Chapter 40 Feeding 2
Enteral feeding
INTRODUCTION
LEARNING OUTCOMES
By the end of this section you should be able to:
FACTORS TO NOTE
See also Factors to note in Feeding 1 (Ch. 39).
Hambridge et al (1995) give reasons why some children are unable to feed orally:
These children can be fed enterally via nasogastric (NG) tube or gastrostomy.
The multidisciplinary team is essential when a sick child has special dietary requirements:
Nasogastric tubes
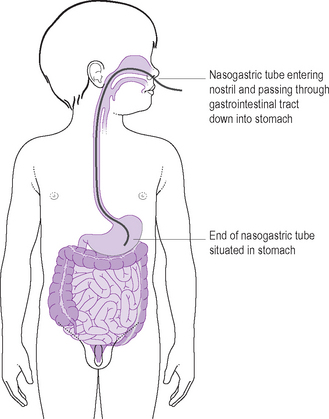
There are two main types of NG tube commonly used. (1) Short-term tubes, which can be used for up to 7 days and (2) long-term tubes, which can last up to 30 days (refer to manufacturer’s guidelines). The tubes are sized according to the width of their internal lumen; 6, 8 and very occasionally 10 French gauge (Fg) are most commonly used in children. If a thickening agent has been added to the child’s feed, the small 6 Fg diameter tube may be too narrow to facilitate instillation of the feed. Tubes can come in various lengths which range from 50–85 cm in both short term and long term tubes. The length used will depend on how big the child is. The tube must be long enough to cover the length from the outer edge of the child’s face, through the nasopharynx and down into the stomach (Fig. 40.1). Short-term tubes should be changed every 5–7 days and long-term tubes monthly, to prevent increased risk of bacterial contamination and the material of the tube being eroded by gastric secretions (Taylor & Goodison-McLaren 1992, Skipper et al 2003).
Gastrostomy tubes are made of silicone. There are three main types: skin-level ‘button’, percutaneous endoscopic tubes and surgically placed tubes. The skin around a gastrostomy site should be washed daily to prevent the skin around the site becoming sore (Coldicutt 1994). Frequency and timing of tube changes vary according to the device used and the child’s condition.
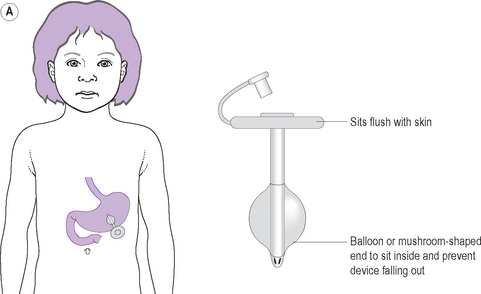
The gastrostomy button is a device in which the exterior of the tube sits flush with the skin and, when not in use, resembles a button on the surface of the skin (Fig. 40.2). It is usually changed once every 3–6 months. However, in some areas, when the gastrostomy tract has been formed via a Stamm procedure (full surgical procedure), tubes are placed directly.
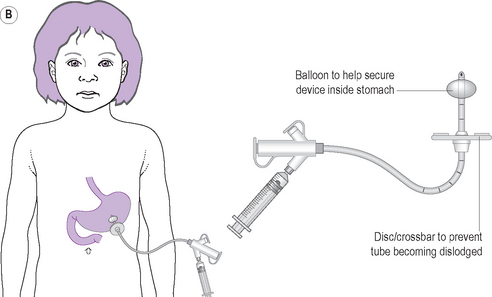
The percutaneous endoscopic tube (PEG) is a gastrostomy tube that is inserted through the skin into the stomach under endoscopic control, therefore avoiding the need for a full, laparoscopic surgical procedure (Booth 1991). It can stay in situ usually for up to 2 years.
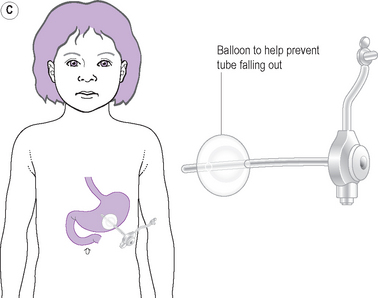
A surgically placed tube is usually much shorter term in use and should only be changed by a surgeon or nurse who has received training in the procedure. If it becomes displaced in the first 2 weeks postoperatively, before the tract has properly formed, it must be re-inserted as a matter of urgency or the skin and tissues will close over. Gastrostomy tubes are most commonly sized between 9 and 15 Fg, although smaller or larger tubes may be used in small babies or older children (Bowling 2003).
Research-based practice relating to the risks of enteral feeding
Research has highlighted the risks of nasogastric feeding, in particular the risk of aspiration of feed because of misplaced tubes, blocked tubes, infection transmission and the excessive vacuum pressure caused by using smaller-volume syringes (Taylor & Goodison-McLaren 1992, Lord 1997, Anderton & Nivgough 1991, Skipper et al 2003).
Maintaining patency of nasogastric and gastrostomy tubes
NG and gastrostomy tubes must be flushed before and after a feed. During continuous feeding, or when not in use, NG tubes should be flushed regularly to maintain patency, e.g. every 4 h during the daytime (Lifshitz et al 1991, Paul et al 1993).
Preventing infection transmission via enteral feeding
Whenever an NG or gastrostomy tube is flushed, it should be done with cooled, boiled water, or Tap, depending on the age and condition of the child (Coldicutt 1994, Anderton 1995, Paul et al 1994, Skipper et al 2003). In addition, feeds should be prepared only on surfaces which have been cleaned thoroughly with soap and water, dried and then wiped with 70% isopropyl alcohol-impregnated wipes (Anderton & Nivgough 1991). Any feed delivery systems should be single-use only, and feed containers (the visible external part of NG and gastrostomy tubes) should also be cleaned with alcohol-impregnated wipes prior to use (Paul et al 1994, Anderton 1995, Skipper et al 2003).
Size of enteral syringe used when administering feed/flush via nasogastric tube
A long-term tube is softer and more prone to damage. The smaller the syringe, the smaller is the bore (the hole in the middle) and the greater the pressure created when injecting with it; 1–5 mL syringes produce the highest pressure for a given force. Using a larger-sized syringe – 50 or 100 mL – reduces the pressure on the tube, thus minimising the risk of damage (Taylor & Goodison-McLaren 1992, Paul et al 1993, Sidey 1995).
GUIDELINES
Parents and older children should be encouraged to be involved with enteral feeding. This can include being involved in or even being trained to pass the NG or gastrostomy tube if they so wish. Involvement can help them to feel in control of the procedure and help their acceptance of the problem (Holden et al 1997).
PASSING A NASOGASTRIC (NG) TUBE
EQUIPMENT
METHOD
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


