN, 2005). In 2008, the NICHD held an interdisciplinary meeting to consider the status of FHR terminology and whether there was a need for additional guidance regarding interpretation of FHR patterns (Spong, 2008). The 1997 definitions of FHR characteristics were reaffirmed at this meeting (Table 15-1), and a new classification system for interpretation of FHR patterns was proposed (Macones, Hankins, Spong, Hauth, & Moore, 2008) (Table 15-2). These changes were incorporated into ACOG (2009a, 2010b) practice bulletins, the AWHONN (2010a, 2010b) fetal monitoring program (Lyndon & Ali, 2009), American College of Nurse-Midwives (ACNM; 2010a, 2010b) documents, and National Certification Corporation (NCC) certification examinations.
Currently, clinical reliance on EFM remains high despite the lack of positive results from published research. To date, EFM is the primary screening technique for the clinical determination of the adequacy of fetal oxygenation during labor. This paradox is better understood following a review of the physiology of the fetal heart and its adaptations during labor. The feelings of many clinicians about EFM versus IA were summarized by Cibils in 1996 (p. 1383): “It is difficult to understand the premise that the intermittent recording (by a crude method) of a given biologic variable [the FHR] will be better to make a clinical decision affecting the mother and fetus than the continuous, precise recording of the same variable.” Chen, Chauhan, Ananth, Vintzileos, and Abuhamad (2011) conducted retrospective cohort study of over 4 million U.S. births occurring between 24 and 44 weeks’ gestation in 2004, using linked birth certificate and infant death certificate data. They found that EFM was used in 89% of births, and EFM use was associated with a substantially decreased risk of low Apgar scores (<4), low Apgar score with seizures, and early neonatal death. However, as pointed out by Devoe (2011a), the design of the Chen et al. study cannot address causality or the nature of the relationship between the use of EFM and the observed outcomes. Moreover, the study did not examine EFM tracings, the labor process, or other myriad circumstances surrounding each birth, and the birth certificate-recorded rate of EFM use was substantially lower than that reported by mothers who have given birth (Declercq, Sakala, Corry & Appelbaum, 2006). Hence, although the study provides some support for the use of EFM, true confirmatory data about improved outcomes when EFM is used during labor are still lacking. Nevertheless, most clinicians prefer EFM as the intrapartum method of fetal assessment, and it is recommended by ACOG (2009a) and the Society of Obstetricians and Gynaecologists of Canada (SOGC) (2007) for high-risk maternal-fetal conditions during labor.
Table 15-1. FETAL HEART RATE CHARACTERISTICS
Term
Definition
Baseline rate
Approximate mean FHR rounded to increments of 5 bpm during a 10-min window excluding accelerations and decelerations and periods of marked variability. There must be ≥2 min of identifiable baseline segments (not necessarily contiguous) in any 10-min window, or the baseline for that period is indeterminate. In such cases, one may need to refer to the previous 10-min window for determination of the baseline.
Bradycardia
Baseline rate of <110 bpm.
Tachycardia
Baseline rate of >160 bpm.
Baseline variability
Determined in a 10-min window, excluding accelerations and decelerations. Fluctuations in the baseline FHR that are irregular in amplitude and frequency and are visually quantified as the amplitude of the peak-to-trough in bpm.
– Absent variability
Amplitude range undetectable.
– Minimal variability
Amplitude range visually detectable but ≤5 bpm. (Greater than undetectable but ≤5 bpm.)
– Moderate variability
Amplitude range 6-25 bpm.
– Marked variability
Amplitude range >25 bpm.
Acceleration
Visually apparent abrupt increase in FHR. Abrupt increase is defined as an increase from onset of acceleration to peak is <30 sec. Peak must be ≥15 bpm and must last ≥15 sec from the onset to return. Acceleration lasting ≥10 min is defined as a baseline change. Before 32 weeks of gestation, accelerations are defined as having a peak ≥10 bpm and duration of ≥10 sec.
Prolonged acceleration
Acceleration ≥ 2 min but <10 min in duration.
Early deceleration
Visually apparent, usually symmetrical, gradual decrease and return of FHR associated with a uterine contraction. The gradual FHR decrease is defined as one from the onset to FHR nadir of ≥30 sec. The decrease in FHR is calculated from onset to nadir of deceleration. The nadir of the deceleration occurs at the same time as the peak of the contraction. In most cases, the onset, nadir, and recovery of the deceleration are coincident with the beginning, peak, and ending of the contraction, respectively.
Late deceleration
Visually apparent, usually symmetrical, gradual decrease and return of FHR associated with a uterine contraction. The gradual FHR decrease is defined as from the onset to FHR nadir of ≥30 sec. The decrease in FHR is calculated from onset to the nadir of deceleration. The deceleration is delayed in timing, with nadir of the deceleration occurring after the peak of the contraction. In most cases, the onset, nadir, and recovery of the deceleration occur after the beginning, peak, and ending of the contraction, respectively.
Variable deceleration
Visually apparent abrupt decrease in FHR. An abrupt FHR decrease is defined as from the onset of the deceleration to beginning of FHR nadir of <30 sec. The decrease in FHR is calculated from the onset to the nadir of deceleration. The decrease in FHR is ≥15 bpm, lasting ≥15 sec, and <2 min in duration. When variable decelerations are associated with uterine contractions, their onset, depth, and duration commonly vary with successive uterine contractions.
Prolonged deceleration
Visually apparent decrease in FHR from baseline that is ≥15 bpm, lasting ≥2 min, but <10 min. A deceleration that lasts ≥10 min is baseline change.
Recurrent
Occurring with ≥50% of contractions in any 20-min window.
Intermittent
Occurring with <50% of contractions in any 20-min window.
Sinusoidal pattern
Visually apparent, smooth, sine wave-like undulating pattern in FHR baseline with cycle frequency of 3-5/min that persists for ≥20 min.
FHR, fetal heart rate.
Adapted from Lyndon, A., O’Brien-Abel, N., & Simpson, K. R. (2009) . Fetal heart rate interpretation. In A. Lyndon & L. U. Ali (Eds.), Fetal Heart Monitoring Principles and Practices (4th ed., p. 105 ). Washington, DC: Association of Women’s Health, Obstetric and Neonatal Nurses/Kendall Hunt; Macones, G. A., Hankins, G. D., Spong, C. Y., Hauth, J. D., & Moore, T. (2008) . The 2008 National Institute of Child Health Human Development workshop report on electronic fetal monitoring: Update on definitions, interpretations, and research guidelines. Obstetrics & Gynecology, 112, 661-666, and Journal of Obstetric, Gynecologic and Neonatal Nursing, 37, 510-515.
DEFINITIONS AND APPROPRIATE USE OF TERMS DESCRIBING FETAL HEART RATE PATTERNS
Appropriate clinical management of variant FHR patterns and effective clinical communication are both enhanced by use of standardized definitions that convey agreed upon meanings among the members of the healthcare team. Adoption of a common language for FHR characteristics and pattern definitions, as well as medical record documentation that is mutually agreed upon and routinely used by all providers, enhances interdisciplinary communication and, therefore, maternal-fetal safety (JCAHO, 2004). Both oral communication and written documentation must accurately convey the clinician’s level of concern and/or record the presumed diagnosis. The chances of miscommunication between care providers, especially during telephone conversations about fetal status, are decreased when everyone is speaking the same language (Simpson & Knox, 2006, 2009). Timely intervention is dependent on clear communication between providers sharing care of an individual patient (Fox, Kilpatrick, King, & Parer, 2000; Miller, 2005; Simpson & Knox, 2009). The NICHD (Macones et al., 2008) nomenclature is the basis for the pattern descriptions in this chapter.
Table 15-2. THREE-TIERED SYSTEM FOR FETAL HEART RATE INTERPRETATION
Classification
Definition
Interpretation
Category I
Includes all of the following characteristics:
Baseline rate 110-160 bpm
Moderate baseline variability
Accelerations present or absent
Late or variable decelerations absent
Early decelerations present or absent
Normal:
Predictive of normal fetal acid-base balance at the time of observation
Category II
All tracings that do not meet criteria for category I or category III
Represents an “appreciable fraction” of tracings encountered in clinical care
Indeterminate:
Not predictive of abnormal fetal acid-base status but cannot be classified as category I or III
Category III
Either:
Absent baseline variability and any of the following: Recurrent late deceleration Recurrent variable decelerations Bradycardia
OR
Sinusoidal pattern
Abnormal:
Associated with abnormal fetal acid-base status at the time of observation
Adapted from Macones, G. A., Hankins, G. D., Spong, C. Y., Hauth, J., & Moore, T. (2008) . The 2008 National Institute of Child Health and Human Development workshop report on electronic fetal monitoring: Update on definitions, interpretation, and research guidelines. Obstetrics and Gynecology, 112(3), 661-666, and Journal of Obstetric, Gynecologic, and Neonatal Nursing, 37(5), 510-515.
The three-tiered classification system for FHR pattern interpretation put forth by the NICHD reflects both the presence and absence of scientific consensus on FHR interpretation (Macones et al., 2008) (see Table 15-2). There is little controversy concerning what constitutes a normal FHR pattern. Most clinicians agree on the definition of a normal (category I) FHR tracing (i.e., baseline rate within 110 to 160 bpm, moderate FHR variability, and absence of late or variable decelerations; accelerations and early decelerations may both be present or absent in a normal tracing). There is good evidence that this type of FHR tracing confers an extremely high predictability of a normally oxygenated fetus when it is obtained (ACOG, 2009a; Macones et al., 2008). Of note, while the presence of spontaneous or induced accelerations is predictive of normal fetal acid-base status at the time of observation, the absence of accelerations is not a reliable predictor of fetal acidemia (Macones et al., 2008).
At the other end of the spectrum from normality, several patterns are likely predictive of current or impending fetal asphyxia so severe that the fetus is at risk for neurologic and other fetal damage or death (Macones et al., 2008). These patterns are classified as abnormal (category III) and include absent baseline FHR variability with recurrent late or variable decelerations or bradycardia, or a sinusoidal FHR pattern. Patterns at this end of the spectrum are considered predictive of abnormal fetal acid-base status and require prompt evaluation and intervention (Macones et al., 2008).
Many fetuses have FHR tracings that are intermediate between these two extremes, and there is no consensus on their presumed condition or clinical management because there is inconsistent evidence in the literature regarding their predictive value in relation to fetal acid-base status. These tracings are classified as indeterminate (category II). Category II tracings include all tracings that are not categorized as category I or category III. This includes tracings demonstrating alterations in baseline (e.g., bradycardia with minimal or moderate variability) and tracings with recurrent late or variable decelerations and minimal or moderate variability, among others. Category II tracings are not considered predictive of abnormal acid-base status at the time they are observed, but they also cannot reliably be placed in category I on the basis of current evidence (Macones et al., 2008). These tracings can be conceptualized as representing some level of fetal physiologic stress. Thus evaluation, attempts to ameliorate or reduce any identified stressors, reevaluation, and close surveillance of these tracings are appropriate (ACOG, 2010b); most clinicians do not wait until the FHR pattern is at the extreme end of abnormality before intervening to attempt to improve fetal status via one or more intrauterine resuscitation techniques (Garite & Simpson, 2011; Simpson, 2007).
A review of the literature on the association between FHR patterns and fetal acidemia found moderate FHR variability was strongly associated with an umbilical cord pH > 7.15 or newborn vigor (5-minute Apgar score ≥ 7). Absent or minimal FHR variability with late or variable decelerations was the strongest predictor of newborn acidemia. The correlation between diminished variability and acidemia was 23%, which the investigators suggest was low because studies reviewed did not always differentiate between decreased and absent variability, and the association with absent variability is likely stronger. The investigators found increasing depth of decelerations was correlated with low pH (<7.15). Acidemia took time to develop except in situations of sudden profound bradycardia. In the context of decreasing variability with recurrent decelerations, newborn acidemia developed over a period of time approaching 1 hour (Parer, King, Flanders, Fox, & Kilpatrick, 2006).
Further data suggest normal fetal status (category I) is associated with normal short-term neonatal outcomes. Based on an analysis of 48,444 EFM tracings of women in term labor in 10 hospitals, babies whose tracings during the last 2 hours prior to birth were exclusively normal (category I) did well, with only 0.6% having Apgar scores <7 at 5 minutes of life and 0.2% having low Apgar scores with neonatal intensive care unit (NICU) admission. However, when more than 75% of the EFM tracing in last 2 hours prior to birth was indeterminate (category II), low Apgar scores at 5 minutes increased to 1.3% of babies and low Apgar score at 5 minutes with NICU admission increased to 0.7% (Jackson, Holmgren, Esplin, Henry, & Varner, 2011).
Analysis of this large database of women in term labor allowed estimation of the frequency of types of EFM tracings based on the NICHD-defined FHR categories (Macones et al., 2008). When all of labor was included, most tracings (77.9%) were normal (category I), 22.1% were indeterminate (category II), and 0.004% were abnormal (category III). During the last 2 hours of labor prior to birth, normal (category I) decreased to 60.9% of the duration, indeterminate (category II) increased to 39.1%, and abnormal (category III) increased to 0.006%. These last 2 hours included women in second-stage labor that had a vaginal or cesarean birth and women that had a cesarean birth without second-stage labor (Jackson et al., 2011). The strength of the association between time in an indeterminate (category II) tracing and the risk of Apgar score less than 7 with a NICU admission in this study did not increase until more than 50% of the last 2 hours of labor were spent in category II. This is consistent with the findings of Parer et al. (2006) that, in the absence of catastrophic events, acidemia develops over a period of time approximating an hour. Thus, there is supportive evidence for the classification system developed by NICHD in relation to presumed fetal acid-base status across a continuum of FHR findings. Ideally, members of the perinatal team have a shared method of interpreting FHR patterns and an agreed upon management guideline for specific FHR patterns (Fox et al., 2000; Knox & Simpson, 2011).
Terms such as stress and distress lack the precise meaning needed to discriminate levels of concern. In 1998, ACOG recommended that nonreassuring fetal status replace the term fetal distress in its committee opinion Inappropriate Use of the Terms Fetal Distress and Birth Asphyxia. This committee opinion was reaffirmed in 2005 (ACOG, 2005b). The three-tiered interpretation system developed by the NICHD EFM expert group was introduced in 2008 (Macones et al., 2008). The term fetal distress has a low positive predictive value, even in high-risk populations, and is often associated with an infant who is in good condition at birth as determined by the Apgar score or umbilical cord blood gas analysis or both. Communication between clinicians caring for the woman and those caring for her baby is best served by categorization of the FHR as normal, indeterminate, or abnormal, followed by a further description of findings when the tracing is indeterminate (category II) or abnormal (category III). Further description should include baseline variability, recurrent variable or late decelerations, prolonged decelerations, fetal tachycardia or bradycardia, maternal risk factors, proximity to birth, and identification of the level of urgency for intervention. It is important that team members explicitly reach and confirm agreement on the necessity of intervention or the parameters for continued close surveillance (Lyndon, Zlatnik, & Wachter, 2011).
Whereas in the past, the term fetal distress generally referred to an ill fetus, categorization of the FHR pattern describes the clinician’s interpretation of data regarding fetal status (i.e., the presumptive relationship between the FHR pattern and fetal acid-base status). The three-tiered categorization scheme acknowledges the imprecision inherent in the interpretation of the data as well as the dynamic nature of the fetal response to labor (Macones et al., 2008). Therefore, the diagnosis of category II or III tracing can be consistent with the birth of a vigorous baby as the predictive value of even category III tracings for neurologic outcome in infants is poor despite indication of increased risk for fetal acidemia (ACOG, 2010b).
Another problematic issue is use of asphyxia and or acidosis when making a presumptive diagnosis of intrapartum hypoxia. Asphyxia means insufficiency or absence of exchange of respiratory gases. The pathologic consequence of asphyxia is injury to the fetal tissues, primarily the brain, with subsequent neurologic impairment. However, asphyxia is a continuum of oxygen deficit that moves from hypoxemia (decreased oxygen content in blood) to acidemia (increased hydrogen ion concentration in blood), then acidosis (increased hydrogen ion concentration in the tissue) (King & Parer, 2000). Hypoxemia and acidemia are detectable via pH measurements of fetal scalp blood or umbilical cord blood at birth. These values reveal the acid-base balance within blood but not within tissue and therefore cannot directly reveal the extent or duration of metabolic acidosis or level of asphyxia in tissue. Thus, the use of terms like asphyxia and acidosis in communication and medical record documentation about characteristics of the FHR and fetal and/or newborn status is both inappropriate and confusing (Fahey & King, 2005) and should be avoided.
TECHNIQUES OF FETAL HEART RATE MONITORING
ASSESSMENT OF UTERINE ACTIVITY
During the intrapartum period, the FHR is interpreted relative to uterine activity. Therefore, interpretation of FHR patterns includes a complete assessment of four components of the uterine contractions: (1) frequency, (2) duration, (3) intensity, and (4) the uterine resting tone between contractions. These assessments can be made by either palpation, external tocodynamometer (tokos is Greek for childbirth), or the use of an intrauterine pressure catheter (IUPC).
Assessment of uterine activity begins with palpation. Contraction frequency is measured from the beginning of one contraction to the beginning of the next and is described in minutes. Duration is the length of the contraction and is described in seconds. Intensity refers to the strength of the contraction and is described as mild, moderate, or strong by palpation, or in millimeters of mercury (mm Hg) or Montevideo units (MVUs) if an IUPC is used. Uterine resting tone is assessed in the absence of contractions or between contractions. By direct palpation, resting tone is described as soft or hard and via IUPC in terms of mm Hg or MVUs. As with any procedure, the least invasive approach is preferred unless maternal-fetal status indicates a need for more precise data.
Each technique has some limitations. Intensity cannot be determined with a tocodynamometer. The tocodynamometer detects pressure changes from the tightening of the fundus during contractions through the maternal abdomen. This technique gives a relatively accurate reading of the duration and frequency of contractions but is unable to assess intensity or resting tone. Thus, manual palpation is an essential component of external uterine activity monitoring (Harmon, 2009). With an IUPC, the peak of the contraction as indicated on the fetal monitor tracing depicts the actual strength of the contraction measured in mm Hg pressure within the amniotic fluid. The IUPC is most accurate because direct measurement of intraamniotic pressure is recorded, but it requires ruptured membranes for insertion, and technical difficulties requiring troubleshooting are not uncommon (Harmon, 2009).
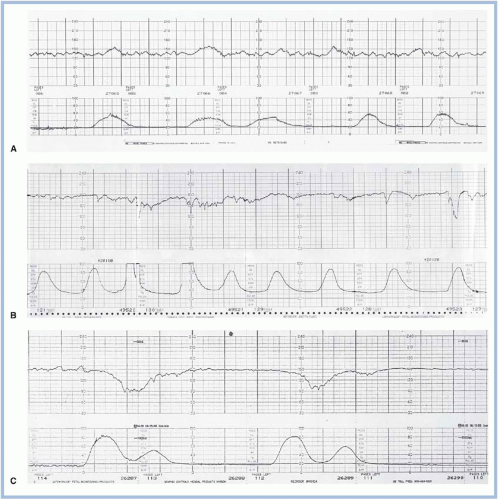
Normal contraction characteristics in the active phase of labor include frequency every 2 to 3 minutes, duration of 80 to 90 seconds, and strong to palpation (Clark, Simpson, Knox, & Garite, 2009). Both contraction characteristics and labor progress are evaluated to determine the adequacy of uterine activity. Some uterine activity patterns are dysfunctional or inadequate for generating progress in labor (Fig. 15-1 A-C). Normal uterine activity is defined as less than or equal to five contractions in 10 minutes averaged over 30 minutes; tachysystole is defined as more than five contractions in 10 minutes averaged over 30 minutes (Macones et al., 2008). Clarke et al. (2009) propose consistent achievement of 200 to 220 MVUs as an indication of adequate labor forces in women receiving oxytocin; however, excessive uterine activity should be avoided to minimize risk of fetal harm. There is an association between higher MVUs and risk of neonatal acidemia at birth. In a study of 1,433 FHR and uterine activity patterns, babies of women with MVUs averaging 236 during first-stage labor were not acidemic at birth, whereas babies of mothers with MVUs averaging 261 had an umbilical artery pH of 7.11 or less (Bakker, Kurver, Kuik, & Van Geijn, 2007). Tachysystole can be spontaneous as a result of endogenous maternal oxytocin or prostaglandins; however, it is more often seen during exogenous stimulation with agents used in cervical ripening and induction and augmentation of labor (Simpson, 2009a).
Coupling or tripling refers to a pattern of two or three contractions with little or no interval followed by a regular interval of approximately 2 to 5 minutes. This pattern may be indicative of a dysfunctional labor process and saturation or down-regulation of uterine oxytocin receptor sites (Dawood, 1995; Phaneuf, Rodriguez Linares, TambyRaja, MacKenzie, & Lopez Bernal, 2000; Zeeman, Khan-Dawood, & Dawood, 1997). If coupling or tripling occurs, a suggested intervention to promote normal uterine activity is temporary discontinuation of oxytocin, maternal repositioning, and an intravenous (IV) fluid bolus of lactated Ringer’s solution with resumption of oxytocin after 30 to 60 minutes.
EXTERNAL DOPPLER VERSUS FETAL SCALP ELECTRODE
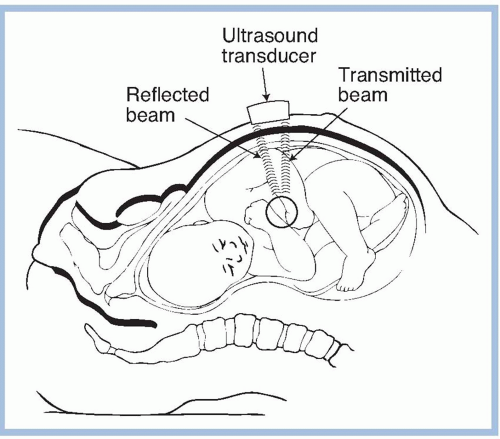
The FHR can be detected via a Doppler ultrasound transducer or fetal electrode. Leopold’s maneuvers are used to determine the fetal position prior to applying the Doppler transducer (see Chapter 14). The Doppler transducer is applied to the maternal abdomen over the fetal back or chest and transmits a high frequency ultrasound. The transducer detects the ultrasound wave that is bounced back off the fetal heart and then counts the FHR by measuring the shift in ultrasound wave frequency between the generated wave and the returning wave reflected off the moving heart (Fig. 15-2). The resulting “Doppler shift” waveform goes through “autocorrelation,” where it is digitized, smoothed, compared with adjacent wave forms, and averaged over three consecutive heartbeats to produce the FHR. This signal is amplified and converted by the monitor to both visual and auditory output of the FHR (Harmon, 2009). The ultrasound wave will not conduct to the fetus if there is air between the emission of the wave and the object it is reflecting off. Gel applied to the transducer helps eliminate air between the transducer and maternal abdomen.
FIGURE 15-1. Three types of uterine contractions. A, Normal contraction frequency, duration, and intensity and uterine resting tone. B, Tachysystole. C, Coupling of contractions.
In the United States, the monitor plots the calculated FHR on paper that is moving at 3 cm/min, or on a graphic computer representation of monitor paper moving at the same speed. Because there is variability in the time interval between heartbeats in a normally oxygenated fetus, the line produced over time has a jagged, irregular appearance resulting from the different rates of consecutive recorded heartbeats. Early Doppler technology tended to exaggerate the FHR variability, but improvements in technology have resulted in a Doppler recording that sufficiently reflects the true variability in the FHR under observation. In some other countries, the recording speed may be set at 1 cm/min, changing the appearance of the FHR patterns observed. Although the Doppler is easy to apply, maternal or fetal movement, uterine contractions, or maternal positions can interrupt a continuous recording. In cases where the mother is significantly overweight, a continuous recording via external monitoring may be challenging.
FIGURE 15-2. The Doppler ultrasound device for detecting cardiac activity. The frequency of the reflected beam is changed when it is reflected from a moving structure. (Adapted from Parer, J. T. [1997]. Handbook of Fetal Heart Rate Monitoring [2nd ed., p. 104]. Philadelphia: W.B. Saunders. Used with permission.)
The direct fetal scalp electrode (FSE) is the most accurate way to assess the FHR but is invasive and should not be used unless the cervix is at least 2 to 3 cm dilated and the membranes have ruptured. The electrode has three leads, which detect the PQRST complex. The filter within the electronics of the machine removes all components except the R wave. The R wave then triggers the machine to count; it waits for a second complex, filters all but the R wave, and then calculates how much time elapsed from the first to the second R wave in a fashion similar to the technique used with Doppler ultrasound. The elapsed time between R intervals is converted into bpm, and the pen records that rate on the paper. Both Doppler ultrasound and FSE are appropriate methods for electronic detection and interpretation of FHR patterns (Macones et al., 2008).
It is important to avoid confusing the maternal heart rate with the FHR. Clinical conditions that increase risk of confusion include low FHR baseline, maternal pushing efforts during second-stage labor, maternal repositioning, maternal obesity, and maternal tachycardia, which may be associated with an elevated temperature, anxiety, or medications (Neilson, Freeman, & Mangan, 2008; Simpson, 2011). An abrupt change in the characteristics of the FHR tracing or FHR accelerations consistently coincident with uterine contractions or with maternal pushing efforts should be evaluated to confirm that the tracing is of fetal origin. In the case of fetal demise, a recording may be produced of the maternal heart rate either via the external ultrasound transducer detecting maternal aortic pulsations or via the FSE detecting the maternal ECG. When there are two sources of data (e.g., maternal heart rate via pulse oximetry and fetal or maternal heart rate via external ultrasound or via FSE), the fetal monitor may display coincident alerts to suggest that both data sources are detecting the same heart rate. When these alerts are displayed, confirmation of two distinct heart rates, one from the fetus and one from the mother, should be undertaken. Potential strategies to minimize risk of confusing maternal heart rate with FHR include confirming maternal heart rate by palpation of maternal pulse during initiation of EFM and comparing it with FHR, repeating this confirmation periodically during first- and second-stage labor, paying close attention to distinguishing between maternal heart rate and FHR during second-stage pushing efforts, and recognizing other clinical situations that could result in maternal heart rate being recorded as FHR such as extremes of maternal weight (Simpson, 2011).
Both Doppler ultrasound and FSEs can produce FHR recordings that are inadequate for interpretation. Use of EFM during labor requires knowledge of sources of artifact and solutions for resolution. Many times, the problem is secondary to equipment malfunction and can be remedied easily. The most common reasons why FHR tracings do not record accurately, the FHR tracing that is produced, and the solutions to the problems are listed in Table 15-3. In November 2009, the U.S. Food and Drug Administration (FDA) issued a recall of specific models of fetal monitors and sent a letter to healthcare providers outlining potential problems. The FDA (2009) noted that the following technical issues had been reported: switching between the FHR and maternal heart rate, halving of the FHR, a mismatch between the audible and printed FHR, false decelerations, and noisy or erratic signals. The concern was that clinical decisions based on unrecognized inaccuracies in the FHR tracing could lead healthcare professionals to perform unnecessary interventions such as cesarean birth, could fail to identify the need for interventions, and/or could fail to identify and treat fetal compromise (FDA, 2009).
Application of an FSE is invasive and increases risk of maternal-fetal infection. Therefore, it should be used only when continuous recordings are indicated and are unable to be obtained with external monitoring. If the recording obtained via external EFM is continuous, there is no need for an FSE as there is no clinical difference in data interpretation. There is evidence to suggest that application of a direct electrode could enhance maternal-fetal transmission of HIV when used in women who are HIV seropositive (Maiques, Garcia-Tejedor, Perales, & Navarro, 1999); therefore, use of an FSE is contraindicated in women who are known to be HIV seropositive (American Academy of Pediatrics [AAP] & ACOG, 2012). Other relative contraindications to the application of a direct fetal lead include women who have active or chronic hepatitis, group B streptococcus, and herpes simplex virus (HSV) or other known and nontreated sexually transmitted diseases (Phillips, n.d.). While the indicted use of an FSE may be reasonable in the setting of HSV without active lesions (AAP & ACOG, 2012), current recommendations are to avoid techniques that result in a break in the skin when these infectious agents are known to be present (AAP & ACOG, 2012; Maiques et al., 1999). Application of a direct fetal lead also may be deferred for women who are known hemophilia carriers and fetal carrier status is either confirmed or unknown (Phillips, n.d.).
Table 15-3. SOURCES OF ARTIFACT OR ERROR IN FETAL HEART RATE RECORDINGS
Recording Produced
Solution
Signal errors
Faulty leg plate, electrode, or monitor
No recording.
Replace equipment.
Transducer does not detect fetal heart
Maternal muscle movements
Uterine contractions
Maternal positioning
Maternal obesity
Intermittent recording consistently.
Move transducer.
Interference by maternal signal
Recording will be maternal heart rate.
Recognize maternal heart beat and use alternative method or adjust placement of transducer.
Limitation of machinery
Counting process omits FHR that is >30 bpm different from preceding beat
Arrhythmia will be audible but does not appear on record.
Use fetal ECG if improved recording needed. Arrhythmias tend to be regular, and artifact tends to be irregular.
Halving or doubling of audible FHR
Very slow rates may be doubled and very fast rates (>240 bpm) may be halved.
Auscultate to determine correct rate.
Interpretive errors
Maternal heart rate recorded
Fetal death
Electrode on cervix
Rate recorded will equal maternal pulse EFM may provide electronic cues that recording is maternal in nature.
Compare with maternal pulse. Palpate maternal pulse.
Scaling error
Two paper speeds are possible on some machines (1 and 3 cm/min). FHR pattern will change at slower speed, exaggerating variability.
Ensure paper speed of 3 cm/min prior to applying transducers
Adapted from Parer, J. T. (1997) . Handbook of Fetal Heart Rate Monitoring (2nd ed.). Philadelphia: W. B. Saunders.
INTERMITTENT AUSCULTATION
Prior to the introduction of Doppler technology, IA of the FHR was accomplished with a Pinard or DeLee stethoscope. A baseline FHR can be obtained, and the presence or absence of decelerations can be noted without determination of variability or the type of deceleration with this technique. Auscultation with a non-Doppler stethoscope is no longer common practice in the United States. Today, when the FHR is assessed during labor via an IA protocol, a handheld Doppler unit is typically used (Display 15-1). There is limited evidence to suggest improved outcomes for fetuses of women assessed via EFM as compared to IA; thus, IA is an appropriate (ACOG, 2010b) and, in some cases, preferred (SOGC, 2007) method of FHR monitoring. SOGC (2007) recommends IA as the primary method of FHR monitoring for women with uncomplicated pregnancy and labor. However, ACOG (2010a), ACNM (2010a), and SOGC recommend that continuous EFM be used for high-risk women, and ACOG suggests women receiving oxytocin be monitored as for high-risk conditions (AAP & ACOG, 2012; ACOG, 2009b). SOGC recommends EFM for augmentation of labor and suggests EFM may be appropriate for labor induction.
Current recommendations for using auscultation during the intrapartum period are outlined by AWHONN (Feinstein, Sprague, & Trepanier, 2008), ACNM (2010a), ACOG (2009a), SOCG (2007), and in the Guidelines for Perinatal Care (AAP & ACOG, 2012). However, there are inconsistencies in the recommendations from AAP, ACOG, AWHONN, ACNM, and SOGC regarding patients for whom IA is appropriate and the frequency of assessment when using IA. Because protocols in clinical trials varied, AWHONN suggests auscultation of the FHR every 15 to 30 minutes in the active phase of the first stage of labor and every 5 to 15 minutes in the active phase of the second stage of labor (AWHONN, 2009; Feinstein et al., 2008). ACOG suggests an assessment frequency for IA of every 30 minutes in the active phase of the first stage of labor and every 15 minutes in the second stage of labor for women without identified risk factors (AAP & ACOG, 2012); and at least every 15 minutes in the active phase of first-stage labor and at least every 5 minutes during second-stage labor for women with identified risk factors (ACOG, 2009a). SOGC (2007) recommends assessment hourly in latent labor, every 15 to 30 minutes in the active phase of first-stage labor, and every 5 minutes during second-stage labor. ACNM recommends auscultation every 15 to 30 minutes in the active phase of the first stage of labor, every 15 minutes in second stage prior to pushing, and every 5 minutes while pushing (ACNM, 2010a). No clinical trials have examined methods of fetal assessment during the latent phase of labor. The variation in recommendations among professional societies reflects the variation in protocols used for clinical trials and the mix of both low- and high-risk patients in most trials. Therefore, clinical judgment and unit policy should guide decisions when deciding the method and frequency of fetal assessment. When auscultation is used as the primary method of fetal surveillance during labor, a 1:1 nurse-fetus ratio is required (ACNM, 2010a; AWHONN, 2009). Categories for interpretation of IA findings are listed in Table 15-4.
Table 15-4. CLASSIFICATION & INTERPRETATION OF AUSCULTATED FHR
Characteristics
Interpretation
Category I
All of the following:
Normal FHR baseline between 110 and 160 bpm
Regular rhythm
Presence of FHR increases or accelerations from the baseline
Absence of FHR decreases of decelerations from the baseline
Normal:
Normal auscultated FHR characteristics are predictive of fetal well-being at the time of observation.
Category II
Any of the following:
Irregular rhythm
Presence of FHR decreases or decelerations from the baseline
Tachycardia (baseline >160 bpm >10 min in duration)
Bradycardia (baseline <110 bpm >10 min in duration)
Indeterminate:
Findings cannot be classified as abnormal, as variability cannot be determined by auscultation. These findings require evaluation, ongoing surveillance, and reevaluation consistent with overall clinical circumstances. In emergent situation (e.g., bradycardia), preparations to expedite birth should occur simultaneously with efforts to ameliorate and verify the nature of the FHR findings.
FHR, fetal heart rate.
Adapted from Lyndon, A., O’Brien-Abel, N., & Simpson, K. R. (2009) . Fetal heart rate interpretation. In A. Lyndon & L. U. Ali (Eds.), Fetal Heart Monitoring Principles and Practices (4th ed., pp. 101-133 ). Washington, DC: Association of Women’s Health, Obstetric and Neonatal Nurses/Kendall Hunt.
The decision to use IA or EFM is made in collaboration with the laboring woman, as there remains a lack of consistent, high-quality evidence to definitively recommend one approach over the other (Devoe, 2011a). The decision is based on many factors, including patient history, fetal condition, risk classification, and hospital policies and procedures. As with EFM, there are benefits and limitations to the use of IA ( Display 15-2). Both IA and EFM are effective in fetal evaluation when used appropriately (AAP & ACOG, 2012; ACNM, 2010a; ACOG, 2010b; AWHONN, 2009; SOGC, 2007).
PHYSIOLOGIC BASIS FOR FETAL HEART RATE MONITORING
EFM is a technique for assessing the adequacy of fetal oxygenation. As previously noted, while a normal FHR tracing (category I) is a good predictor of a normoxic fetus, the reverse is not true. Because the high rate of false-positive indeterminate and abnormal FHR tracings has many origins and several clinical implications, a working knowledge of FHR physiology can aid clinical interpretation of FHR patterns during labor. The following section reviews the importance of maternal oxygenation, uteroplacental exchange, umbilical blood flow, and factors influencing FHR regulation. Subsequently, we review the characteristics of the normal FHR, interventions for managing alterations in FHR, and FHR pattern evolution.
DISPLAY 15-2 Benefits and Limitations of Auscultation
BENEFITS
Neonatal outcomes are comparable to those with EFM based on current RCTs.
Lower cesarean birth rates have been associated with auscultation than with EFM in some RCTs.
The technique is less invasive.
The patient’s freedom of movement is increased.
The technology allows for fetal heart assessment if the patient is immersed in water.
The equipment is less costly than EFM equipment.
Auscultation is not automatically documented on paper (often a source of debate in legal situations).
A caregiver must be present at the bedside to provide the 1:1 nurse-to-patient ratio that is recommended based on RCTs comparing auscultation and EFM.
LIMITATIONS
Use of a fetoscope may limit the ability to hear the FHR (e.g., in cases of maternal obesity or increased amniotic fluid volume).
Certain FHR characteristics associated with EFM (e.g., variability and types of decelerations) cannot be detected.
Some patients may feel that auscultation is more intrusive.
Auscultation is not automatically documented on paper (as EFM is, which is perceived as an important piece of documentation by many practitioners).
There is a potential need to increase or realign staff to meet the 1:1 nurse-to-patient ratio that is recommended based on RCTs comparing auscultation and EFM.
Fetal oxygenation depends on well-oxygenated maternal blood flow to the placenta. Adequate maternal hemoglobin levels, adequate maternal oxygen saturation (SaO2), and adequate oxygen tension in maternal arterial blood PaO2 are needed to for fetal oxygenation. While most pregnant women are healthy and well-oxygenated, maternal conditions that may impair oxygen delivery to the fetus include severe anemia, asthma, congenital cardiac defects, congestive heart failure, lung disease, or seizures.
UTERINE, PLACENTAL, AND UMBILICAL BLOOD FLOW
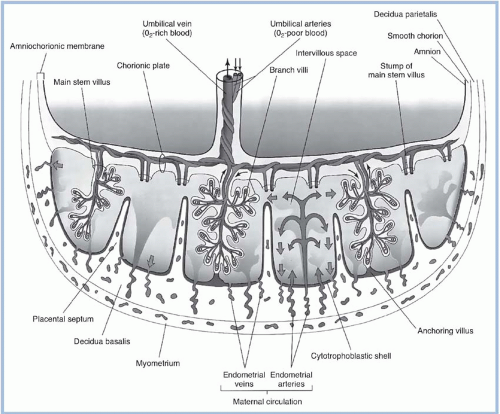
Adequate uterine blood flow is required for the passage of respiratory gases and substances across the placenta. Uterine blood flow increases throughout pregnancy and in a singleton pregnancy at term is approximately 700 mL/min or 10% to 15% of maternal cardiac output (Blackburn, 2007; Parer, 1997). While uterine blood also supplies the myometrium and endometrium, the intervillous space within the placenta receives 70% to 90% of the total uterine blood flow near term (Parer, 1997). In the intervillous space, well-oxygenated maternal blood propelled by maternal arterial blood pressure surrounds the fetal chorionic villi, allowing exchange of oxygen, carbon dioxide, and other substances between the maternal and fetal circulations (Fig. 15-3). The newly oxygenated fetal blood within the fetal villi flows into veins that converge into a single umbilical vein, which carries the oxygenated blood and nutrients to the fetus. Deoxygenated blood and waste products return from the fetus to the placenta via two umbilical arteries, which divide successively into smaller vessels, eventually creating an arteriovenous system within each chorionic villus (Blackburn, 2007).
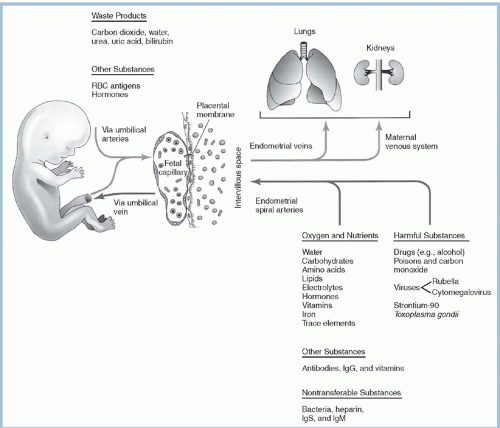
Maternal-fetal exchange of oxygen, carbon dioxide, nutrients, waste products, water, and other substances is facilitated by the large surface area of the placental membrane separating the maternal and fetal blood (Fig. 15-4). Mechanisms by which these substances transfer across the placental membrane include passive diffusion, facilitated diffusion, active transport, hydrostatic pressure, breaks or leaks, and pinocytosis. Oxygen and carbon dioxide are exchanged rapidly by passive diffusion. Passive diffusion allows movement down the concentration gradient from an area of high concentration, across a membrane, to an area of lower concentration. The concentration gradients and characteristics of fetal hemoglobin favor transfer of oxygen from mother to fetus and transfer of carbon dioxide from fetus to mother.
Clinical factors that can potentially decrease uteroplacental perfusion and fetal oxygenation include excessive uterine contractions or hypertonus; maternal hypotension or hypertension; placental changes due to decreased surface area, degenerative changes, infarcts, calcification, infection, or edema; and vasoconstriction. In addition, umbilical cord entanglement, compression, or occlusion may impede fetal oxygenation. Therefore, a primary goal in intrapartum care is to maximize uterine blood flow, uteroplacental exchange, and umbilical blood flow, thereby minimizing risk to the fetus.
FETAL HEART RATE REGULATION
The cardioregulatory center in the medulla oblongata interacts with the parasympathetic and sympathetic branches of the autonomic nervous systems, baroreceptors, chemoreceptors, fetal hormones, sleep/wake cycles, breathing movements, painful stimuli, sound vibrations, and temperature to influence FHR (O’Brien-Abel, 2009). Major factors believed to influence the integration of FHR control are outlined in Table 15-5. Interplay between the two components of the autonomic nervous system (sympathetic and parasympathetic), higher cortical functions in the brain, and chemoreceptors and baroreceptors are all reflected in the baseline rate and, in part, make up the FHR variability seen on the recording from an FHR monitor.
FIGURE 15-3. Schematic drawing of a transverse section through a full-term placenta showing maternal uteroplacental circulation and fetal-placental circulation. (From Moore, K. L., & Persaud, T. V. N. [2003]. The Developing Human: Clinically Oriented Embryology [7th ed., p. 126]. Philadelphia: Saunders. Used with permission from Elsevier.)
Sympathetic nervous system fibers are widely distributed throughout the fetal myocardium at term. Stimulation of these nerve fibers releases norepinephrine, causing increased heart rate, strength of cardiac contractions, and cardiac output (Parer, 1997; Nageotte & Gilstrap, 2009). The average baseline FHR in the normal fetus at 20 weeks’ gestation is 155 bpm; at 30 weeks, 144 bpm; and at term before labor, 140 bpm (Nageotte & Gilstrap, 2009). This slow, gradual decrease in FHR seen with advancing gestational age is due to an increased dominance of the parasympathetic over the sympathetic branch of the autonomic nervous system. While the sympathetic branch is dominant in an extremely premature fetus, a baseline FHR greater than 160 bpm should be further evaluated to rule out fetal compromise, rather than assuming the tachycardia is secondary to prematurity (Freeman, Garite, & Nageotte, 2003).
The parasympathetic nervous system influences the fetal heart via the vagus nerve, which innervates the sinoatrial (SA) and atrioventricular nodes within the heart. Stimulation of the vagus nerve releases acetylcholine, which decreases firing of the SA node, resulting in a slower heart rate in a normal fetus (Dalton, Phill, Dawes, & Patrick, 1983; Parer & Nageotte, 2004). With advancing gestational age, this vagal influence results in approximately 10 bpm difference in baseline FHR between 28 and 30 weeks’ gestation and term. The second important function of the parasympathetic system is the transmission of FHR variability. Vagal stimulation of the SA node is the primary influence in the transmission of impulses causing FHR variability. Because severe hypoxia and metabolic acidosis will decrease central nervous system (CNS) function, the presence of moderate FHR variability reliably indicates a well-oxygenated, nonacidemic fetus (ACOG, 2010b; Garite, 2007; Macones et al., 2008).
FIGURE 15-4. Transfer of substances between the mother and the fetus across the placental membrane. Ig, immunoglobulin; RBC, red blood cell. (From Moore, K. L., & Persaud, T. V. N. [2003]. The Developing Human: Clinically Oriented Embryology [7th ed., p. 128]. Philadelphia: Saunders. Used with permission from Elsevier.)
Chemoreceptors, located centrally in the medulla oblongata and peripherally in the aortic arch and carotid sinuses, have their greatest effect on the regulation of respiration and in the control of circulation (Nageotte & Gilstrap, 2009; Parer, 1997). When uteroplacental blood flow falls below the threshold needed for normal respiratory gas exchange, increased carbon dioxide tension (PCO2) in fetal vessels stimulates the chemoreceptors to fire, resulting in slowing of the FHR (Freeman et al., 2003). The influence of chemoreceptors may be seen in the mechanism of late decelerations and in variable decelerations with hypoxemia.
Baroreceptors, located in the aortic arch and carotid sinuses, are small stretch receptors that quickly detect increases in fetal arterial blood pressure (Nageotte & Gilstrap, 2009; Parer, 1997). When umbilical blood flow is occluded, fetal arterial blood pressure quickly increases, triggering the baroreceptors to send impulses via the vagus nerve to the midbrain to abruptly decrease the FHR, cardiac output, and blood pressure, thereby protecting the fetus. The influence of baroreceptors may be seen in the mechanism of variable decelerations.
Table 15-5. FACTORS INFLUENCING FETAL HEART RATE CONTROL
Influence
Action
FHR Effect
Cardioregulatory center
Collection of neurons in ventral and lateral surface of medulla oblongata
Integrating source for control of FHR
Interacts with parasympathetic and sympathetic nervous systems, baroreceptors, chemoreceptors, fetal hormones, sleep/wake cycles, breathing movements, painful stimuli, sound, vibrations, and temperature to influence FHR
Baseline rate, variability, and various FHR patterns provide indirect insights into functioning of CNS
Presence of FHR variability represents an intact nervous pathway through cerebral cortex, midbrain, vagus nerve, and normal cardiac conduction system
Parasympathetic branch of the autonomic nervous system
Originates in medulla oblongata
Vagus nerve (10th cranial) innervates SA and AV nodes
Stimulation releases acetylcholine
Pathway for transmission of variability
↓FHR
Slow, gradual ↓ FHR with ↑ gestational age (approximately 10 bpm difference in baseline FHR between 28 wk and term)
Maintains transmission of beat-to-beat variability
Moderate variability indicates absence of severe hypoxia or metabolic acidosis
Modulates baseline FHR with sympathetic
Sympathetic branch of the autonomic nervous system
At term, nerve fibers widely distributed throughout myocardium
Reserve mechanism to improve the heart’s pumping ability during intermittent stress
Catecholamines can also cause fetal vasoconstriction and hypertension
↑ FHR
Blocking with propranolol results in ↓ FHR of approximately 10 bpm
Modulates baseline FHR with parasympathetic nervous system
Baroreceptors
Protective, stretch receptors
Located in aortic arch and carotid sinuses at bifurcation of external and internal carotid arteries
When ↑ arterial BP, the baroreceptors quickly detect amount of stretch, sending impulses via vagus nerve to midbrain
Impulses return via vagus nerve, causing sudden ↓ FHR, ↓ CO, and ↓ BP, thereby protecting fetus
Abrupt ↓ FHR
Abrupt ↓ CO
Abrupt ↓ BP
Variable decelerations with moderate variability are baroreceptor influenced
Chemoreceptors
In the adult
In the fetus:
Central—located in medulla oblongata
Peripheral—in aortic arch and carotid sinuses
When arterial blood perfusing chemoreceptors contains ↑ PCO2 or ↓ PO2:
○ Central chemoreceptors respond with reflex tachycardia and hypertension, most likely in an attempt to circulate blood and ↓ the PCO2
○ Peripheral chemoreceptors respond with bradycardia
Interaction of central and peripheral chemoreceptors poorly understood
Combined effect is slowing of FHR
Described in mechanism of late decelerations and in variable decelerations resulting from umbilical arterial occlusion coupled with hypoxemia
When blood flow is below threshold for normal respiratory gas exchange, ↑ PCO2 stimulates chemoreceptors to slow FHR
Hormonal regulation
Epinephrine and norepinephrine secreted from the adrenal medulla
Arginine vasopressin secreted from posterior pituitary
Renin-angiotensin-aldosterone secreted from kidneys
In response to stressful situations, compensatory response shunts blood away from less vital organs and toward brain, heart, and adrenal glands
In adult, responds to ↓ plasma volume, ↑ plasma osmolarity
In fetal sheep, hypoxemia most potent stimulus; distributes blood flow
Responds to ↓ plasma volume or ↓ BP; protects fetus from hemorrhagic stress by stimulating vasoconstriction
↓ FHR, ↑ strength of cardiac contractions, ↑ CO, ↑ arterial BP
↑ FHR, ↑ CO, ↑ arterial BP
Sinusoidal heart rate pattern in experimental studies
↑ FHR, ↑ CO, ↑ arterial BP
Frank-Starling mechanism
In the adult, CO = HR × SV
SV is influenced by Frank-Starling mechanism, which states that ↑ inflow of blood into heart stretches cardiac muscle, thereby resulting in ↑ force of contraction and ↑ SV
In the fetus, this mechanism has not been found to apply on the basis of studies involving fetal and adult lambs
Compared with adult, fetal SV does not fluctuate significantly
Fetal CO ≈ HR
Modest variations in baseline FHR probably have little effect on fetal CO
However, during FHR >240 bpm or FHR <60 bpm, fetal CO is substantially decreased
AV, atrioventricular; BP, blood pressure; CNS, central nervous system; CO, cardiac output; FHR, fetal heart rate; HR, heart rate; PCO2, partial pressure of carbon dioxide; PO2, partial pressure of oxygen; SA, sinoatrial; SV, stroke volume.
From O’Brien-Abel, N. (2009) . Physiologic basis for fetal monitoring. In A. Lyndon & L. U. Ali (Eds.), Fetal Heart Monitoring Principles and Practices (4th ed., pp. 35-36 ). Washington, DC: Association of Women’s Health, Obstetric and Neonatal Nurses/Kendall Hunt. Used with permission.
Fetal monitoring is an ongoing indirect assessment of physiologic factors affecting fetal oxygenation and thereby fetal acid-base status. Uteroplacental blood flow, intervillous space perfusion, umbilical blood flow, and intrinsic influences of parasympathetic and sympathetic nervous system, baroreceptors, and chemoreceptors are reflected in the characteristics of the observed FHR. Ongoing assessment and interpretation of FHR characteristics are used to determine fetal oxygenation and rule out fetal acidemia.
CHARACTERISTICS OF THE NORMAL FETAL HEART RATE
FHR pattern interpretation involves assessment of five components of the FHR as well as the relationship of FHR characteristics to both uterine activity and the overall clinical situation. Characteristics of the FHR to be evaluated include (1) baseline rate, (2) FHR variability, (3) presence or absence of accelerations, (4) other periodic and/or episodic changes, and (5) evolution over time (Macones et al., 2008). Periodic and episodic changes refer to accelerations and decelerations. Periodic changes in FHR occur in response to uterine activity. Episodic changes are not associated with uterine activity and may occur randomly. This section reviews the characteristics of the normal FHR (category I tracings), and the next section will review the etiology and management of the most common periodic and episodic changes seen in category II and III tracings, as well as some other less common alterations in FHR.
BASELINE RATE
The baseline FHR is the approximate mean FHR rounded to increments of 5 bpm during a 10-minute segment, excluding periodic or episodic changes, periods of marked FHR variability, and segments of the baseline that differ by >25 bpm (Macones et al., 2008). In determining the baseline rate, at least 2 minutes of identifiable baseline are required, although they do not need to be contiguous. If, during a 10-minute segment, there are not at least 2 minutes of identifiable baseline, the baseline for that period is indeterminate. In this case, one may need to refer to the previous 10-minute segment(s) for determination of the baseline. The normal baseline FHR range is 110 to 160 bpm (Macones et al., 2008). Bradycardia is a baseline FHR <110 bpm; tachycardia is a baseline FHR >160 bpm (Macones et al., 2008). Since the baseline is determined over a 10-minute period, a baseline change has occurred once the change in FHR has been sustained for at least 10 minutes. Periodic and episodic changes are quantified relative to the most recently determined adjacent baseline FHR.
VARIABILITY
Variability is a characteristic of the FHR baseline defined as fluctuations in the baseline FHR that occur with irregular amplitude and frequency (Macones et al., 2008). The FHR of the healthy fetus is displayed as an irregular line on the monitor tracing. These irregularities demonstrate the FHR variability, which reflects the slight difference in time interval between successive heartbeats (short-term component), and cyclic fluctuations over time (long-term component). The irregular fluctuations of the FHR are visually quantitated as the amplitude of the peak-to-trough in beats per minute as follows:
Absent variability has an amplitude range that is undetectable.
Minimal variability has an amplitude range that is detectable, but less than or equal to 5 bpm.
Moderate variability has an amplitude range of 6 to 25 bpm.
Marked variability has an amplitude range greater than 25 bpm.
Clinically, variability is visually determined as a unit without separating short- and long-term components (Macones et al., 2008; NICHD, 1997). As a characteristic of the baseline, variability is assessed during the baseline and not during periodic changes such as decelerations.
ACCELERATIONS
Accelerations may be present or absent in a normal (category I) FHR tracing. Accelerations are visually apparent abrupt increases (defined as onset of acceleration to peak in < 30 seconds) in FHR above the baseline (Fig. 15-5). The acme is at least 15 bpm above the baseline, and the acceleration lasts at least 15 seconds but less than 2 minutes from the onset to return to baseline (Macones et al., 2008). The FHR only needs to reach a peak ≥ 15 bpm above baseline with onset-return criteria as described previously; it does not need to be sustained at ≥ 15 bpm above baseline. Before 32 weeks of gestation, accelerations are defined as having an acme of at least 10 bpm above the baseline and duration of at least 10 seconds (Macones et al., 2008). Like moderate variability, the presence of accelerations indicates central oxygenation and predicts the absence of fetal metabolic acidemia (ACOG, 2009a; Clark, Gimovsky, & Miller, 1984; Macones et al., 2008). Accelerations can occur as periodic or episodic changes in the FHR. The absence of accelerations is not a reliable predictor of fetal acidemia (Macones et al., 2008).
EARLY DECELERATIONS
Early decelerations may or may not be present in a normal (category I) FHR tracing (Macones et al., 2008). Early decelerations are characterized by a visually apparent gradual (defined as onset of deceleration to nadir ≥30 seconds) decrease and return to baseline FHR associated with a uterine contraction. Early decelerations are typically symmetrical and coincident in timing with the uterine contraction; in most cases, the onset, nadir, and recovery of the deceleration are coincident with the beginning, peak, and ending of the contraction, respectively (Macones et al., 2008).
Early decelerations are presumed to be a response to fetal head compression. Altered cerebral blood flow causes the decrease in heart rate through a vagal reflex. When the contraction occurs, pressure on the fetal head stimulates the vagus nerve. The heart rate begins to drop at the onset of the contraction when the head compression begins and returns to the baseline rate at the end of the contraction when the head is no longer compressed (Freeman et al., 2003). Early decelerations are benign, requiring no intervention or treatment and are not associated with fetal hypoxia or low Apgar scores. The key to assessment of early decelerations is to make sure one distinguishes them from late decelerations. The presence of variability is a key clinical factor. Vagal stimulation occurs as a result of head compression, not secondary to hypoxemia, and will not result in a decrease in variability.
FIGURE 15-5. Accelerations of the fetal heart rate.
UTERINE ACTIVITY
Uterine activity is a key characteristic for interpretation of the overall clinical picture and the FHR pattern. Uterine activity is quantified by determining the number of contractions present in a 10-minute segment averaged over 30 minutes (Macones et al., 2008). Uterine activity should be further characterized in terms of contraction duration and intensity and the quality and duration of resting tone (Lyndon, O’Brien-Abel, & Simpson, 2009; Macones et al., 2008). The frequency of uterine activity is classified as either normal or tachysystole (Macones et al., 2008):
Normal uterine activity is ≤ 5 or fewer contractions
in 10 minutes, averaged over 30 minutes.
Tachysystole occurs when there are > 5 contractions in 10 minutes, averaged over 30 minutes.
Tachysystole is further characterized by the presence or absence of FHR decelerations.
Although the definition for tachysystole includes an averaging of contractions over a 30-minute period, this is not meant to imply that 30 minutes is required before tachysystole can be determined or that interventions to decrease uterine activity should be delayed until tachysystole has been occurring for 30 minutes. One or two 10-minute segments of more than five contractions is sufficient to identify excessive uterine activity and initiate appropriate interventions.
INTERVENTIONS FOR INDETERMINATE OR ABNORMAL FETAL HEART RATE PATTERNS
Before discussing the etiology and individual management of periodic or episodic changes in the FHR, a general review of the initial assessment and interventions used to maximize fetal oxygenation in the presence of variant FHR patterns is warranted. When an indeterminate (category II) or abnormal (category III) FHR pattern is identified, initial assessment may include a cervical exam to rule out umbilical cord prolapse, rapid cervical dilation, or rapid descent of the fetal head; a review of uterine activity to rule out tachysystole; and an evaluation of maternal vital signs, in particular temperature and blood pressure, to rule out maternal fever or maternal hypotension (ACOG, 2010b). These assessment data can guide appropriate treatment to attempt to resolve the pattern. Intrauterine resuscitation refers to a series of interventions to promote fetal well-being that include a change in maternal position, a decrease in uterine activity or uterine contraction frequency, administration of IV fluids, and administration of oxygen, and sometimes administration of terbutaline sulfate or amnioin-fusion (ACOG, 2010b; Garite & Simpson, 2011; Simpson, 2009b). Other resuscitative techniques include correction of maternal hypotension and modification of second-stage labor maternal pushing efforts (Garite & Simpson, 2011; Simpson, 2009b). The type of resuscitative technique is based on the specific characteristics of the observed FHR pattern and maternal condition. In some cases, a combination of techniques will be required. A summary of the goals and techniques for intrauterine resuscitation are presented in Table 15-6. These interventions are directed at improving maternal blood flow to the placenta and oxygen delivery to the fetus. Data suggest that these techniques can improve fetal oxygen status, but there is no evidence that these techniques will reverse asphyxia. If the clinical characteristics of the FHR patterns are thought to represent a serious risk for acidemia, these measures should be initiated only if doing so does not delay the move toward expeditious birth (Lyndon et al., 2009; Simpson, 2007, 2009b).
Table 15-6. INTRAUTERINE RESUSCITATION
Goal
Techniques/Methods
Promote fetal oxygenation
Lateral positioning (either left or right)
Oxygen administration at 10 L/min via nonrebreather face mask
IV fluid bolus of at least 500 mL of lactated Ringer’s solution
Discontinuation of oxytocin/removal of Cervidil/withholding next dose of Cytotec
Stopping pushing temporarily or pushing with every other, or every third, contraction (during second-stage labor)
Reduce uterine activity
Discontinuation of oxytocin/removal of Cervidil/withhold next dose of Cytotec
IV fluid bolus of at least 500 mL of lactated Ringer’s solution
Lateral positioning (either left or right)
If no response, consider terbutaline 0.25 mg subcutaneously
Alleviate umbilical cord compression
Repositioning
Amnioinfusion (during first-stage labor)
Stopping pushing temporarily or pushing with every other, or every third, contraction (during second-stage labor)
Correct maternal hypotension
Lateral positioning (either left or right)
IV fluid bolus of at least 500 mL of lactated Ringer’s solution
If no response, consider ephedrine 5-10 mg IV push
IV, intravenous.
POSITION CHANGE
Changing maternal position alters the relationship between the umbilical cord and fetal parts or the uterine wall and alters maternal cardiac output. It is usually done to minimize or correct cord compression and to improve uterine blood flow (increased uterine blood flow may also decrease the frequency of uterine contractions) (Simpson, 2009b). Position change can resolve or decrease the severity of prolonged decelerations and/or variable decelerations. Position change may also modify late decelerations if the etiology of this pattern is decreased uterine blood flow (usually secondary to supine positioning and inferior vena caval compression), as venous return and cardiac output are increased in the lateral position (Clark et al., 1991).
Only gold members can continue reading. Log In or Register to continue