Outbreaks and deliberate releases – SARS, toxins and biological agents
Unusual illnesses – deliberate release of infectious and chemical agents416
Poisoning with nerve agents421
Key nursing skills in outbreaks and deliberate releases422
How Infection Spreads
• close contact with unrecognised infected persons
• infectious respiratory secretions – cough and sneeze
• true airborne transmission (‘aerosol’)
• faecal and oral transmission
• contact with contaminated body surface (shaking hands)
• touching contaminated external surfaces
The possibility of an outbreak of an unfamiliar infection or of disease caused by bioterrorism cannot deflect the ward staff from basing all their initial management of seriously ill patients on the principle of probability: common things occur commonly. Thus an outbreak of severe pneumonic illness is more likely to be due to Legionella from say a faulty cooling tower (as in a 2003 outbreak in Montpellier) than from SARS or an airborne terrorist release of plague. A patient with progressive paralysis is far more likely to be suffering from the Guillain–Barré syndrome than from botulism, and a haemorrhagic rash more likely to be meningococcal septicaemia than Ebola virus.
Nonetheless, there is an issue of early recognition because, in their initial stages, these rare infections and toxins share clinical features with more commonplace conditions. The fact that deliberate infections and mass poisonings have taken place in recent years means further attacks are likely. Staff should therefore remain vigilant and plans must be in place. Previously, the responses to outbreaks and toxic releases have been characterised by:
• inadequate preparations
• late recognition
• poor communications
It is critical that the most up-to-date information is to hand. Local expertise will be limited, although there is increasing experience with strict respiratory protection through its use in multi-drug-resistant TB. Fortunately, international experience and guidelines are freely available electronically through several important websites (→ further reading p. 424).
There are several basic principles involved.
• An awareness of new threats and the emergence of novel infections/agents
• An appreciation that there will be no previous personal experience with cases
• The need for immediate up-to-date information from the internet
• The need to review protocols and procedures in the light of new information
• The skills of infection control in highly contagious patients
• The need for timely communication
• The rapid involvement of designated staff and resources
Severe Acute Respiratory Syndrome
SARS is uncommon, but it provides an important lesson in how an Acute Medical Unit may have to deal with the emergence of a new and highly infectious disease.
In February 2003, a doctor from the southern Chinese province of Guangdong became ill while staying at a Hong Kong hotel. Twelve other guests became infected, of whom seven had rooms on the same floor. These index cases moved on – spreading SARS to Vietnam, Singapore, Canada, Ireland and the US. By mid-April it had infected almost 3500 people in 27 countries, causing widespread panic. By May 2003, scientists had identified the infecting organism as a coronavirus (now known as SARS-CoV), which is normally an animal virus but which had crossed species to man. By July, the outbreak was over, having infected more than 8000 people with an 11% mortality rate.
SARS is spread like TB or influenza, in droplet form, but in spite of infection control measures, 25% of the cases occurred in exposed healthcare workers.
The implications of making a tentative diagnosis are so profound regarding isolation measures and public health protection that it is vital to be aware of the precise diagnostic criteria (case definition).
Case definition of SARS
Possible case
A patent who is ill enough to be in hospital with a high fever (> 38°C) and coughing, difficulty with breathing or dyspnoea and with chest X-ray changes of pneumonia who, within 10 days before the onset of symptoms:
• has been in an area that has been designated by the World Health Organisation to be a zone of potential re-emergence of SARS (currently mainland China and Hong Kong)
or
• has been in close personal contact with a probable case of SARS
Probable case
• Patients with a clinical diagnosis of SARS (possible cases) in whom preliminary laboratory tests are positive
Confirmed case
• Probable case in whom further tests are positive
Management of a possible case of SARS
Patients with suspected SARS are likely to be severely ill and have the clinical picture of acute pneumonia. While confirmation of the diagnosis is awaited, they should be treated along conventional guidelines for severe pneumonia, but with the additional need for strict infection control.
Detailed guidance for infection control in possible cases of SARS should be available through a local protocol and can also be found at the Health Protection Agency website.
The patient should wear a surgical mask – within the constraints imposed by their oxygen requirements – and should be nursed in a negative-pressure single room. All healthcare workers entering the room must comply with infection control:
• neck-to-heel gowns and gloves – to be left in the room before leaving
• a respirator mask conforming to EN149:2001 FFP3, such as the 3M mask: 1873 V. Staff using an FFP3 mask must be fit tested
• cap and goggles or visor – to be removed, with the mask, once outside the room
• boots
• strict hand washing in alcohol – before and after leaving the room
Surgical masks versus particulate respirators
Surgical face masks are designed to prevent droplet emission and to act as a barrier to splashes of liquid. They will capture microorganisms in the exhaled breath, but do not protect against airborne infection: for this an appropriate respirator is needed. Respirators are high-filtration masks that prevent inhalation of sub-micron sized particles. They do not filter the wearer’s expired air. To be used safely and to maintain a high filtering efficiency, the respirator must be fitted correctly, with a less than 10% leak.
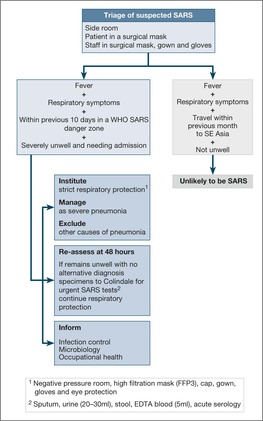
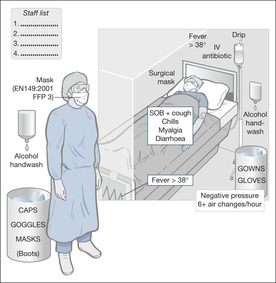
Fig. 11.1 gives an overview of the initial pathway for a potential case of SARS. Fig. 11.2 summarises the strict infection control measures that are required. The clinical management of SARS is the same as for severe community acquired pneumonia, with fluid replacement and i.v. antibiotics. High-flow oxygen, above 6L/min, is to be avoided, as it increases the risk of droplet spread: administer 30–40% oxygen using a Ventimask. Oral prednisolone (40–60mg daily) in severe cases probably improves the prognosis. Daily chest films are essential for monitoring these patients, because the pneumonia characteristically progresses with alarming speed. There is a high chance of the patients needing ventilation – particularly if they are elderly or have co-morbidity. Close liaison will be needed with the ITU, and probably with a designated Regional Centre.
Other Emerging Infections
SARS is only one example of new infectious diseases that have profound implications for Public Health. In August 1999, eight similar cases of encephalitis were admitted to hospitals in the Northern Queens district of New York. Four of the individuals were paralysed and needing ventilation. All eight usually spent their evenings out of doors in the vicinity of breeding sites for Culex mosquitos, which were suspected to be spreading a virus. Subsequent investigations of a substantial number of bird deaths in the area and of the patients identified the offending organism: West Nile Virus. The lessons from the successful recognition of this disease include:
• an awareness of the importance of clustering of cases
• the value of good communication
• excellent cross-professional working
More recently, in 2003, a virulent avian flu virus broke out in South East Asia. The virus, the H5N1 strain of bird flu, crossed the species barrier from domestic duck to man and killed 20 people in Thailand and Vietnam. Many believe that a major flu pandemic from this type of source is inevitable. SARS and influenza spread in the same way, so that similar infection control measures would be required.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


