Have patient in lithotomy position, draped for minimal exposure.
Female Genitalia
Examination

Technique
Findings
External Genitalia
Wash or sanitize hands and wear gloves on both hands
Ask patient to separate or drop open her knees. Tell patient you are beginning the examination, then touch lower thigh and—without breaking contact—move hand along thigh to external genitalia.
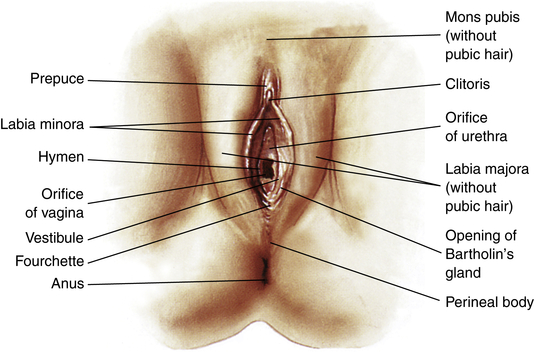
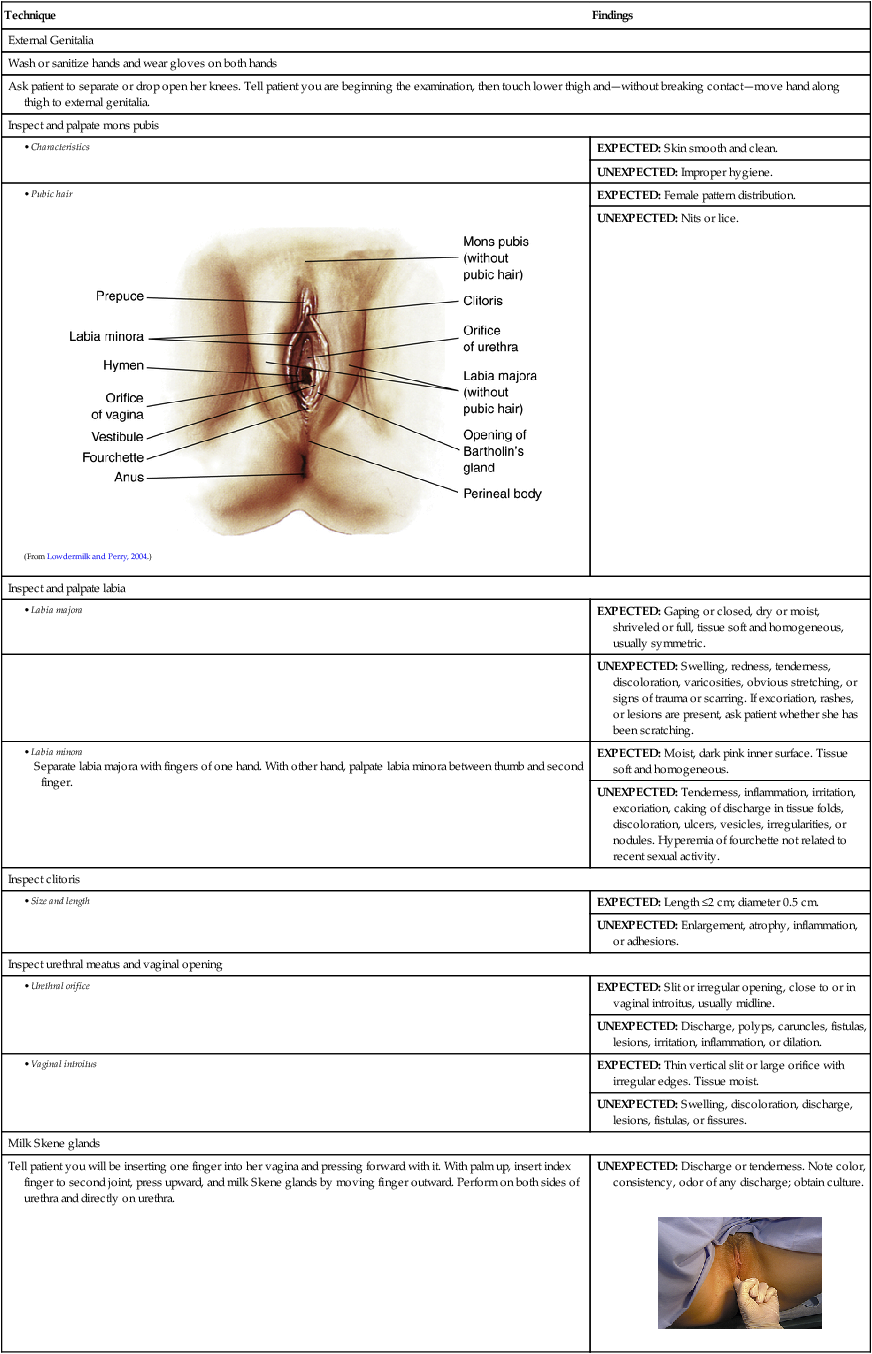
Inspect and palpate mons pubis
EXPECTED: Skin smooth and clean.
UNEXPECTED: Improper hygiene.
EXPECTED: Female pattern distribution.
UNEXPECTED: Nits or lice.
Inspect and palpate labia
EXPECTED: Gaping or closed, dry or moist, shriveled or full, tissue soft and homogeneous, usually symmetric.
UNEXPECTED: Swelling, redness, tenderness, discoloration, varicosities, obvious stretching, or signs of trauma or scarring. If excoriation, rashes, or lesions are present, ask patient whether she has been scratching.
EXPECTED: Moist, dark pink inner surface. Tissue soft and homogeneous.
UNEXPECTED: Tenderness, inflammation, irritation, excoriation, caking of discharge in tissue folds, discoloration, ulcers, vesicles, irregularities, or nodules. Hyperemia of fourchette not related to recent sexual activity.
Inspect clitoris
EXPECTED: Length ≤2 cm; diameter 0.5 cm.
UNEXPECTED: Enlargement, atrophy, inflammation, or adhesions.
Inspect urethral meatus and vaginal opening
EXPECTED: Slit or irregular opening, close to or in vaginal introitus, usually midline.
UNEXPECTED: Discharge, polyps, caruncles, fistulas, lesions, irritation, inflammation, or dilation.
EXPECTED: Thin vertical slit or large orifice with irregular edges. Tissue moist.
UNEXPECTED: Swelling, discoloration, discharge, lesions, fistulas, or fissures.
Milk Skene glands
Tell patient you will be inserting one finger into her vagina and pressing forward with it. With palm up, insert index finger to second joint, press upward, and milk Skene glands by moving finger outward. Perform on both sides of urethra and directly on urethra.
UNEXPECTED: Discharge or tenderness. Note color, consistency, odor of any discharge; obtain culture.

Palpate Bartholin glands
Tell patient she will feel you pressing around the entrance to her vagina. Palpate lateral tissue between index finger and thumb, then palpate entire area bilaterally, particularly posterolateral portion of labia majora.
EXPECTED: No swelling.
UNEXPECTED: Swelling, tenderness, masses, heat, fluctuation, or discharge. Note color, consistency, odor of any discharge; obtain culture.
Test vaginal muscle tone if indicated
Ask patient to squeeze vaginal opening around your finger.
EXPECTED: Fairly tight squeezing by some nulliparous women, less so by some multiparous women.
UNEXPECTED: Protrusion of cervix or uterus.
Locate the cervix
With your finger still in place, reach in farther to locate the cervix and note the direction in which it points. This may help you locate the cervix when you insert the speculum.
EXPECTED: Midline, may point horizontally, anteriorly, or posteriorly.
UNEXPECTED: Deviates to right or left.
Inspect for bulging and urinary incontinence if indicated
Ask patient to bear down.
EXPECTED: No bulging.
UNEXPECTED: Bulging of anterior or posterior wall, or urinary incontinence.
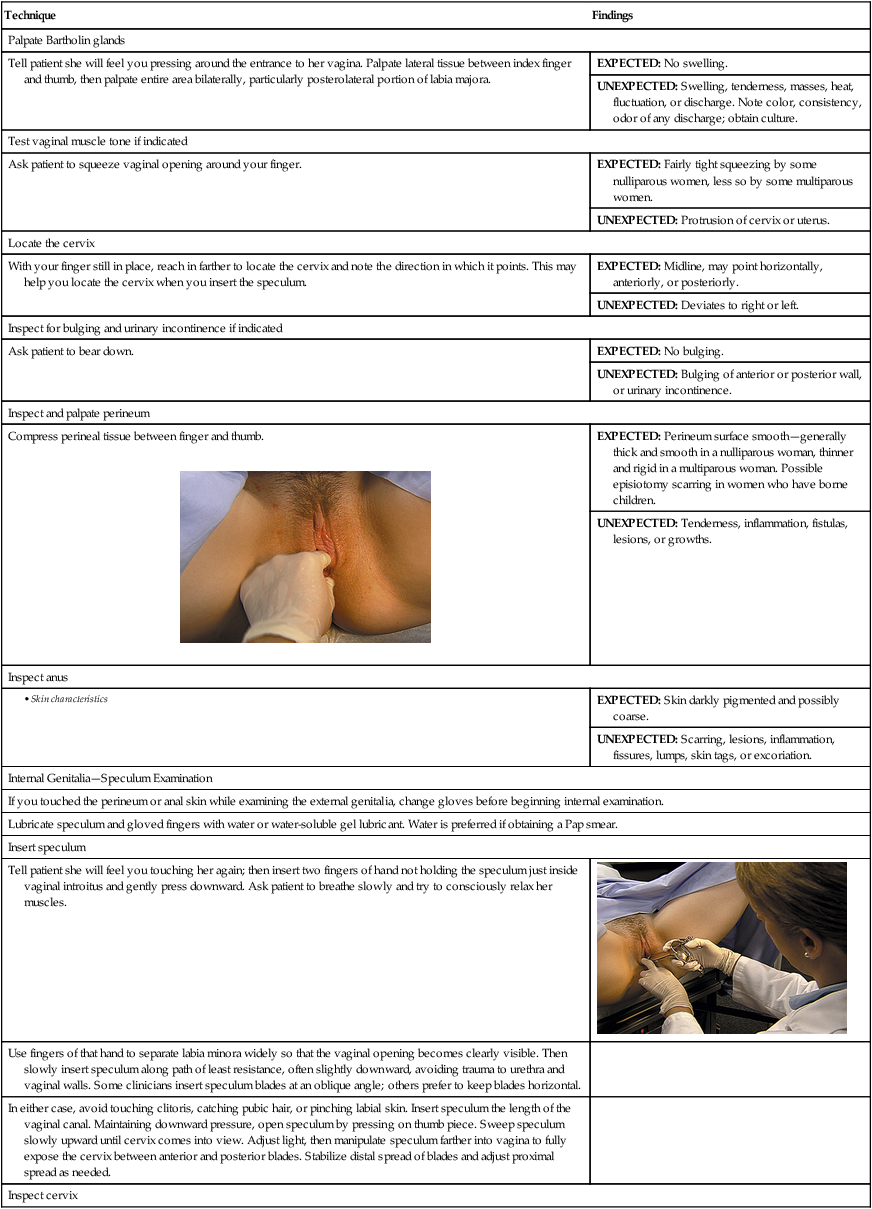
Inspect and palpate perineum
Compress perineal tissue between finger and thumb.

EXPECTED: Perineum surface smooth—generally thick and smooth in a nulliparous woman, thinner and rigid in a multiparous woman. Possible episiotomy scarring in women who have borne children.
UNEXPECTED: Tenderness, inflammation, fistulas, lesions, or growths.
Inspect anus
EXPECTED: Skin darkly pigmented and possibly coarse.
UNEXPECTED: Scarring, lesions, inflammation, fissures, lumps, skin tags, or excoriation.
Internal Genitalia—Speculum Examination
If you touched the perineum or anal skin while examining the external genitalia, change gloves before beginning internal examination.
Lubricate speculum and gloved fingers with water or water-soluble gel lubricant. Water is preferred if obtaining a Pap smear.
Insert speculum
Tell patient she will feel you touching her again; then insert two fingers of hand not holding the speculum just inside vaginal introitus and gently press downward. Ask patient to breathe slowly and try to consciously relax her muscles.

Use fingers of that hand to separate labia minora widely so that the vaginal opening becomes clearly visible. Then slowly insert speculum along path of least resistance, often slightly downward, avoiding trauma to urethra and vaginal walls. Some clinicians insert speculum blades at an oblique angle; others prefer to keep blades horizontal.
In either case, avoid touching clitoris, catching pubic hair, or pinching labial skin. Insert speculum the length of the vaginal canal. Maintaining downward pressure, open speculum by pressing on thumb piece. Sweep speculum slowly upward until cervix comes into view. Adjust light, then manipulate speculum farther into vagina to fully expose the cervix between anterior and posterior blades. Stabilize distal spread of blades and adjust proximal spread as needed.
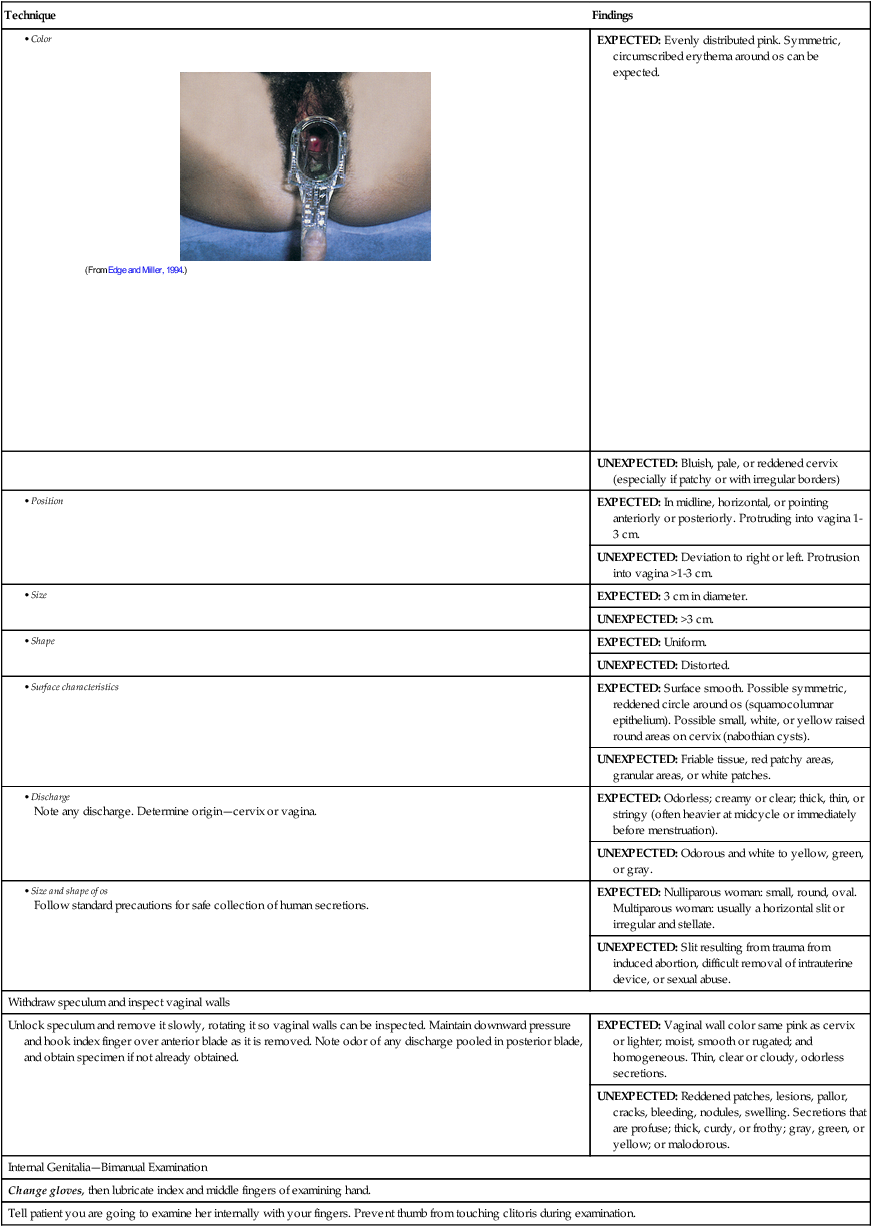
Inspect cervix
EXPECTED: Evenly distributed pink. Symmetric, circumscribed erythema around os can be expected.
UNEXPECTED: Bluish, pale, or reddened cervix (especially if patchy or with irregular borders)
EXPECTED: In midline, horizontal, or pointing anteriorly or posteriorly. Protruding into vagina 1-3 cm.
UNEXPECTED: Deviation to right or left. Protrusion into vagina >1-3 cm.
EXPECTED: 3 cm in diameter.
UNEXPECTED: >3 cm.
EXPECTED: Uniform.
UNEXPECTED: Distorted.
EXPECTED: Surface smooth. Possible symmetric, reddened circle around os (squamocolumnar epithelium). Possible small, white, or yellow raised round areas on cervix (nabothian cysts).
UNEXPECTED: Friable tissue, red patchy areas, granular areas, or white patches.
EXPECTED: Odorless; creamy or clear; thick, thin, or stringy (often heavier at midcycle or immediately before menstruation).
UNEXPECTED: Odorous and white to yellow, green, or gray.
EXPECTED: Nulliparous woman: small, round, oval. Multiparous woman: usually a horizontal slit or irregular and stellate.
UNEXPECTED: Slit resulting from trauma from induced abortion, difficult removal of intrauterine device, or sexual abuse.
Withdraw speculum and inspect vaginal walls
Unlock speculum and remove it slowly, rotating it so vaginal walls can be inspected. Maintain downward pressure and hook index finger over anterior blade as it is removed. Note odor of any discharge pooled in posterior blade, and obtain specimen if not already obtained.
EXPECTED: Vaginal wall color same pink as cervix or lighter; moist, smooth or rugated; and homogeneous. Thin, clear or cloudy, odorless secretions.
UNEXPECTED: Reddened patches, lesions, pallor, cracks, bleeding, nodules, swelling. Secretions that are profuse; thick, curdy, or frothy; gray, green, or yellow; or malodorous.
Internal Genitalia—Bimanual Examination
Change gloves, then lubricate index and middle fingers of examining hand.
Tell patient you are going to examine her internally with your fingers. Prevent thumb from touching clitoris during examination.
Female Genitalia




Get Clinical Tree app for offline access
