Question 1. What is a gastrostomy tube and name the different types of gastrostomy tubes?
A gastrostomy tube is a feeding tube that connects the stomach with the surface of the abdominal wall. It is usually placed in children who require medium to long-term nutrition support.
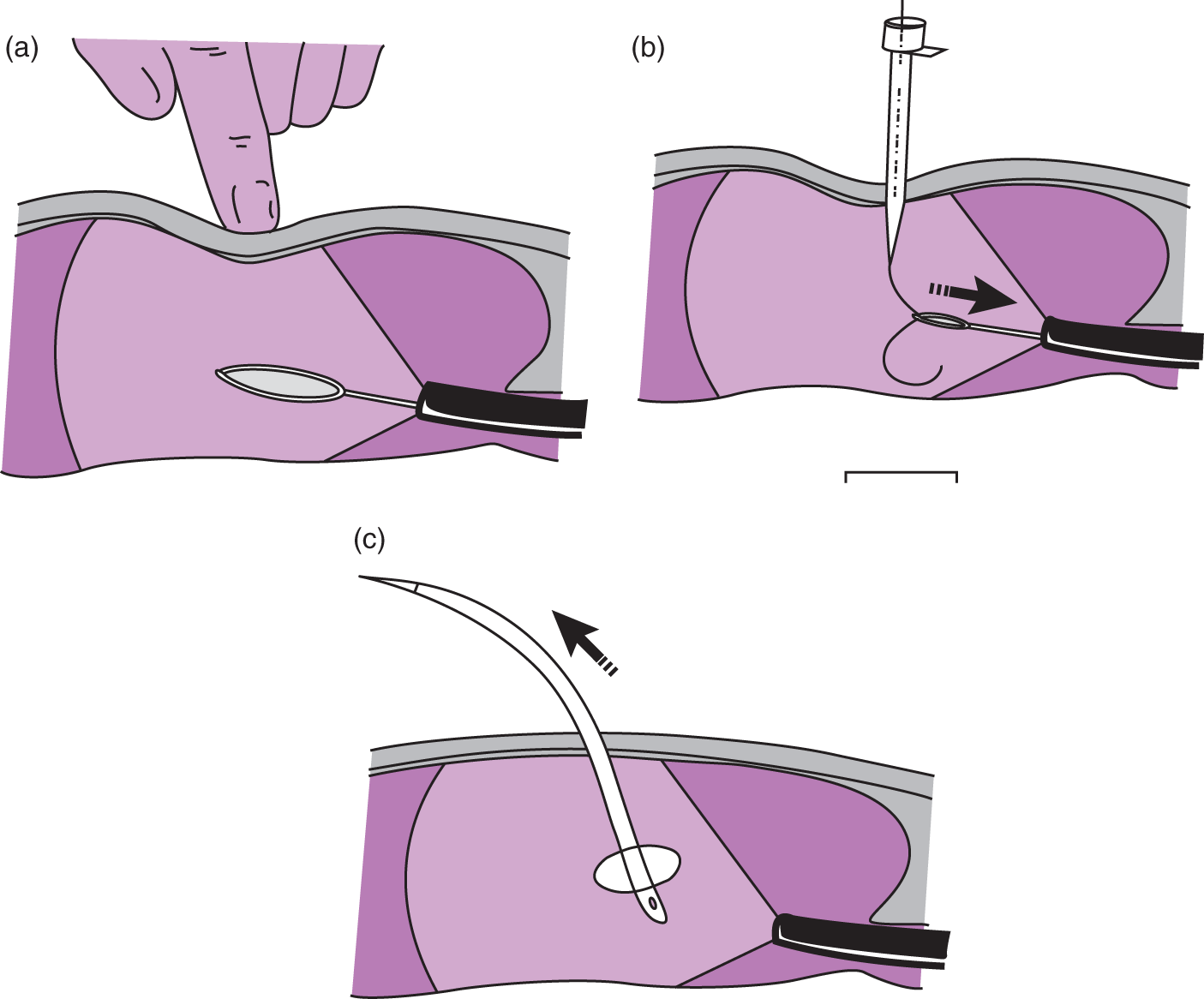
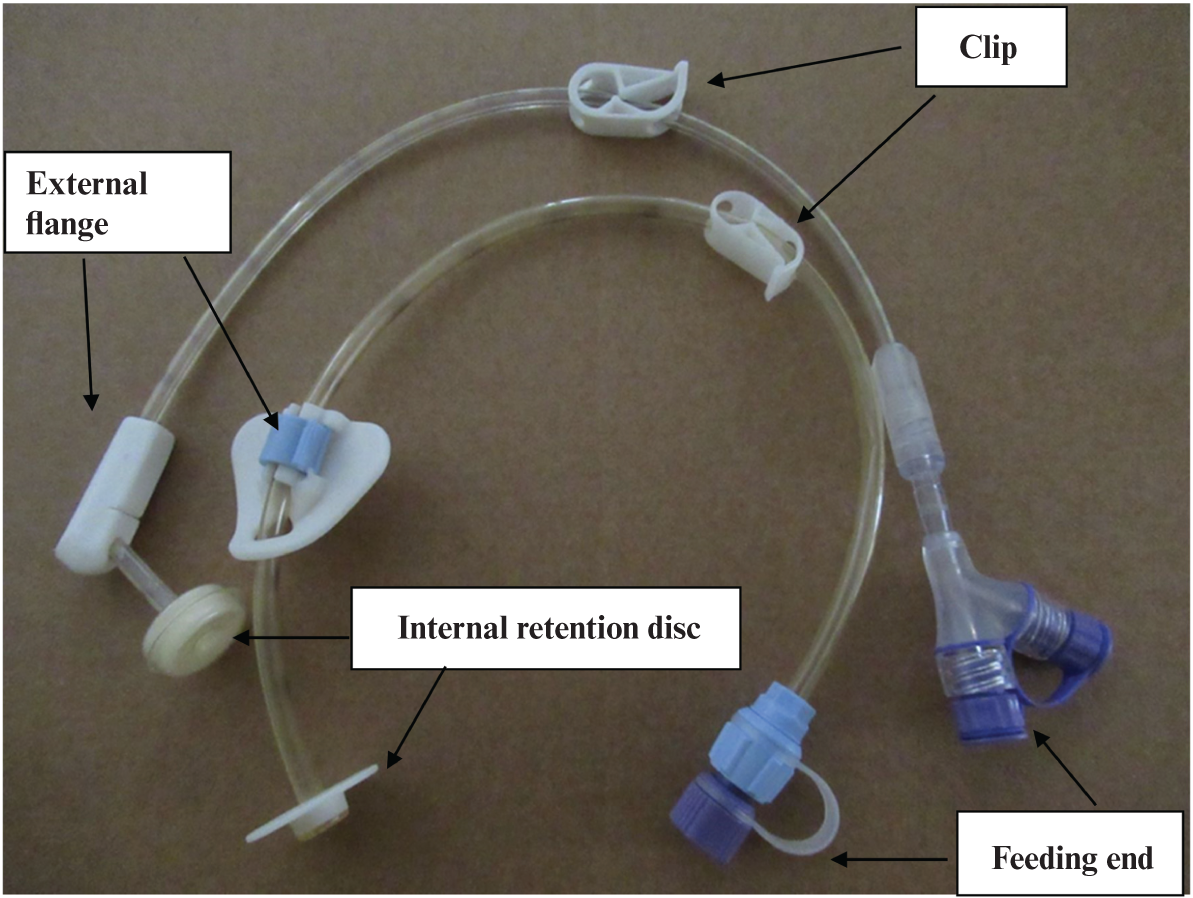
In 1980, Gauderer et al. reported a technique to insert a feeding tube that did not require a laparotomy – the percutaneous endoscopic gastrostomy (PEG), which uses an endoscope to insert a gastrostomy tube. Under general anaesthetic, the endoscope is passed through the mouth, down the oesophagus and into the stomach. A light at the end of the endoscope, along with finger indentation is used to identify a suitable position in the stomach to place the tube (Figure 30.1a). The skin is cleaned and a small incision is made in the skin, a wide-bore needle is passed through the incision into the stomach. A guide wire is passed through the needle; this is grasped by forceps which is passed through the end of the endoscope (Figure 30.1b). The endoscope and guide wire are pulled up the oesophagus and out through the mouth. The PEG tube is attached to the guide wire at the mouth, the guide wire is then pulled out through the abdominal wall pulling the PEG tube into the stomach, and an endoscope is then passed to check tube position (Figure 30.1c). Figure 30.2 shows examples of PEG tubes.
FIGURE 30.1 Percutaneous endoscopic gastrostomy tube placement (Cotton & Williams 1996). Reproduced with kind permission.
FIGURE 30.2 Percutaneous endoscopic gastrostomy (PEG) tubes and component parts.
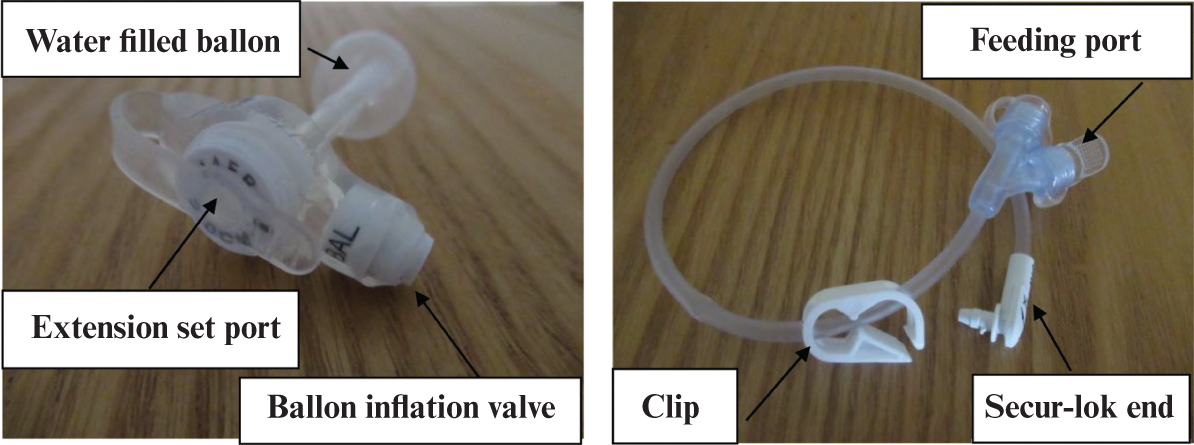
This PEG tube needs to remains in situ until the stoma tract has healed, usually 6–8 weeks, and can then be replaced. It can be replaced with a G-tube or low-profile skin-level feeding tube more commonly called a button (see Figure 30.3). Both of these gastrostomy tubes are held in the stomach by a water filled balloon (see Figure 30.4).
FIGURE 30.3 Low-profile skin level gastrostomy tube in situ (button).
Heuschkel et al. (2015) notes that a button gastrostomy lies flush with the skin, providing a more acceptable and less obtrusive way to connect an extension set and tube feeds.
All planned care should adopt an appropriate model of nursing, for example Casey (1988) and Roper et al. (2000). Casey’s model looks at working in partnership with families and it is important to work with Jane’s family as they will be providing her ongoing care following discharge. Coleman et al. (2003) further explore the concept of family and carer participation by looking at a practice continuum tool. This highlights an important concept in children’s nursing, identifying that there will be times during Jane’s care where it will be appropriate for it to be all nurse led, for example in the immediate postoperative period, moving through to times where it is all parent or family led, for example just prior to discharge home having completed training for home enteral tube feeding. It is important though to negotiate how, and indeed how much family involvement there is on an individual family basis Watts et al. (2014). Although Roper et al. (2000) address 12 activities of daily living (see Chapter 1) this chapter will only address maintaining a safe environment, personal cleansing and dressing, and eating and drinking in relation to postoperative care and discharge planning.
Only gold members can continue reading. Log In or Register to continue