Chapter 11 Episiotomy and tears
TYPES OF INCISION
Medial incision
Medial incisions are made in the anatomical plane and are comfortable. There is less bleeding, and they are easy to repair. However, access is limited and the incision carries the risk of extension into the rectum, hence it is only used by someone experienced (Figure 11.1a).
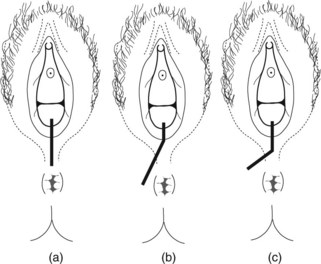
Mediolateral Incision
This incision is safe, easy to perform, and thus the most commonly used. It is associated with least risk of anal sphincter damage. The cut must begin at the mid-point of the fourchette and is directed towards the ischial tuberosity into the ischiorectal pad of fat (Figure 11.1b).
TECHNIQUE
• An existing epidural can provide adequate anaesthesia; if not infiltrate with a local anaesthetic. The fingers are placed inside the introitus to protect the presenting parts of the fetus (Figures 11.2 and 11.3).
• The index and middle fingers are placed in the introitus along the direction of intended cut. The thumb is apposed to stabilise the perineum. A single cut 3 cm long starting from the mid-point of the fourchette is made with scissors.
• In the J-shaped incision, the thumb, middle and index fingers are apposed in the midline of the fourchette. The tip of the thumb is placed 0.5–1 cm above the brown of the anus. A midline incision to the tip of the thumb is made. The thumb and fingers are kept firmly apposed. The scissors are then rotated to align transgentially to the brown perianal area and another incision is then made (Figure 11.4).

Figure 11.2 Using the fingers the fourchette is drawn away from the presenting part of the fetus before infiltration.


TIMING
Episiotomy should be performed:
• when tearing of the vagina becomes obvious. This is indicated by a show of fresh blood when the presenting part of the fetus distends the perineum as the mother pushes
DO
• Unless in an emergency, ensure there is adequate anaesthesia. Epidural anaesthesia may not be sufficient. Pudendal block anaesthetises only S2–S4 hence perineal infiltration with additional local anaesthetic is required to cover S5 of the perianal area (Figure 11.5).
• Remember the total amount of local anaesthetic used should not exceed 200 mg of lidocaine. This is especially important in women who have been given an epidural block.
• The pudendal nerve enters the pudendal canal approximately 1 cm below and 1 cm cephalad to the ischial spine when the woman is supine. The pudendal vessels are beside the nerves (Figure 11.6), therefore aspirate back before infiltration to prevent intravascular injection.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


