Facilitation of skills related to childbearing
Membrane sweep
Learning outcomes
Having read this chapter, the reader should be able to:
NICE (2008) recommend that while the majority of women will go into spontaneous labour by 42 weeks, the midwife should discuss the risks associated with prolonged pregnancy (>42 weeks) with women at the 38-week antenatal appointment. This discussion should include membrane sweeping, also referred to as a ‘stretch and sweep’. This chapter considers the skill of sweeping or ‘stripping’ the membranes.
Membrane sweeping
Yildirim et al (2010) define membrane sweeping as ‘the digital separation of the chorioamniotic membranes from the lower uterine segment’. It involves a vaginal examination (VE) (p. 224), so the midwife can use her fingers to gently dilate (stretch) the cervical os, and then separate the membranes from the lower segment (sweep). This is performed on a cervix that is beginning to dilate, as it requires entry of the fingers through the cervix. If the cervix is not dilated, cervical massage can be undertaken (NICE 2008). This causes an increase in the local production of prostaglandin and increases prostaglandin metabolites within the maternal circulation (Boulvain et al 2005, Yildirim et al 2010) with labour following over the next few days.
de Miranda et al (2006) undertook membrane sweeping every 48 hours, performing three 360° sweeps on each occasion until labour commenced or the pregnancy reached 42 weeks’ gestation. Yildirim et al (2010) used the same technique but only performed it once. NICE (2008) do not specify how to undertake a membrane sweep but recommend nulliparous women be offered the procedure at the 40- and 41-week antenatal visits, while parous women should be offered it at the 41-week visit. Additionally they suggest membrane sweeping should be offered whenever a VE is undertaken to assess the cervix or additional membrane sweeping offered if labour does not commence spontaneously. The frequency at which membrane sweeping should be undertaken is still subject to debate.
Cervical massage can be achieved on a closed cervix by using the fore- and middle fingers to make circular pushing and massaging movements on the surface of the cervix for 15–30 seconds’ duration (de Miranda et al 2006, Yildirim et al 2010). Gibbon (2012) recommends massaging the cervix around the vaginal fornices.
Benefits and risks
Membrane sweeping does appear to reduce the time to spontaneous onset of labour and the need for formal methods of induction, e.g. prostaglandin (PGE2) (de Miranda et al 2006, Mozurkewich et al 2011, NICE 2008). Yildirim et al (2010) found an increase in spontaneous labour within 7 days. de Miranda et al (2006) concluded membrane sweeping significantly reduced the time to delivery by 1 day when undertaken at 41 weeks’ gestation. Their study reduced the number of women with post-term pregnancies from 41 to 23% and found the effects were more evident for cervical sweeping than massage with significant effects for both primi- and multigravid women. However, Hamdan et al (2009) in their study looking at serial membrane sweeping at 36+6–40+6 weeks for women planning a vaginal birth after caesarean delivery found no significant effect on the spontaneous onset of labour. Hill et al (2008) undertook weekly sweeps from 38 weeks and found no difference in the number of post-term pregnancies or inductions of labour.
There are no differences in adverse maternal and neonatal outcomes for women who had membrane sweeping or massage compared with those who did not, e.g. prelabour rupture of membranes, maternal and neonatal infection requiring antibiotic treatment, meconium-stained liquor, vaginal bleeding, instrumental and operative delivery, neonatal morbidity (Boulvain et al 2005, de Miranda et al 2006, Hamdan et al 2009, Yildirim et al 2010).
Membrane sweeping is associated with increased maternal discomfort and vaginal bleeding with and following the procedure (Boulvain et al 2005, de Miranda et al 2006, Mozurkewich et al 2011) and it is important the woman is aware of this before she consents to the procedure. Yildirim et al (2010) found that 19.5% of women found membrane sweeping resulted in discomfort.
Sweeping the membranes appears to be a safe procedure which may reduce the incidence of prolonged pregnancy. Provided there are no complications, e.g. placenta praevia, contraindication to labour or vaginal birth, it can be offered to women over 40 weeks’ gestation. Local protocols should be followed but generally this procedure can be undertaken in an outpatient setting such as the woman’s home or antenatal clinic. Asepsis should be maintained and the midwife should be trained in this aspect of care prior to undertaking the procedure.
The midwife should maintain contemporaneous records and should document the discussion with the woman, that consent is obtained, when and how the procedure was undertaken, and the findings from the VE.
PROCEDURE: stretch and sweep of the membranes
• Discuss the procedure including the benefits and risks with the woman and gain informed consent.
• Prepare for and undertake the examination per vaginam (as detailed on p. 225 as far as ‘Locate the cervix …’) expecting to find a posterior, largely uneffaced, almost closed cervix.
• Undertake a Bishop’s scoring (or similar) assessment (see Glossary) of the cervix.
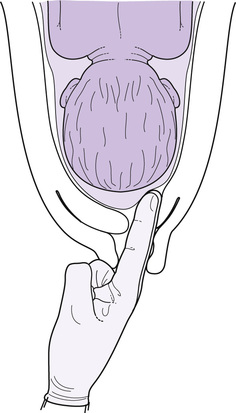
• Using some inward pressure, move the finger(s) with a sweeping circular action through 360° (Fig. 29.1). This should be undertaken fairly decisively as the woman will be uncomfortable, which will increase if the procedure is unnecessarily prolonged.