Chapter 39 ENDOCRINE HEALTH
STRUCTURE AND FUNCTION OF THE ENDOCRINE SYSTEM
ENDOCRINE GLANDS AND HORMONES
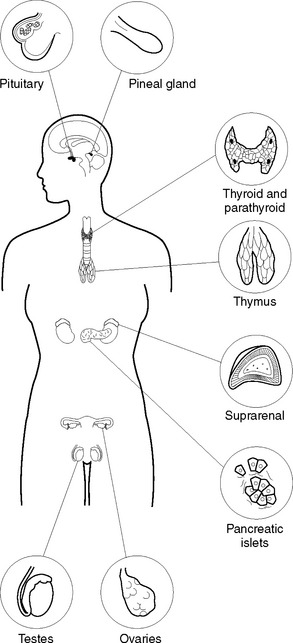
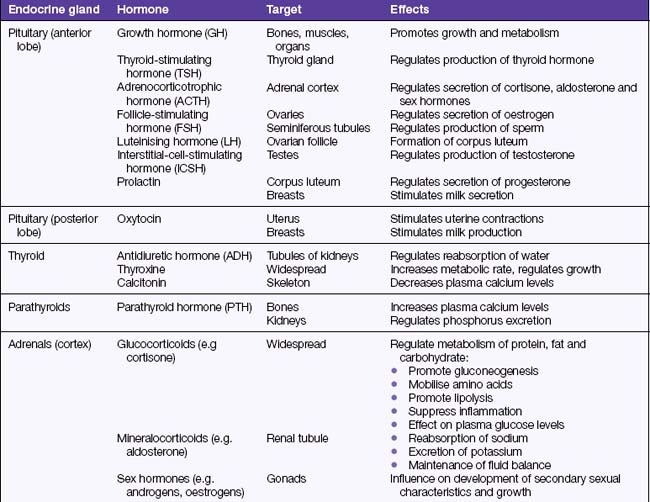
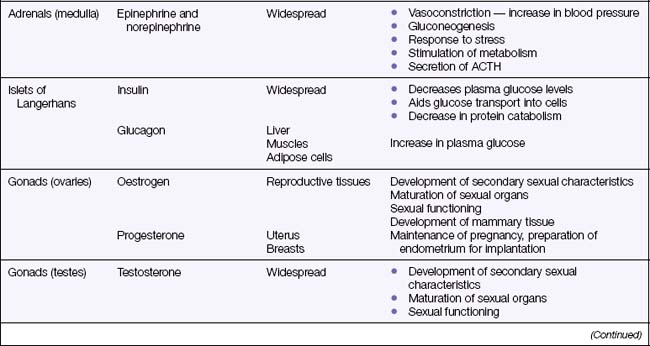
A hormone is a chemical substance secreted into the blood by an endocrine gland (Figure 39.1). The hormone is transported via the blood to areas of the body where it is needed to stimulate a specific cellular activity. Target organs are those that respond to a particular hormone. Some hormones can control other hormones by influencing their action, metabolism, synthesis and transport. A hormone can be described as a chemical regulator that integrates and coordinates cellular activities. Hormones are either steroids or proteins, and only target cells have the ability to respond to a specific hormone. After entering the blood, some hormones become bound to plasma proteins, while others are transported in an unbound state. Most hormones are continuously secreted at a rate determined by stimulation of the gland that releases them. Table 39.1 lists all the major hormones.

THE PITUITARY GLAND
DISORDERS OF THE PITUITARY GLAND
Hyperpituitarism
Hyper-function of the anterior pituitary gland commonly results from a tumour, which creates pressure on cerebral structures and causes neurological manifestations, such as severe headaches and visual disturbances, or excessive secretion of pituitary hormones, with consequent increased stimulation of the target organs. It is a chronic progressive disorder marked by hormonal dysfunction and skeletal overgrowth, which can appear in two forms: gigantism and acromegaly.
Hypopituitarism
Diagnostic tests
Testing posterior pituitary function includes the water-deprivation test, which is performed when the client’s symptoms indicate diabetes insipidus. This test is based on the principle that withholding fluid for several hours stimulates secretion of ADH. In a person suspected of having diabetes insipidus, the urine may be tested to determine specific gravity. A low specific gravity is suggestive of diabetes insipidus.
THE THYROID GLAND
DISORDERS OF THE THYROID GLAND
Hyperthyroidism
Graves’ disease
An autoimmune disorder, Graves’ disease is a common hyperthyroid disease. Antibodies stimulate the thyroid gland, leading to glandular hypertrophy. Graves’ disease more commonly affects young women. Symptoms include all the characteristics of hyperthyroidism — tachycardia, nervousness, hyperactivity and excitability. The individual will have a voracious appetite but loses weight and can be quite underweight. Diarrhoea is common, as peristaltic rate increases. Excessive sweating and extreme thirst are also common, because of the increased metabolic rate. One outstanding characteristic of Graves’ disease is that of exophthalmos, or protrusion of the eyeballs, which is due to oedema in the tissues behind the eye, and does not resolve even when the hyperthyroidism is corrected. A serious complication of Graves’ disease is thyroid storm (or crisis), which is discussed in Clinical Interest Box 39.1.
Goitre
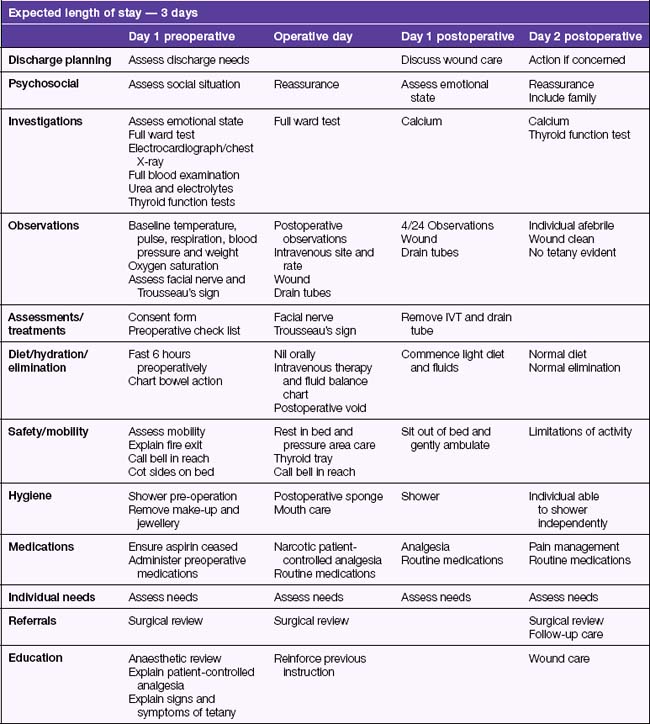
Management of hyperthyroidism involves assisting the individual and their family to manage the symptoms associated with hyperthyroidism until it is controlled with medication, or surgery if indicated. Surgical intervention may involve a subtotal thyroidectomy, which removes part of the thyroid gland, leaving enough gland to produce adequate thyroid hormone, or a total thyroidectomy may be performed if the gland is cancerous. A person who has had a total thyroidectomy requires long-term hormone replacement. The critical pathway in Table 39.2 outlines the nursing care of a client undergoing thyroidectomy surgery.
Hypothyroidism
Hypothyroidism is characterised by a decreased secretion of thyroid hormones. Hypothyroidism may be congenital or it may develop later in life. Cretinism is the congenital form of hypothyroidism and results from absence or underdevelopment of the thyroid gland or it may occur from severe maternal iodine deficiency during pregnancy. The manifestations of cretinism are related to a marked depression of metabolic processes and progressive mental impairment. Typically the infant is overweight, lethargic, has dry thick skin, coarse features, a broad flat nose and protruding tongue and abdomen. If the disease goes unchecked, sexual organs fail to develop and muscle growth is retarded. Treatment is started as soon as diagnosis is made and involves lifelong thyroid hormone replacement therapy (HRT).
Myxoedema is acquired hypothyroidism and develops when the thyroid gland stops functioning effectively. Hypo-thyroidism can also result from surgical intervention used to correct hyperthyroidism. The most common natural cause of hypothyroidism is an autoimmune disorder, Hashimoto’s disease. Symptoms of hypothyroidism are the opposite of those of hyperthyroidism. The individual is fatigued, drowsy, sensitive to cold temperatures, gains excessive weight, has thin nails and brittle hair, decreased pulse and respiratory rates and irregular menstruation. Hypothyroidism responds well to HRT and symptoms may disappear after a few months of treatment.



