Obtaining a history, including the patient’s signs and symptoms, current health patterns, and previous past medical history, will help in identifying ear, nose, and throat (ENT) problems and developing an individualized plan of care.
Key Signs and Symptoms
Epistaxis.
When did the bleeding first begin? Did it occur spontaneously or occur after facial or nasal trauma, nose blowing, digital manipulation, or recent nasal or sinus surgery? In many cases, anterior bleeding commonly flows from the nasal vestibule and, in reclining position, will drip into the throat. Posterior bleeding commonly causes dripping in to the oropharynx when upright or supine. Nasal endoscopy or examination via anterior rhinoscopy is performed to confirm the site of bleeding.
Unilateral or bilateral? What side of the nose is the bleeding coming from, and if bilateral, on what side did it begin? Ask patient about measures employed to control the bleeding thus far.
Assess current medication history: Is the patient taking acetylsalicylic acid (ASA, aspirin), antiplatelet agents, or anticoagulants? When was the last dose taken?
Is there a history of current oxygen therapy? Is there a history of chronic bleeding disorders? Obtain results of recent bloodwork: complete blood count (CBC), prothrombin time (PT), International Normalized Ratio (INR), or partial prothrombin time (PTT).
Headache.
Exactly what parts of the head or face hurt? Is it pain or a pressure sensation? Use the PQRST Method of Pain Assessment with emphasis on location, duration, and symptom onset.
Assess for associated neck, dental, or jaw pain, nausea, vomiting, visual changes, and/or sensitivity to light or sound. Assess for associated nasal congestion, postnasal drip, or clear or purulent rhinorrhea. Assess for history of migraine disease.
Sore throat. Assess onset and duration of symptoms, previous medical treatment, and symptom response.
Is it accompanied by swollen glands, high fever, nasal congestion, and postnasal drip? Assess for associated weight loss; head, neck, or ear pain; voice changes; neck mass; trismus; or difficulty breathing. Has the patient been able to eat or drink?
Is it acute or chronic? Was there any exposure to others with throat infection?
Nasal congestion.
Is it acute or chronic? Accompanied by fever and purulent drainage? Assess severity and duration of symptoms, associated purulent or clear rhinorrhea, fever, facial pain or sinus tenderness, itchy eyes, sneezing, or postnasal drip. If symptoms are chronic, assess if worsened with changes in barometric pressure, vary with seasons, or brought on by odors or allergen exposure.
Assess for current/chronic history of use of nasal sprays containing oxymetazoline, or if the patient is experiencing anosmia/microsmia (loss of sense of smell or diminished sensitivity). Ask if the patient has had previous history of nasal polyps, previous nasal or sinus surgery, or nasal fracture.
Hoarseness.
Assess history of recent surgical procedures involving the head or neck, recent endotracheal intubation, radiation treatment to the head/neck, history of tobacco/alcohol use, occupation as vocal performer, or history of lung disease with use of inhaled steroids, chronic or recent antibiotic therapy, symptoms of gastroesophageal reflux.
Is it acute (less than 2 weeks), recurrent, or chronic (more than 2 weeks)? Assess onset and duration of symptoms, subjective impairment in communication or voice-related quality.
NURSING ALERT Hoarseness for longer than 2 weeks in a smoker is an indication for ENT evaluation and laryngoscopy.
Assess for recent URI symptoms, associated dysphagia, odynophagia, globus sensation (sensation of something in the throat), throat pain, weight loss, ear pain, neck mass or enlarged lymph nodes in neck, hemoptysis, or shortness of breath.
Earache (otalgia).
Is it worsened by manipulation of the auricle or is it a deep, throbbing pain? Is there otorrhea? Assess onset and duration of pain using the PQRST Pain Scale. Assess for associated erythema or edema of the external ear canal or external auricle, pruritis, hearing loss, or otorrhea. Is the pain intermittent or constant?
Were there preceding upper respiratory infection symptoms? Is the pain associated with hearing loss, aural fullness, vertigo, headache, or fluctuation of hearing? Has there been any recent dental procedures?
Assess history for nighttime bruxism, clenching of the jaw or teeth, malocclusion, or pain worsened with movement of the jaw, dental pain, or swelling of the muscles of mastication.
Assess for ear pain that occurs with swallowing and associated symptoms of head and neck cancer.
Hearing loss.
Was it sudden or gradual in onset? Assess subjective onset of hearing loss. Did the patient experience sudden or gradual onset of the hearing loss? Is there associated tinnitus, vertigo, aural fullness, or ear pain?
Unilateral or bilateral? Assess for history of noise exposure; recreational shooting, occupational, acoustic trauma, or history of chronic otitis media. Assess for history of familial/hereditary hearing loss.
Dizziness.
Is the patient light-headed or experiencing vertigo (as if the room or self is spinning). Assess for subjective lightheadedness, room spinning, or imbalance. Are symptoms acute or chronic and associated with symptoms of fluctuation of hearing, aural fullness, or tinnitus (symptoms of Ménière’s disease).
Is the dizziness associated with a change in head or body position? Do symptoms occur with rolling over in bed, looking up or bending over, or when going from sitting to standing? Are there feelings of presyncope, history of syncopal episode when rising from sitting to standing? Are there changes in blood pressure associated with lying, sitting, and standing?
Assess for duration of symptoms and associated nausea, vomiting, headache, or focal neurological symptoms.
Current Health Patterns
Inquire about nutrition, dental care, normal mouth care habits, dental caries, use of partial or full dentures, stress-related grinding, clenching, or clamping of teeth.
Ask about history of alcohol, smoking, use of a pipe, and smokeless tobacco. Is there a personal history of human immunodeficiency virus (HIV), sexually transmitted disease, recreational drug use, or human papillomavirus (HPV)?
Determine personal hygiene about ears. Are cotton swabs or other objects used for cleaning or to relieve itching? Does the patient wear hearing aids or ear plugs?
Is there any loud noise exposure? Is there history of noise exposure via recreational shooting, or in the patient’s occupation? Ask about use of noise protection when exposed to prolonged and loud noise. Is there family history of hearing loss?
Does the patient frequently strain voice through talking, singing, or shouting? Is the patient a singer?
What medications is the patient taking? Have antibiotics been used? For how long?
Past Medical History
Is there a history of allergic rhinitis, other allergy symptoms, immunotherapy, chronic or recurrent sinusitis, previous nasal surgery, chronic otitis media, chronic pharyngitis, history of snoring, or obstructive sleep apnea?
Is there any immunosuppressive illness, such as diabetes mellitus, cancer, HIV infection, autoimmune disease, recent radiation or chemotherapy?
Is there a history of previous thyroid, carotid artery, or other surgery involving the laryngeal nerve?
Any history of previous or recent head, facial, or nasal trauma?
See Chapter 5, page 57, for physical assessment of the ears, nose, throat, and neck.
Diagnostic Tests
Audiometry
Description
Audiometry is the most basic and accurate testing to determine and measure hearing ability. The results are plotted on a graph known as an audiogram. Testing is performed by an audiologist. The following points below describe aspects of audiometry:
Pure tone threshold audiometry is the lowest level at which sound is heard across various sound frequencies. This is compared to normative data to measure hearing loss and used to monitor hearing sensitivity over time.
Speech audiometry provides information about the patient’s communication ability. Speech reception threshold is defined as the softest level at which the patient can repeat a word. Speech recognition or speech discrimination is the percentage of words that a patient can repeat accurately at the comfortable listening level. This helps to determine ability to understand conversational speech.
Pure tune testing is performed by presenting pure tones via air and bone conduction. Air conduction testing is done by presenting pure tones at various octave levels from 250 to 8,000 Hz through a transducer, such as insert earphone or cushion headphone. The patient sits in a soundproof booth and the audiologist presents tones and the patient is asked to indicate when the sound is heard. Testing by bone conduction is done with use of a bone oscillator, which is placed on the mastoid of the test ear and pure tones are presented at 500, 1,000, 2,000, and 4,000 Hz.
Immitance testing includes tympanometry and acoustic reflex testing.
Acoustic reflex testing measures the response of the stapedius muscle in response to auditory signals. It provides information about the acoustic and the facial nerves, as well as information about a conductive or sensioneural hearing loss.
Tympanometry measures the changes that occur to the tympanic membrane and middle ear when changes in air pressure are introduced into the ear canal. It can provide information about eustachian tube dysfunction, middle ear fluid, tympanic membrane perforation, patency of pressure-equalizing tubes, and middle ear disease such as otosclerosis.
Nursing and Patient Care Considerations
The patient wears earphones and signals upon hearing a tone.
A soundproof room is used to increase accuracy.
No special patient preparation or participation is necessary for tympanometry.
Cineradiography
Description
This motion study is performed to study the functional dynamics of the pharynx and esophagus.
It provides a more physiologic examination than esophagram (barium swallow). Mucosal detail is seen better with cineradiography, whereas video capture allows more dynamic evaluation with less radiation.
“Modified barium swallow” evaluates laryngotracheal aspiration while a speech pathologist provides various consistencies of food and swallowing techniques. An esophagram evaluates the pharyngeal and esophageal mucosa.
Nursing and Patient Care Considerations
The patient is usually kept NPO the night before surgery.
The patient will be given radioprotective gear to prevent radiation from reaching other parts of the body.
Electronystagmography
Description
Electronystagmography is the recording of eye movements, specifically nystagmus, during various oculomotor and vestibular testing. Videonystagmography is the recording of eye movements using infrared video image analysis in three dimensions. The pattern of nystagmus, in conjunction with the patient’s neurotological examination and clinical history, may provide information about the underlying etiology of the patient’s symptoms.
Used to establish the diagnosis of Ménière’s disease, vestibular neuronitis or labyrinthitis, benign paroxysmal positional vertigo (BPPV), or migraine-associated vertigo and to assist in ruling out vestibular pathology in a patient with symptoms of dizziness.
The test takes place in a dimly lit room, with the patient on an examination table, and lasts for 60 to 90 minutes.
Electrodes are placed on the forehead and lateral to each eye in electronystagmogram (ENG) testing. Video goggles are used in videonystagmography. Eye movements are recorded in response to various position changes and visual stimuli, with eyes open and eyes closed.
Caloric testing is the evaluation of nystagmus induced by warm or cold water irrigation into the external ear canals. Caloric testing can also be obtained by instilling cool and warm air into the ear canal. Caloric testing is used to measure the degree of vestibular dysfunction. Testing of patients with a normally functioning vestibular system will induce vertigo.
The audiologist may perform the vertebral artery test with older adults, patients who have history of neck trauma, or patients in which vertebral artery disease is suspected. Patients that elicit symptoms when the head is hyperextended may not be able to have portions of the positional testing completed.
Nursing and Patient Care Considerations
Patient preparation includes avoiding a heavy meal before the procedure and avoiding caffeine and alcohol for 48 hours before the procedure.
Medications that may affect the vestibular system, such as sedatives, anti-anxiety agents, narcotics, and medications ordered for dizziness, may be held for several days before the procedure.
The patient will receive instructions from the facility/provider who will be administering the test for specific medications that will need to be held and for how long before testing is performed. The patient should be counseled in the importance of following these preprocedure instructions, as they may affect the accuracy of the testing.
GENERAL PROCEDURES AND TREATMENT MODALITIES
Nasal Surgery
Types of Surgery and Indications
Facial Trauma and Nasal Fractures
Nasal bone fractures are common after blows to the nose during sports activities, interpersonal altercations, motor vehicle accidents, or falls. These can be diagnosed via physical examination or nasal/facial images, including x-rays or computed tomography (CT) scans.
Techniques of repair of nasal fractures include closed reduction or open reduction.
Closed reduction may be performed by ENT surgeon by applying force, internally and externally, to move the septum back into proper position. This may be done under local/general anesthesia, in operating room, or in office with local anesthesia. Closed reductions are ideally performed 5 to 10 days after the injury when the bones are still mobile.
Open reduction can also be done for older, healed fractures several months after the injury.
Repair and stabilization of other maxillofacial fractures usually require an operating room procedure for wiring or plating.
Nasal Septal Surgery
Septoplasty is an intranasal procedure performed under general anesthesia to remove portions of, straighten, or trim the septal bone and/or cartilage. Silastic splints are sutured on either side of the septum to stabilize the repositioned septum. The splints are removed several days postoperatively. This surgery is performed to treat chronic nasal obstruction and may be done in conjunction with sinus surgery to promote a clear nasal airway.
Submucosal turbinate reduction or excision of middle turbinate concha bullosa is an intranasal procedure performed under local or general anesthesia in the operating room to surgically trim, excise, or reduce tissue in the nasal cavity that contributes to nasal obstruction. May be done in conjunction with septoplasty.
Rhinoplasty
Involves changing the nose’s external appearance. Grafted cartilage or bone harvested from other parts of the body may be used.
A septorhinoplasty may be done when there are external and internal nasal deformities.
Sinus Surgery
Functional endoscopic sinus surgery (FESS) is corrective sinus surgery performed under general anesthesia in the operating room using direct visualization via a rigid nasal endoscope or, more recently, with assistance of image-guided systems. Image-guided systems utilize CT scans to provide surgeon with intraoperative landmarks and map.
Diseased mucosa is removed and the natural sinus ostia are widened to facilitate the normal sinus drainage patterns.
In addition to nasal and sinus conditions, surgery may also be used to treat traumatic optic neuropathy, cerebrospinal leaks, nasolacrimal duct obstruction, dysthyroid orbitopathy, posterior orbital lesions, and choanal atresia.
Packing may be placed intraoperatively depending on surgeon’s preference and amount of bleeding. Packing is usually very small, filling only the area adjacent to the sinus ostia, so is not visible except for a retrieval string extending outside the nasal ala.
Balloon catheter sinuplasty: The procedure uses a small balloon catheter to open blocked sinus passageways. The procedure is done to widen and restructure the blocked passageways without surgical removal of bone and tissue (see Figure 17-1).
Other approaches to the sinuses, such as the Caldwell-Luc procedure (opening under lip to enter maxillary sinus and strip out diseased mucosa), may be performed but newer techniques are more often utilized. A nasoantral window (creating an opening between the maxillary sinus and the anterior inferior nose), and anterior/posterior ethmoidectomies may be perfomed, as well as opening and draining the frontal or sphenoid sinuses. The patient with historically extensive postoperative nasal and sinus packing is rarely seen and is now used only in selected complicated cases with extensive bleeding.
Figure 17-1. Balloon catheter sinus surgery. A catheter is introduced through the nose and into the sinus ostia, where the balloon is inflated to enlarge the sinus opening and promote drainage.
Preoperative Management
The head of bed should be raised to promote drainage, lessen edema, and make patient more comfortable.
Intermittent cold compresses and pain medications should be utilized, as ordered.
Antibiotics may be used preoperatively to reduce bacterial colonization of nose and sinuses.
The patient should be advised that a sensation of pressure may be felt in the nasal area during surgery performed under local anesthetic.
The patient should be counseled about the possible use of packing with some surgeries, which may be removed several days postoperatively
Instructions for stopping aspirin, nonsteroidal anti-inflmmatory medications and antiplatelet and anticoagulant medications will be provided by the surgeon and individualized after collaboration with the patient’s cardiologist or primary care provider.
NURSING ALERT
In most cases, the patient should avoid use of aspirin, nonsteroidal antiinflammatory drugs, anticoagulants, antiplatelet agents, and herbal medications such as Ginkgo biloba, garlic, green tea, and any other drugs that may affect platelet function before surgery. If patient has taken these medications within a week of surgery, make sure surgeon is notified.
Complications
Hematoma/hemorrhage: Septal hematoma or postoperative bleeding. A septal hematoma will need to be drained by surgeon immediately if this should occur.
Local infection—contaminated nasal packing is an excellent culture medium for pathogens. Most patients are treated postoperatively with antibiotics, but this is surgeon-specific.
Aspiration.
Pressure necrosis (from packing) may occur, but the current trend is toward less packing.
Blindness from orbital hematoma or unintended orbital involvement in endoscopic sinus surgery.
Cerebrospinal fluid (CSF) rhinorrhea from unintended or traumatic violation of the cribriform plate. This is commonly referred to as a CSF leak.
Pulmonary decompensation.
Nursing Diagnoses
Ineffective Breathing Pattern (nasal airway clearance) related to nasal packing and swelling.
Risk for Aspiration related to bleeding, inability to blow nose.
Deficient Knowledge related to performance of nasal hygiene.
Impaired Oral Mucous Membrane related to mouth breathing.
Risk for Infection related to alterations in nasal/sinus mucous membranes and drainage patterns.
Nursing Interventions
Facilitating Breathing and Comfort
Keep head elevated (three to four pillows) day and night to minimize swelling. This also promotes comfort.
Apply cold compresses or ice packs intermittently for 24 hours to lessen edema and discoloration and to promote comfort. (Use great caution and only with approval of surgeon after rhinoplasty.)
Advise the patient that packing will be removed within 1 week of placement.
Encourage the use of a humidifier to relieve crusting of nasal mucosa and prevent irritation from dryness in nose and throat.
Encourage relaxation techniques and deep-breathing exercises for anxiety associated with nasal passages being blocked.
Be alert for worsening pulmonary conditions, such as asthma, chronic obstructive pulmonary disease, and sleep apnea, when the nose is congested or packed.
Encourage use of analgesics but caution overuse, which may cause respiratory depression. Medicate with analgesics as prescribed. Topical decongestants may be prescribed to relieve nasal congestion in the first few days postoperatively. Pain after nasal surgery is usually mild to moderate.
Preventing Bleeding and Aspiration
Monitor closely for bleeding; check for increased swallowing, blood dripping down back of throat (use flashlight and tongue blade), expectoration of large amounts of clots and blood.
Change the 4 × 4 gauze pad under the nose as it becomes soaked with blood; bleeding should gradually decrease. Teach family and patient that blood will be bright red at first and will gradually lessen over the next several days.
Notify the surgeon if bleeding increases. Expect a temporary minor increase in bleeding with vomiting, sneezing, ambulation, or crying in the first 48 hours.
Teach the patient that mild nausea is normal postoperatively and may be from anesthesia, pain medications, swallowing of blood; however, be alert for continuous trickle of blood postnasally.
Instruct the patient not to blow nose but to blot secretions with tissue and “sniff and spit.”
Regularly observe and document visible packing retrieval strings external to nose, taped to cheek, if present. Postoperative instructions should be given upon discharge with appointments for postoperative splint removal or sinus debridement, if indicated. Surgeon will discuss activity and work restrictions specific to the patient.
Ensuring Proper Nasal Hygiene
Encourage the patient to use a vaporizer to help relieve crusting of nasal mucosa from dryness.
Remind the patient that sneezing, straining, and nose blowing increase venous pressure and can result in bleeding/hematoma.
Advise the patient to keep the mouth open while sneezing if unable to control sneezing.
Teach the patient an appropriate method of nasal hygiene as approved by surgeon. After FESS, the patient will need regular appointments for sinus debridement by the surgeon. Advise the patient sinus irrigation will need to be done to control nasal crusting and to facilitate healing (see Patient Education Guidelines 17-1).
In general, the patient may gently clean nasal ala area with saline and/or peroxide for comfort, but large crusts should be removed by surgeon or allowed to work themselves free.
Instruct the patient to avoid environmental irritants, especially smoke.
Protecting Oral Mucous Membranes
Administer frequent mouth care because the patient is forced to breathe through the mouth.
Use flexible straw to sip mouthwash for rinsing purposes.
Encourage fluid intake and use of lip protectant.
Preventing Infection
Be alert for uncontrolled postoperative pain, fever, foul odor or taste in mouth, or unusual drainage.
Administer or encourage prophylactic antibiotics on time, if ordered.
Advise patient to keep follow-up appointment for splint removal, packing removal, and sinus debridement.
PATIENT EDUCATION GUIDELINES 17-1
Nasal Saline Irrigation
This procedure will help clear nasal passages of crusted drainage that may be blocking the sinus opening. Perform this once or twice per day to feel less nasal congestion and to help sinuses drain.
Prepare saline solution right before irrigation. Commercially prepared sinus irrigation kits are readily available that contain packets and sinus rinse bottle.
Mix ½ tsp table salt and ¼ tsp baking soda with 8 oz warm distilled or sterilized water until well dissolved.
Lean forward from the waist over a sink.
Fill a bulb syringe (1 oz infant ear or nasal bulb) or rinse bottle with the saline solution by squeezing it in the solution and letting it fill by suction. If using sinus rinse kit, follow instructions.
Insert the tip of the filled syringe into one nostril, aimed toward the eye away from the nasal septum.
Squeeze the syringe gently and feel the solution run backward in the nose and out the other nostril and possibly down the back of the throat and out of the mouth.
When comfortable with this procedure, you may be able to rotate head forward, backward, and from side to side to irrigate the sinuses as well as the nose.
Nose irrigation with bulb syringe or sinus irrigation kit.
Patient Education and Health Maintenance
Tell the patient to notify the surgeon immediately for uncontrolled postoperative pain, any visual changes postoperatively, fever, unilateral clear nasal discharge with leaning the head forward, uncontrolled excessive nasal bleeding, dyspnea, or blanching or necrosis of the external nasal tissues or the palate while packing is in place.
After Caldwell-Luc procedure or rhinoplasty, advise the patient that numbness in operative area may be present for several weeks to months.
Instruct the patient to avoid strenuous activity, lifting, and trauma to nose.
After splint removal, avoid trauma to nose and sleep in supine position. Operating surgeon will provide more specific postoperative instructions.
Excessive sun exposure should also be avoided after rhinoplasty for 1 year due to a tendency for hyperpigmentation.
If a nasal splint is present, tell patient to avoid getting it wet; do not attempt to remove it.
Advise the patient that postoperative follow-up may need to continue for several weeks to months to monitor for excess scar formation or cosmetic deformity.
Evaluation: Expected Outcomes
Mouth breathing without difficulty.
No excessive bleeding, protects airway without aspiration.
Nasal and palatal tissues free from blanching or darkening.
Oral mucous membranes dry, but pink and intact.
Afebrile, no signs of infection.
Ear Surgery
Ear surgery may involve the tympanic membrane, the middle ear cavity, the mastoid, or the inner ear. It may be done for perforation of the eardrum to facilitate drainage and remove diseased tissue in cases of infection or cholesteotoma, to relieve vertigo, or to treat hearing loss.
Types of Surgery
Myringotomy—creating a surgical opening into tympanic membrane (with knife or laser) for possible drainage tube insertion.
Tympanoplasty—reconstruction of diseased or deformed middle ear components (see Table 17-1).
Type I (myringoplasty)—purpose is to close perforation by placing a graft over it to create a closed middle ear to improve hearing and decrease risk of infection and cholesteatoma. Perforation is closed using one of the following:
Fascia from temporalis muscle (this is the most commonly used material).
Vein grafts from hand or forearm.
Epithelium from auditory canal (eustachian tube).
Type II to V—suitable replacement (polyethylene, Teflon or titanium prosthesis, bone, cartilage) is used to maintain continuity of conduction sound pathway. The necessity of a two-stage procedure is determined.
First stage—eradication of all diseased tissues; area is cleaned out to achieve a dry, healed middle ear.
Second stage—performed 4 to 6 months after first stage; reconstruction, using grafts.
Mastoidectomy—removal of mastoid process of temporal bone.
Simple or cortical mastoidectomy is done via a postauricular approach but the bony ear canal is left intact.
Modified radical mastoidectomy or canal wall down mastoidectomy is done with a meatoplasty for the best results. A wide excision of the mastoid and diseased middle ear contents through a postauricular incision is performed with the bony canal being drilled out. A new larger ear canal is created that gives better access to the areas where cholesteatoma usually occurs (the attic and antrum).
Stapedectomy—removal of footplate of stapes and insertion of a graft or prosthesis
Stapedotomy—removal of the stapes suprastructure, allowing a hole to be created with a laser in the stapes footplate. The base of the prosthesis will be inserted into the opening and the other end will be crimped around the incus.
Labyrinthectomy—destruction of the labyrinth (inner ear) through the middle ear and aspiration of the endolabyrinth.
Endolymphatic decompression and shunt—release of pressure on the endolymphatic system in the labyrinth and creation of a shunt for fluid to the subarachnoid space or the mastoid.
Cochlear implant—implantation of electronic device that bypasses the damaged cochlea and stimulates auditory nerve.
Osseointegrated implantation for placement of a hearing implant for single-sided deafness or for conductive hearing loss (Baha system or Oticon implantable hearing system).
Preoperative Management
Hearing function is fully evaluated.
Antibiotics are given to treat infection.
The patient is prepared emotionally for the effects of surgery.
Careful assessment for signs of acute infection is performed, which may delay surgery.
Table 17-1 Types of Tympanoplasty
MIDDLE EAR DAMAGE
REPAIR PROCESS
Type
Tympanic Membrane
Ossicles
I
Perforated
Normal
Close perforation—myringoplasty
II
Perforated
Erosion of malleus and/or incus
Close perforation; graft against incus or whatever remains of malleus
III
Tympanic membrane destroyed or widely perforated
Rest of ossicular chain destroyed but stapes are intact and mobile
Grafts implanted to contact the normal stapes
Tympanostapedopexy
IV
Tympanic membrane destroyed or widely perforated
Ossicular chain destroyed. Head, neck, and crura of stapes destroyed. Stapes footplate mobile.
Expose mobile stapes footplate—graft implanted. Air pocket between graft and round window provides protection
The cavum minor operation
V
Tympanic membrane destroyed or widely perforated
Ossicular chain destroyed. Head, neck, and crura of stapes destroyed. Stapes footplate fixed.
Make opening in horizontal semicircular canal; graft seals off middle ear to give sound protection for round window
Tympanoplasty and fenestration of lateral semicircular canal
Postoperative Management
Antibiotics may be continued to prevent local and central nervous system (CNS) infection.
Patients are advised to have limited activity for the first 24 hours to decrease symptoms of nausea and vertigo (if the inner ear was disturbed) or to prevent disruption of prosthesis.
Analgesics, anti-emetics, and antihistamines are given, as needed.
The patient is positioned to promote drainage but maintain some immobility. Using two extra pillows to elevate the head, thereby preventing edema for 2 weeks, is a good idea.
Patient is often seen 7 to 10 days after surgery to remove any metal stent placed. Additional packing may be removed up to 6 weeks postoperatively if prosthesis or graft procedure was performed. Often an ear drop will be used to slowly dissolve remaining packing over a period of 6 to 8 weeks to give some weight to the grafted tympanic membrane.
Hearing will be reevaluated after edema has subsided and healing has occurred. The time frame for this varies by procedure but may be as long as 3 to 4 months after surgery to allow for healing.
With an osseointegrated implant, a fitting of the outer processor is usually delayed by 2 to 3 months to allow the bone to osseointegrate around the implant. In children, or in radiated bone, this may be done in two stages separated by 6 months to allow for a slower rate of bone growth.
Cochlear implant activation and placement of the outer speech processor and external transmitter occurs approximately 4 weeks after surgery to allow for healing.
Acute Pain related to surgical incision and swelling.
Risk for Infection related to invasive procedure.
Risk for Injury related to vertigo.
Nursing Interventions
Relieving Pain
Administer or teach self-administration of analgesic, as indicated, postoperatively.
Tell the patient to expect pain to subside within first few hours with simple procedures or within first day or two with major procedures.
Position the patient for comfort following the instructions from the surgeon.
On side with surgical ear upward to maintain graft position and immobility.
Lying on side with surgical ear down to promote drainage from ear canal.
Position of patient preference.
Elevate the head of bed to reduce swelling and pressure.
Advise the patient to avoid sudden movement. Use pillows for support.
Preventing Infection
Reinforce external dressings, as needed, until after first changed by surgeon, then change when saturated to prevent bacterial growth in damp dressings.
Loosely pack cotton or gauze in ear canal, as indicated, without causing increased pressure.
Do not probe or insert anything into ear canal.
Administer or teach self-administration of antibiotics, as prescribed. Do not use eardrops unless specifically ordered postoperatively.
Wash hands before ear care and instruct the patient not to touch ear.
Take care not to get the dressing or ear wet.
Advise the patient not to blow nose, which could cause nasopharyngeal secretions to be forced up eustachian tube into middle ear.
Instruct the patient to report any increased pain, fever, ear inflammation, or drainage, indicating local infection.
Be alert for headache, fever, stiff neck, or altered level of consciousness, which may indicate CNS infection.
Ensuring Safety
Be aware that dizziness or vertigo may occur for the first several days postoperatively.
Maintain side rails up while the patient is in bed.
Assist the patient with ambulation for the first time after surgery and as needed thereafter.
Encourage the patient to move slowly because sudden movements may exacerbate vertigo.
Administer or teach self-administration of anti-emetics and antihistamines, as ordered and as needed; watch for sedation.
Instruct the patient not to blow nose, cough, lean forward, or perform Valsalva’s maneuver to avoid disrupting graft or prosthesis, aggravating vertigo, or forcing bacteria up the eustachian tube. If coughing or blowing nose is necessary, do so with open mouth to relieve pressure.
Patient Education and Health Maintenance
Advise the patient that there may be a temporary hearing loss for a few weeks after surgery because of tissue edema, packing, and so forth. The effects of a hearing restoration operation will not be known for several weeks and additional rehabilitation may be necessary to optimize results.
Advise the patient to protect the ear, perform dressing changes, or place loose cotton in outer ear, as indicated. Replace cotton twice daily or sooner if saturated by drainage.
Encourage follow-up for packing removal, as directed.
Instruct the patient to avoid sudden pressure changes in the ear.
Do not blow nose.
Do not fly in a small plane. The date for which a patient may fly is individualized by their surgery and surgeon’s preference.
Do not dive.
Advise against smoking.
Tell the patient to protect ears when going outdoors for the first week. A cotton ball is all that is needed.
Tell the patient to avoid getting ear wet until completely healed.
Tell the patient to avoid crowds or exposure to colds so upper respiratory infection is prevented.
Instruct the patient about signs and symptoms of complications to report.
Advise the patient that facial nerve paralysis may be temporary and to increase fluid intake through a straw during this time.
Evaluation: Expected Outcomes
Verbalizes relief of pain.
No signs of infection.
Ambulates without difficulty.
CONDITIONS OF THE MOUTH AND JAW
Candidiasis
Evidence Base
Pappas, P., Kauffman C. A., & Andes, D. (2009). Clinical management guidelines for the management of candidiasis: 2009 update by the Infectious Disease Society of America. Clinical Infectious Diseases, 48, 503-535.
Candidiasis is an opportunistic fungal infection commonly caused by Candida albicans. It may be localized in the mouth and pharynx, but may also occur in the esophagus. Candidiasis can become a source of systemic dissemination, particularly in high-risk persons.
Pathophysiology and Etiology
Commonly seen in individuals with immunosuppression from disease states or treatment regimens such as diabetes, cancer, or HIV and those receiving radiation therapy and/or chemotherapy.
May be caused by altered oral environment from xerostomia, use of inhaled steroids for asthma and COPD, or chronic antibiotic therapy, preexisting infections, poor oral hygiene or nutritional status, or wearing dentures.
Clinical Manifestations
Oral examination reveals diffuse, white, painless plaques. Underlying mucosa may be erythematous.
May be asymptomatic but may result in mild oral discomfort, burning, or alterations in taste.
Patients with disease spread beyond the oral cavity may present with chest pain, pain and difficulty with swallowing, or hoarseness.
Diagnostic Evaluation
Microscopic smear of plaques shows characteristic hyphae.
Oral fungal culture positive for C. albicans.
Occasionally, biopsy of lesions may be necessary to rule out leukoplakia (premalignant plaques).
Management
Topical antifungal medications such as nystatin suspension or clotrimazole troches are most often used.
Systemic treatment is indicated if topical agents fail or for esophageal cases with fluconazole, ketoconazole, or amphotericin B.
Topical oral rinses or preparations containing combinations of hydrocortisone, diphenhydramine, antifungals, or antibiotics may be used to enhance healing and to lessen discomfort.
Viscous lidocaine may be used topically to coat the oral mucosa before meals to lessen pain and enhance oral intake.
Oral prostheses may also be treated to avoid harboring and reintroducing infection.
Complications
Candidal infection throughout the GI tract.
Candidal sepsis in patients who are immunocompromised.
Nursing Assessment
Carefully examine oral cavity daily to monitor lesions as well as response to prescribed antifungal therapy.
Assess level of pain; administer analgesics, as prescribed; and monitor response to analgesics.
Assess nutritional status and effect of pain on oral intake. Monitor oral intake, nutritional and hydration status, weight loss/gain, signs of dehydration.
Teach patients that are prescribed inhaled steroid therapy for asthma/COPD to rinse mouth after each use to prevent oropharyngeal candidiasis.
Nursing Diagnoses
Imbalanced Nutrition: Less Than Body Requirements related to oral discomfort.
Deficient Knowledge related to antifungal therapy.
Nursing Interventions
Attaining Adequate Nutrition
Administer analgesics, as prescribed, 30 to 60 minutes before meals.
Provide soft foods, soothing liquids; avoid temperature extremes.
Provide gentle suctioning if pain becomes so severe that patient cannot handle secretions and provide intravenous (IV) fluids.
Ensuring Adequate Therapy
Administer antifungal agents, as prescribed. Observe the patient for proper use of topical preparation.
Make sure that mouth is clean and free of food debris before administering drug.
For swish-and-swallow preparations, tell the patient to swish and hold in mouth for at least 5 minutes before swallowing.
For troches, have the patient suck until dissolved.
Observe for signs and symptoms of systemic drug adverse effects: nausea, vomiting, diarrhea. Renal, bone marrow, cardiovascular, hepatic, or neurologic toxicities may occur in patients receiving systemic therapy with underlying chronic disease states.
Explain the importance of continuing therapy for duration prescribed.
Patient Education and Health Maintenance
Instruct high-risk patients about daily oral examination and signs and symptoms to observe.
Teach the patient to avoid highly seasoned foods, extremes in temperature, alcoholic beverages, and smoking, all of which irritate the oral mucosa.
Encourage good oral hygiene.
May need to refrain from wearing dentures due to oral discomfort.
Encourage the patient on long-term systemic antifungal therapy to follow up for liver function test monitoring, as directed.
Evaluation: Expected Outcomes
Adequate intake of liquids and soft foods as evidenced by stable body weight, signs of dehydration.
Swishes oral suspension for 10 minutes before spitting or swallowing.
Herpes Simplex Infection (Type 1)
Also known as cold sores or fever blisters, herpes simplex virus (HSV; usually type 1) is commonly associated with lip and oral lesions 80% of the time. HSV-1 causes genital outbreaks in 20% of the cases.
Pathophysiology and Etiology
After a primary infection and the patient produces antibodies, the virus remains latent in the sensory ganglia.
Recurrent herpes labialis may by precipitated by sun exposure, fever, oral trauma, fatigue, emotional upset, hormonal changes, and other factors.
The spread of HSV-1 is through respiratory droplets or exposure to infected saliva via a break in the skin or mucous membranes.
HSV type 2 (and rarely HSV type 1) is associated with genital lesions and is sexually transmitted.
Clinical Manifestations
Prodromal period—tingling, soreness, burning in area where lesion will develop.
Small vesicles appear on erythematous, edematous base, frequently near the mucocutaneous junction of the lips and adjacent skin.
May also occur in oral mucosa, especially in immunocompromised persons.
Vesicles rupture, causing ulcerations.
Lesions heal spontaneously in 7 to 14 days.
Diagnosis and Management
No diagnostic tests are necessary but serologic testing may be done. The diagnoses of herpes simplex is made from viral culture from skin vesicles, serology, or monoclonal antibody testing.
Treatment may not be necessary if cases are mild and are usually short lived.
Comfort measures, such as mild oral or topical analgesics.
Good hygiene to prevent spread to self and others.
Antiviral agents are available to decrease the duration of symptoms.
Penciclovir 1% cream—FDA approved; applied every 2 hours while awake at earliest sign. If used within 1 hour of outbreak, will decrease duration of viral shedding.
Acyclovir 5% cream may be used on topical lesions. Oral or IV antivirals may also be used if clinically indicated.
Nursing Interventions and Patient Education
Advise adequate rest and nutrition and avoidance of identified triggers.
Advise that virus is transmitted through close contact, such as kissing and sharing food and cups, so avoid these from prodromal period until well healed.
Recommend good handwashing and hygiene.
Apthous ulcers or canker sores—not caused by HSV-1.
Temporomandibular Disorders
Temporomandibular disorders are conditions affecting the jaw joint that consist of one or more of the following:
Myofascial pain—pain in the muscles serving the jaw (temporalis, masseter, medial and lateral pterygoids), neck, and shoulder.
Internal derangement of the jaw joint (dislocated or displaced joint disk or injured condyle).
Degenerative joint disease (eg, arthritis).
Pathophysiology and Etiology
Causes include rheumatoid or osteoarthritis; scleroderma; ankylosing spondylitis; trauma; teeth clenching or bruxism (teeth grinding). Neoplasms and acute infections such as parotitis, dental infections, and peritonsillar abscesses cause referred ear pain and should be differentiated from temporomandibular disorders.
Any mental and physical stresses can induce or exacerbate symptoms.
Above factors result in inflammation and muscle spasm of TMJ.
Clinical Manifestations
Pain at the joint, temples, mandible, or masticatory muscles may worsen with jaw movement. Referred muscle spasm of the neck, trapezius, and sternocleidomastoid muscle causes discomfort.
Clicking or crepitus from opening and closing of the jaw or popping of the joint.
Limitation of movement, dislocation, or jaw locking.
May be associated with headaches, earaches, or tinnitus.
Change in the bite where the upper and lower teeth do not match in the normal comfortable way.
May experience deteriorating oral hygiene or halitosis from limited oral opening (trismus), making dental hygiene difficult.
May experience difficulty chewing due to limited jaw excursion, resulting in altered diet and weight loss.
Jaw clicking alone is common and requires no workup or intervention if asymptomatic.
Diagnostic Evaluation
Diagnosis can usually be achieved by history and physical examination without extensive testing. Provocative maneuvers performed on physical examination that reproduce pain with opening and closing of the jaw are generally suggestive of TMJ arthralgia.
Dental and TMJ x-rays may or may not be helpful.
Occlusal analysis evaluates for malocclusion of the jaw and teeth in a bite position.
CT scan and magnetic resonance imaging (MRI) are usually normal unless there is underlying degenerative changes, fracture, or neoplasm of jaw or cervical spine.
Initial management employs jaw rest (soft, no-chew diet for 2 weeks, plus avoiding extreme jaw movements, such as wide yawning and gum chewing).
Anti-inflammatory/analgesic medications such as ibuprofen.
Application of warm, moist heat or ice packs.
Muscle relaxants may be prescribed.
Therapeutic nightguard or splint—to realign malocclusion or joint disk and to optimize muscle relaxation.
Physical therapy for gentle stretching and relaxing exercises with or without ultrasound (deep-heat) therapy—to enhance analgesia and muscle relaxation and to promote local tissue metabolism.
Check that transcutaneous electrical nerve stimulation reduces muscle spasm of head, neck, and back and reduces pain.
In general, conservative reversible measures above are employed as long as possible before progressing to invasive/surgical management.
Arthroscopy—investigational procedure to visualize joint, reposition disk, lyse adhesions, or debride joint.
Reserved for conditions not improved by medical management.
Complications include cranial nerve (CN) VII damage with facial paralysis and paresis, perforation of the external auditory canal, piercing of the middle cranial fossa.
Surgery—to remove the disk or reshape bony prominences.
Complications include malocclusion, CN VII damage, infection.
Nursing Interventions and Patient Education
Assess the character, frequency, location, and duration of pain. Evaluate what triggers and relieves the pain. Determine how effective previous treatments have been.
Explore the effect of the disorder on the patient’s lifestyle, especially eating habits. Assist the patient to alter methods of oral hygiene and eating if severe trismus is present.
Instruct the patient on the indications, dosages, and adverse effects of analgesics and anti-inflammatory medications.
Teach the patient proper use of heat therapies. Cold applications may be preferred by some patients to reduce pain and spasm.
Encourage the patient to perform active mouth opening, protrusion, and lateral movement exercises of the jaw for 5 minutes, four to five times per day, as prescribed, to stretch muscles and reduce spasm.
Encourage the use of soft food and liquid supplements during times of acute pain exacerbated by eating. Advise reduction of foods that require excessive chewing, such as raw vegetables, tough meat, nuts. Discourage gum chewing.
Explore tension-reducing modalities with the patient, especially progressive muscle relaxation to reduce muscle tension and spasm.
Encourage follow-up with dentist, oral surgeon, ENT specialist, or other caregiver, as indicated.
Encourage proper use of the night guard or dental splint, including periodic appointments to assess fit.
May need MedicAlert bracelet and preoperative anesthesia consultation for elective surgeries if maximum jaw opening is less than 30 mm, limiting access for airway intubation.
Maxillofacial and Mandibular Fractures
Fractures of the maxillofacial bones or mandible may occur as the result of industrial, athletic, and vehicular accidents; violent acts; and falls.
Pathophysiology and Etiology
Maxillofacial fractures usually occur due to blow to the cheek or face.
Mandibular fractures frequently occur due to blow to the chin.
May be nondisplaced or displaced, usually closed, and includes soft tissue injury.
May also occur as part of planned surgical reconstruction for jaw problems.
Injuries sustained in altercations or motor vehicle accidents may be associated with alcohol intoxication or recreational drug use.
Clinical Manifestations
Malocclusion, asymmetry, abnormal mobility, crepitus (grating sound with movement), pain, or tenderness.
X-rays (posteroanterior, oblique, occlusal, panorex)—to show fracture and possible displacement.
CT scan—to evaluate extent of complicated injuries.
Management
Maintenance of adequate respiratory functioning—may include oxygen support, endotracheal intubation, or tracheostomy. See Chapter 35, page 1197.
Control of bleeding—usually accomplished with direct pressure.
Reduction of the fracture—usually closed reduction.
Immobilization—depends on location, type, and severity of the fracture.
Barton’s bandage with a Kling or stockinette bandage.
Interdental fixation with rubber bands or wiring.
Intermaxillary fixation with rubber bands or wiring.
Interosseous fixation with open reduction.
Maintenance of adequate nutritional intake with liquid or soft diet—to maintain immobilization of fracture site.
Pain control—to promote comfort.
Control of infection with antibiotics in the presence of positive cultures.
Complications
Airway obstruction, aspiration.
Hemorrhage, infection.
Disfigurement.
Extraocular muscle entrapment/orbital globe displacement with resultant visual disturbance.
Acute drug or alcohol withdrawal.
Nursing Assessment
Obtain description of injury and review chart and diagnostic tests for extent of injury.
Continually assess respiratory status.
Assess level of pain.
Assess visual acuity and extraocular movement.
Assess for tremors, delirium or hallucinations, anxiety, and seizure activity related to alcohol or drug withdrawal.
Nursing Diagnoses
Risk for Aspiration related to immobilization of jaw.
Imbalanced Nutrition: Less Than Body Requirements related to pain, injury, and immobilization.
Acute Pain related to injury and surgical intervention.
Disturbed Body Image related to disfigurement of injury or surgical repair.
Risk for Injury related to complications of surgery.
Nursing Interventions
Preventing Aspiration
Maintain effective airway.
Elevate head of bed 30 to 45 degrees or position leaning over a bedside stand to reduce edema and improve handling of secretions.
Make sure suctioning equipment is readily accessible; teach patient oral and nasal suctioning; position on side or upright during suctioning.
Administer anti-emetic, as prescribed, for nausea and vomiting to prevent aspiration.
Make sure wire cutters or scissors are present for immediate removal of the wires or rubber bands if the airway becomes obstructed. (Vertical rubber bands or wires should be cut.)
Make sure that a method for calling the nurse (call bell) is within easy access for the patient at all times in case of emergency.
Monitor blood pressure, pulse, respirations, and temperature to note early onset of infection or aspiration.
Maintaining Nutritional Status
Administer liquid diet, as prescribed; place straw against teeth or through any gaps in the teeth. Teeth may initially be sensitive to hot and cold.
Position in upright position before, during, and for 45 to 60 minutes after all feedings.
Evaluate ongoing nutritional and hydration status; weight; intake, output, and specific gravity; laboratory values— 24-hour urea nitrogen, transferrin level, electrolytes, and albumin.
Advance to blenderized diet, as tolerated.
Make environment as pleasant as possible to enhance appetite—remove all sources of odor, decrease interruptions, position comfortably.
Increasing Comfort
Administer liquid or a suspension of analgesics, as prescribed—avoid opioids on an empty stomach, which may cause nausea and vomiting.
Administer diazepam as prescribed to reduce anxiety and control reflex muscle spasm.
Apply paraffin wax to the ends of wire fixation devices to decrease irritation to the gums and oral mucosa.
Apply petroleum jelly to the lips to decrease dryness and prevent cracking.
Strengthening Body Image
Provide firm reassurance regarding progress to reduce anxiety and allay fears.
Avoid unrealistic promises in relation to scars or disfigurement.
Allow the patient to choose the first time for looking in the mirror.
Provide privacy, as requested. The patient may be sensitive to appearance.
Preventing Complications
Provide mouth care every 2 hours while awake for the first several days, then four to six times per day.
Initially, provide mouth care with warm normal saline mouth swishes.
As diet is progressed, remove collected debris with a pressurized water stream cleaner and encourage the patient to brush teeth with a soft, child-size toothbrush.
Observe facial injuries for swelling, erythema, pain, or warmth to detect onset of infection.
Change facial dressings as needed to prevent soiling with secretions, food, or drainage, which may promote bacterial growth.
Provide alternative form of communication, such as magic slate or picture board, because maxillomandibular fixation limits articulating ability, making speech difficult to understand.
Patient Education and Health Maintenance
Encourage adequate nutrition—inform the patient and family that foods can be blenderized and thinned with juices or broths to a consistency that can be taken through a straw.
Explore with the patient options for maintaining proper oral care; encourage the patient to practice the options of choice.
Discuss the use of anti-emetic medications to prevent nausea and vomiting, stressing the complications this could cause.
Make sure the patient has wire cutters or scissors at all times and knows how to use them should airway obstruction occur.
Encourage follow-up health care visits, including counseling for alcohol or drug abuse.
Evaluation: Expected Outcomes
No evidence of aspiration.
Tolerates fluids through straw; maintains adequate body weight.
Expresses relief of pain.
Views self in mirror; notices improvement in appearance.
No signs of infection; oral hygiene maintained.
PROBLEMS OF THE NOSE, THROAT, AND SINUSES
Rhinopathies
Evidence Base
Distler, J. W. (2011). Environmental allergens: Diagnoses and management of Ig-E mediated disorders. American Journal of Nurse Practitioners, 15(9/10).
Rhinopathies are disorders of the nose that interrupt its normal functions of olfaction and warming, filtering, and humidifying inspired air. These include allergic rhinitis, nonallergic rhinitis, vasomotor rhinitis, and other conditions.
Pathophysiology and Etiology
Allergic rhinitis—immunoglobulin E (IgE)-mediated response causing release of vasoactive substances from mast cells (see page 1020).
Non-IgE-mediated allergy/sensitivity—exposure to irritants such as tobacco smoke, perfumes, soaps, hairsprays, air pollution, or certain foods may produce symptoms of nasal congestion, postnasal drip, or rhinorrhea but are not caused by inhalant allergy.
Nonallergic rhinitis includes infectious rhinitis, rhinitis medicamentosa, rhinitis of pregnancy, or vasomotor rhinitis.
Drug-induced (rebound rhinitis; rhinitis medicamentosa)—caused by excessive use of topical nasal decongestants. These products include oxymetazoline and phenylephrine. Many systemic medications may induce nasal congestion and stuffiness and include specific beta blockers, antihypertensives, and antidepressants.
Vasomotor rhinitis—consists of symptoms caused by autonomic instability with disruption of the normal balance of sympathetic and parasympathetic innervation. This produces nasal congestion, rhinorrhea, and postnasal drip. Symptoms may be manifested on exposure to cold weather or eating spicy, hot, or cold foods (gustatory rhinitis).
Rhinitis of pregnancy—nasal congestion resulting from estrogen-mediated mucosal engorgement, especially in the last trimesters of pregnancy, may also occur with oral contraceptive use, postmenopausal estrogen therapy, and during the last portion of the menstrual cycle. Edema of the nasal mucosa and turbinate congestion occur.
Nonallergic rhinitis with eosinophilia syndrome—patients have symptoms of rhinitis, negative allergy testing, but large number of eosinophils in nasal secretions. Treatment is similar to those with vasomotor rhinitis.
Manifestations of Allergic Rhinitis
Hypersecretion—wet, running/dripping nose or postnasal drip.
Eyes—edema of the conjunctivae, tearing and itching of the eyes, increase in vascularity, fine allergic shiners or dark staining under eyes.
Nasal cavity—congestion, pressure, or stuffiness (see Figure 17-2). Chronic nasal crusting and erythema around outer nares, turbinates are often swollen, edematous with pale or bluish hue. Allergic salute often seen in children caused by upward lifting of the tip of the nose with the hand.
Oral cavity—chronic mouth breathing, enlarged lymph tissue in the oropharynx, prominent vascularity or cobblestoning in posterior pharynx.
 NURSING ALERT Hoarseness for longer than 2 weeks in a smoker is an indication for ENT evaluation and laryngoscopy.
NURSING ALERT Hoarseness for longer than 2 weeks in a smoker is an indication for ENT evaluation and laryngoscopy.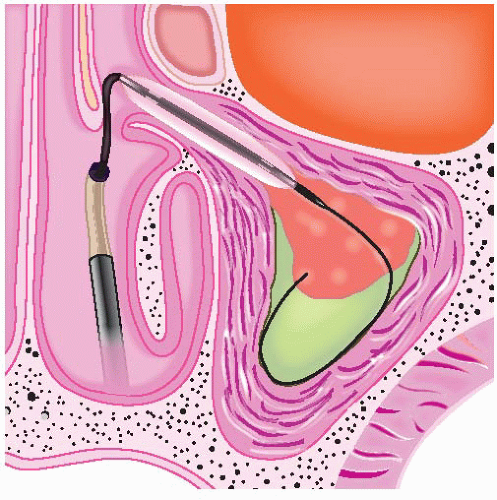
 NURSING ALERT
NURSING ALERT
 Evidence Base
Evidence Base Evidence Base
Evidence Base



