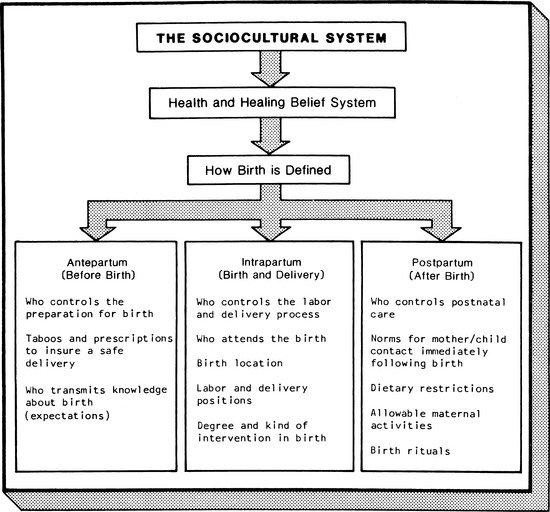
CHAPTER 4 1 State the need for a cultural assessment of the childbearing family. 2 Describe data to be collected through a cultural assessment. 3 Perform a cultural assessment of a childbearing family. 4 Analyze data obtained from a cultural assessment for potential problem areas. 5 Formulate nursing interventions to address problem areas identified from the assessment. 6 Identify barriers to care that are frequently encountered by the culturally diverse client. 7 Identify ways to decrease barriers to care encountered by the culturally diverse client. A Transcultural nursing is concerned with the provision of nursing care in a manner that is sensitive to the needs of individuals, families, and groups. 1. A major aim of transcultural nursing is to understand and assist members of diverse cultural groups with their nursing and health care needs. 2. Nursing interventions that are culturally relevant to the needs of the client decrease the possibility of conflict or misunderstanding arising from people from different backgrounds (Andrews, 1995). 3. The goal of transcultural nursing is “to develop a scientific and humanistic body of knowledge to provide culture-specific and culture-universal nursing care practices” (Andrews, 2003). a. Culture-specific refers to particular values, beliefs, and patterns of behavior that tend to be special or unique to a group and that do not tend to be shared with members of other cultures. b. Culture-universal refers to the commonly shared values, norms of behavior, and life patterns that are similarly held among cultures about human behavior and lifestyles (Leininger & McFarland, 2002). 4. Applying transcultural concepts to nursing practice includes: b. Understanding the cultural context of the client and family c. Using culturally sensitive strategies to meet mutually satisfying goals 5. A common problem faced by nurses who want to use cultural data is knowing what data to collect and how to use the data effectively. a. A major purpose of collecting cultural data is to give the nurse greater insight into and understanding of: (1) The nature and behavior of clients (2) The problems that clients encounter in health promotion and maintenance b. These data should be relevant to potential or actual nursing problems. c. Transcultural knowledge is used to augment, clarify, explain, or assist in attaining client-centered goals. B The overall goal is to develop and sustain cultural (and linguistic) competence among health care professionals. 1. The concept refers to a complex integration of knowledge, attitudes, and skills that enhance cross-cultural communication and appropriate/effective interactions with others (American Academy of Nursing, 1992, 1993; Campinha-Bacote, 2000, 2003; Geron, 2002). 2. Cultural competence has been defined as a process, as opposed to an end point, in which the nurse continually strives to work effectively within the cultural context of individuals, families, or communities from diverse cultural backgrounds (Andrews & Boyle, 1997; Campinha-Bacote, 2000, 2003; Purnell & Paulanka, 2008; Wells, 2000). 3. Cultural and linguistic competence have been defined and issued as standards from the Office of Minority Health at the U.S. Department of Health & Human Services (1999) as the ability of health care providers and organizations to understand and effectively respond to the cultural and linguistic needs brought by the clients to the health care encounter. C Childbearing is a time of transition and social celebration of great importance in any society (Lauderdale, 2008). 1. Many cultures have particular customs and beliefs that dictate activities and behavior during this time. a. Some might be considered prescriptive in nature: phrased positively, and describing expectations of behavior. (1) Might involve wearing special articles of clothing (3) Might be recommendations for physical activity and/or diet b. Others are restrictive: phrased negatively, and limiting choices or behaviors; usually directed toward: c. A third area of beliefs is the taboo—restrictions with serious supernatural consequences. 2. The labor and delivery and postpartum periods might also be governed by unique customs. D The different ways in which a particular society views this transitional period and manages childbirth depend on the culture’s beliefs about health, medical care, reproduction, and the role and status of women (Figure 4-1). 1. Pregnancy and childbirth practices in Western society have changed dramatically during the past two decades. A few of the trends that require nurses to examine and rethink how we can better care for our clients include: a. An increase in the number of women in the workforce b. Advances in reproductive technology e. Increase in health information available to consumers on the Internet f. The large influx of refugees and immigrants (Tiedje, 2000) 2. Subcultures within the United States and Canada have very different practices, values, and beliefs about childbirth and the roles of men, women, social support networks, and health care practitioners. 3. Additionally, religious background, regional variations, age, urban or rural background, sexual preferences, and other individual characteristics all contribute to cultural differences surrounding the childbearing period. 4. Great variations exist in the social class, ethnic origin, family structure, and social support networks of women and their families. One must keep in mind the individual differences that are present within cultures as well as those found between cultures. 5. Culturally competent care for ethnic minority women requires a delicate balance in assumptions that drive the assessment process and the resultant care. a. One must balance the assumption that those women who immigrated from a similar region share similar values and beliefs that influence how they will respond to the childbirth experience with the assumption of diversity among women from the same area (Meleis, 2003). b. Women’s experiences that profoundly influence their childbirth experience include all of the individual characteristics described previously; therefore, the descriptions of the various “populations” in this chapter must be viewed within the context of diversity within each group. 1. Cultural assessment is defined as assessment of: 2. It is performed to identify patterns that might assist or interfere with a nursing intervention or planned treatment regimen. 3. To understand why birth is managed in a particular way, it is necessary to view the process in terms of the society’s: b. Political and economic system d. In addition, Kay (1982) delineated specific cultural data for the four periods during childbearing: antepartum, intrapartum, postpartum, and newborn. In this chapter assessment needs during each of these four periods are discussed. (For specific details about particular cultural groups, see the material referenced in appropriate chapters and sections; see also the appendix at the end of this chapter.) a. Determinants of the society’s acceptance of the pregnancy b. Consideration of pregnancy as a state of illness or of health. Many cultural groups perceive pregnancy as a normal physiologic process or state, and don’t believe that pregnant women are ill or in need of “curative services.” These women often delay or do not receive any prenatal care from a health care provider (Lauderdale, 2008). (1) Latinos in particular consider pregnancy a natural condition that usually doesn’t require medical care, unless there is a problem, until late in the pregnancy. However, the mother and fetus are vulnerable to outside influences and will take protective measures (Mattson, 2003). (2) In one study, Amish women used perinatal care based on their beliefs about pregnancy and childbirth, and in relation to cost, transportation, and child care. The women initiated prenatal care earlier for first pregnancies, and later with subsequent ones, knowing that pregnancy was a “nonproblematic” condition. They did seek immediate attention if a serious problem arose (bleeding, for example) (Campanella, Korbin, & Acheson, 1993). (1) Dietary prescriptions or restrictions (a) Adherence to the hot or cold theory of health and diet (especially with Hispanic and Asian clients). This theory describes the intrinsic properties of foods, beverages, medicines, and their effects on the body. [i] Health is maintained through a balance of these forces. [ii] If an imbalance occurs, illness results. [iii] To produce balance (and restore or maintain health), illness and conditions such as pregnancy are treated with substances having the opposite property of the illness (i.e., pregnancy is considered to be a hot state; thus any treatments must be of a cold nature). • Temperature and spiciness do not determine classification; however, this varies among cultural groups. • Generally, warm or hot foods are believed to be easier to digest than cold or cool foods. [iv] These properties of hot and cold are also part of the yin-yang belief system prevalent among Asian approaches to health and diet (Andrews, 2008b). (b) Another somewhat unfamiliar practice is that of pica, or the ingestion of nonfood substances, especially clay or starch [i] Pica is often practiced by African-American women, usually in the rural southern United States. [ii] There are many explanations for why this occurs. [iii] Some Hispanic women prefer the solid milk of magnesia, whereas others eat the ice or frost that forms inside refrigerator/freezer units (Boyle & Mackey, 1999). (2) Activity restrictions or prescriptions, including the use of massage as a treatment for the various ills experienced during pregnancy; many people believe that the activities of the mother influence the outcome of pregnancy and the well-being of the newborn. (3) Expression of emotions, including anger, fear, and anxiety (a) Pueblo and Navajo Indians, Mexicans, and Japanese believe the mother should remain happy to bring the baby joy and good fortune (Waxler-Morrison, Andrews, & Richardson, 1990). (b) Hispanics believe experiencing susto in pregnancy is bad for the mother and baby (Mattson, 2003). (c) One major consideration at this time is intimate partner violence (IPV) that may escalate or begin during pregnancy. IPV of pregnant women has been associated with adverse pregnancy outcomes for mother and infant (Taggart & Mattson, 1996). (See Chapter 18 for further discussion.) (4) People from whom to seek advice, and the appropriate time to do so (a) Women from many cultures might refuse to seek early prenatal care because they consider pregnancy a normal and healthy state. (b) Fear, modesty, and a wish to avoid a physical examination by a male care provider might also prevent some women from seeking care from Western providers (Andrews, 2008b). a. Appropriate setting for labor and delivery to occur (1) There are often cultural differences between laboring women and nurses in a highly biotechnologic Western birthing unit related to the application of technology and pain management (Carlton, Callister, & Stoneman, 2005) b. Appropriate attendants for support and as a “practitioner” (1) Most non-Western cultures see childbearing as being within the woman’s domain. (2) Support during labor and assistance after delivery are usually provided by women relatives or friends. (a) It is unusual, and should not be expected, for a father from a non-Western culture to provide this support and caretaking. (b) Male caregivers may be refused, or may cause distress (Asian, Arab, many Hispanic groups). Practices followed by women of Islamic, Chinese, and Asian Indian backgrounds might include strict religious and cultural prohibitions against viewing the woman’s body by either the husband or any other man (Lauderdale, 2008). (c) For an Orthodox Jewish woman in labor, and for reasons of modesty, the support person of choice may be a woman of her community (Lewis, 2003) c. Pain control, including what expressions of discomfort are permitted and expected d. Restrictions and prescriptions for activity, including ambulation and massage e. Dietary recommendations, including the continuation of intake of food and drink; possible preference for herbal teas (Hispanic and Asian women especially). (1) Behaviors that are necessary to ensure the appropriate length, including diet and activity; Hispanics in particular like to walk around rather than remain lying in bed, and also believe that drinking manzanilla tea makes the contractions stronger. (2) Expected interventions if the time is prolonged. Despite the growing number of Cesarean births occurring across the world, there is little in the literature documenting the beliefs of women about this growing surgery. (a) However, it is known that there are many cultures in which women are reluctant or fearful of having a cesarean birth (Callister, 2008; Zlot, Jackson & Korenbrot, 2005). (b) Who makes the decision as to whether the recommendation for a cesarean birth will be accepted is also culturally based; it might be the husband, a religious leader, or community or family elders. g. Expected and ideal positions for facilitating pushing and delivery h. Appropriate disposition of placenta and umbilical cord after delivery (1) Some cultural groups believe that burying the placenta, the umbilical cord, or both in a particular place will bring good fortune to the child and family. (2) Others wish to preserve the cord through drying to use it medicinally at a later time.
Ethnocultural Considerations in the Childbearing Period
INTRODUCTION
CLINICAL PRACTICE
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree