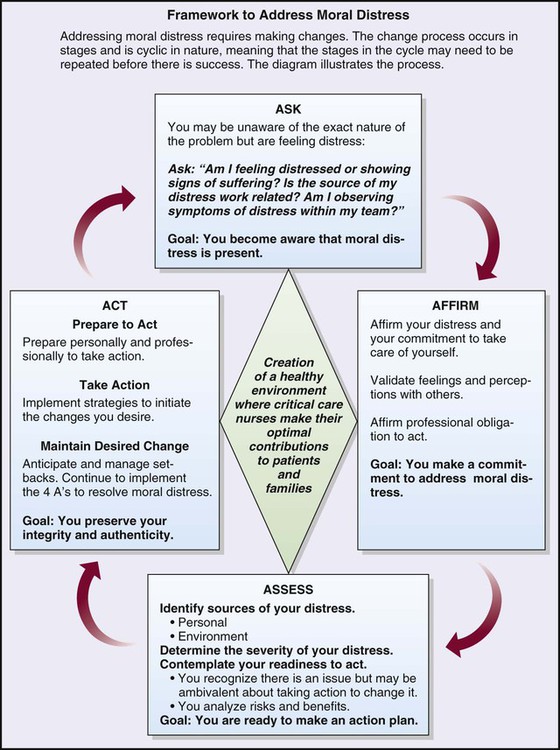
Morals are the “shoulds,” “should nots,” “oughts,” and “ought nots” of actions and behaviors, and they are related closely to cultural and religious values and beliefs that govern our social interactions. Morals form the basis for action and provide a framework for the evaluation of behavior.1 Ethics are concerned with the basis of the action rather than whether the action is right or wrong, good or bad. Imposition of ethics implies that an evaluation is being made that is based on or derived from a set of standards. It refers to what rules are required to prevent harm to persons and to the collective beliefs and values of a community or profession.1 Recently, moral distress has been a topic widely discussed in the literature as a serious problem for nurses.2–5 Nurses face multiple challenges on a daily basis: emergency situations, tension from conflict with others, complex clinical cases, new technologies, increasing regulatory requirements, acquisition of new skills/knowledge, staffing issues, financial constraints, workplace violence, to name a few. This care environment has led to increasingly complex moral and ethical dilemmas.5 In addition, they frequently may experience emotional outbursts from patients, families, co-workers, and feel a lack of control and “burnt out.”2,5 Moral distress occurs when a person knows the ethically appropriate action to take but cannot act on it. It also manifests when a nurse acts in a manner contrary to personal and professional values. As a result, there can be significant emotional and physical stress that leads to feelings of loss of personal integrity and dissatisfaction with the work environment. Relationships with co-workers and patients are affected, and the quality of care can be negatively affected. There is also a great impact on personal relationships and family life; nurses experiencing moral distress may resign their position or leave the profession entirely.3 It is therefore important that nurses recognize moral distress and actively seek strategies to address the issue through institutional, personal, and professional organizational resources. Knowledge and application of ethical principles and guidelines can assist the nurse in daily practice when ethical dilemmas occur. Box 2-1 provides a position statement on moral distress, promulgated by the American Association of Critical-Care Nurses (AACN).6 The document is evidence-based, providing additional references for the reader. There is also a reference to ensuring that support to alleviate moral distress is present in a healthy work environment (see Chapter 1). Actions are listed for direct care staff nurses as well as employers. The AACN has created a framework—The 4A’s to Rise Above Moral Distress—to support nurses who are experiencing moral distress (Figure 2-1). ASK, the first stage, is a self-awareness and reflection period in which one becomes more aware of the distress and its effects on oneself. Specific areas to address are physical, spiritual, emotional, and behavioral responses. During stage two, AFFIRM, one affirms the distress and makes a commitment to take care of oneself. In stage three, ASSESS, one needs to identify the timing and context of when the stressors occur; determine the severity of the distress; and examine one’s readiness to act. The final stage, ACT, consists of preparation, the action itself, and maintaining the desired change. Although the model was created by AACN, it is a framework that can be used in diverse settings and by various health care professionals.7 McCue8 reported using this model as a resource for resolving an issue between a chief nurse executive and chief executive officer. In this case, the impact of the outcome was at the organizational level. In order to avoid moral distress, nurses must feel free to advocate for themselves, their patients, co-workers, and a safe and effective work environment. Lachman and colleagues describes moral courage as “the willingness to stand up for and act according to one’s ethical beliefs when moral principles are threatened, regardless of the perceived or actual risks (such as stress, anxiety, isolation from colleagues, or threats to employment)”.9,p24 They describe organizational cultures that support moral courage, the importance of peer support, education, and policies that can support moral courage of staff. Other authors have reported that moral courage is needed in everyday practice and that one must act ethically even in the presence of risk.4,10 Certain ethical principles were derived from classic ethical theories that are used in health care decision making. Principles are general guidelines that govern conduct, provide a basis for reasoning, and direct actions. The six ethical principles that are discussed in this chapter are autonomy, beneficence, non-maleficence, veracity, fidelity, and justice (Box 2-2). The concept of autonomy appears in all ancient writings and early Greek philosophy. In health care, autonomy can be defined as an agreement to respect another’s right to self-determine a course of action and the support of independent decision making11 without coercion or interference from others. Autonomy is a freedom of choice or a self-determination that is a basic human right. It can be experienced in all human life events. The critical care nurse is often “caught in the middle” in ethical situations, and promoting autonomous decision making is one of those situations. As the nurse works closely with patients and families to promote autonomous decision making, another crucial element becomes clear. Patients and families must have all of the information about a particular situation before they can make a decision that is best for them. They should be given all the pertinent information and facts, and they must have a clear understanding of what was presented. This is where the nurse is a most important member of the health care team—as patient advocate, the nurse provides more information as needed, clarifies points, reinforces information, and provides support during the decision-making process. Box 2-3 presents the Nursing Interventions Classification (NIC) feature on nursing intervention activities that facilitate decision making. NIC Decision-Making Support Determine whether there are differences between the patient’s view of own condition and the view of health care providers Assist patient to clarify values and expectations which may assist in making critical life choices Inform patient of alternative views or solutions in a clear and supportive manner Help patient identify the advantages and disadvantages of each alternative Establish communication with patient early in admission Facilitate patient’s articulation of goals for care Obtain informed consent, when appropriate Facilitate collaborative decision making Be familiar with institution’s policies and procedures Respect patient’s right to receive or not to receive information Provide information requested by patient Help patient explain decision to others, as needed Serve as a liaison between patient and family Serve as a liaison between patient and other health care providers Use interactive computer software or web-based decision aides as an adjunct to professional support Refer to legal aid, as appropriate From Bulechek GM, et al: Nursing Interventions Classification (NIC). 6th ed. St. Louis: Mosby; 2013. The concept of doing good and preventing harm to patients is the sine qua non for the nursing profession. However, the ethical principle of beneficence—which requires a nurse to promote the well-being of patients—points to the importance of this duty for the health care professional. The principle of beneficence presupposes compassion; taking positive action to help others; desire to do good. It is the core principle of patient advocacy.11 Harms and benefits are balanced, leading to positive or beneficial outcomes. In approaching issues related to beneficence, conflict with another principle, that of autonomy, is common. Paternalism exists when the nurse or physician makes a decision for the patient without consulting the patient. Another ethical principle that is closely related to autonomy and veracity is fidelity. Fidelity, or faithfulness and promise-keeping to patients, is an essential aspect of nursing. The American Nurses Association (ANA) states that this principle requires loyalty, fairness, truthfulness, advocacy, and dedication to our patients. It involves an agreement to keep our promises. Fidelity refers to the concept of keeping a commitment and is based on the virtue of caring.11 It forms a bond between individuals and is the basis of all professional and personal relationships. Regardless of the amount of autonomy that patients have in critical care areas, they still depend on the nurse for many types of physical care and emotional support. A trusting relationship that establishes and maintains an open atmosphere is one that is positive for all involved. Privacy also has been described as being inherent in the principle of fidelity. It may be closely aligned with confidentiality of patient information and a patient’s right to privacy of his or her person, as in maintaining privacy for the patient by pulling the curtains around the bed or making sure that he or she is adequately covered. The ANA summary and principle on privacy and confidentiality are found in Box 2-4. Box 2-4 Ana Statement on Privacy and Confidentiality • A patient’s right to privacy with respect to individually identifiable health information, including genetic information, should be established statutorily. Individuals should retain the right to decide to whom, and under what circumstances, their individually identifiable health information will be disclosed. Confidentiality protections should extend not only to health records, but also to all other individually identifiable health information, including genetic information, clinical research records, and mental health therapy notes. • Use and disclosure of individually identifiable health information should be limited. • A patient should have the right to access his or her own health information and the right to supplement such information so that they are able to make informed health care decisions, to correct erroneous information, and to address discrepancies that they perceive. • Patients should receive written, easily understood notification of how their health records are used and when their individually identifiable health information is disclosed to third parties. • The use or disclosure of individually identifiable health information absent an individual’s informed consent should be prohibited. Exceptions should be permitted only if a person’s life is endangered, if there is a threat to the public, or if there is a compelling law enforcement need. In the case of such exceptions, information should be limited to the minimum amount necessary. • Appropriate safeguards should be developed and required for the use, disclosure and storage of personal health information. • Legislative or regulatory protections on individually identifiable health information should not unnecessarily impede public health efforts or clinical, medical, nursing, or quality of care research. • Strong and enforceable remedies for violations of privacy protections should be established, and health care professionals who report violations should be protected from retaliation. • Federal legislation should provide a floor for the protection of individual privacy and confidentiality rights, not a ceiling. Federal legislation should not preempt any other federal or state law or regulation that offers greater protection.
Ethical Issues
Differences between Morals and Ethics
Moral Distress
Moral Courage
Ethical Principles
Autonomy
 Box 2-3
Box 2-3
Beneficence
Fidelity
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree