Chapter 9 CULTURAL DIVERSITY IN AUSTRALIA AND NEW ZEALAND
CULTURAL DIVERSITY IN AUSTRALIA AND NEW ZEALAND
Indigenous Australia was marked by cultural diversity long Before Cook (BC, as the late Oodgeroo Noonuccal used to say). Some 500 different Indigenous language groups occupied the whole of the continent (Berndt & Berndt 1988) and lived in well-defined socioeconomic, political, land-owning units (Elkin 1964). The situation was a little different in New Zealand (Aotearoa). Polynesian people settled the islands between 250 and 1150CE (Belich 1996). Known as Māori, they adhered to common cultural traditions, although there were some dialectic differences between the groups (Rice 1992).
In the late 18th century the British Crown claimed the continent of Australia as terra nullius; that is, unoccupied/empty and therefore open to settlement/annexation (see McGraw 1995; Reynolds 1987, 1989; Lippmann 1999). As a result, Indigenous Australians experienced dispossession and dislocation. For almost 200 years, governments created special laws and policies, which treated them as ‘non-human’ and controlled every aspect of their lives, including marriage, employment, education, recreation and religion. Today it could be argued that these policies and laws were intrinsically racist and abused Indigenous human rights by segregating, assimilating and controlling the minorities (see the work of Reynolds 1987; Broome 2001). This history has left its mark on Australian attitudes towards the country’s traditional owners as well as the life chances of today’s Indigenous Australians (see Saggers & Gray 1991; National Inquiry into the Separation of Aboriginal and Torres Strait Islander Children from their Families 1997; Tatz 2001; Dowd et al 2005).
In New Zealand, or Aotearoa, on the other hand, Britain recognised that it had to negotiate with sovereign, independent Māori groups (Orange 1987; Belich 1996). Perhaps, this was because the colonists could identify social structures and hierarchical power relations, marked by tribes, clans, chiefs and councils, not so very different from their own. In 1840 the British Crown signed the Treaty of Waitangi with Māori representatives of many of the multiple iwi (tribes) and hapu (sub-tribes) of New Zealand in order to ensure that further British settlement could take place. The Treaty of Waitangi was meant to safeguard Māoris’ existing property and citizenship rights (Durie 1994). This treaty and the passage of the Waitangi Tribunal Act of 1975 ensured that Māori claims for reparations could be dealt with legally. It ensured that New Zealand has had a very different colonial experience to that of Australia (Pearson 1996). Today, the Treaty of Waitangi and the Waitangi Tribunal Act offer a way to address some of the consequences of colonisation. They also provide a set of principles, outlined in the New Zealand Royal Commission of Social Policy, Volume II, 1988, to guide interactions with Māori people. These are the principle of partnership, the principle of participation and the principle of protection. Nevertheless, the process of Māori colonisation has resulted in structural inequality and widespread institutional racism, which have led to poverty and the breakdown of Māori social structure, culture, language, life chances and health (Walker 1990).
At the turn of the 20th Century, Australia and New Zealand essentially consisted of two kinds of populations — immigrants who were largely from Britain, and Indigenous peoples. Indeed, Australia ensured that its immigrants would, preferably, be of northern European descent by enacting the White Australia Policy after Federation. The policy was not repealed until 1973 (Eckermann et al 2006).
Today, Australian and New Zealand societies are composed of peoples from many cultures. As Eckermann et al (2008) have pointed out, roughly 22.5% of the Australian population has been born overseas and speaks a language other than English at home (Australian Bureau of Statistics [ABS] 2004). The background of immigrants has, however, changed over the years. Julian (2004) points out that since the 1980s, much more emphasis has been placed on skilled and business migration. Further, during the 1990s, Australia instigated a quota for refugees. Such refugees tended to originate from the latest sources of conflict. Thus:
Indigenous Australians constitute 2.4% of the total population in Australia (ABS 2004). The proportion of immigrants from Asia who annually migrate to Australia is now approaching the proportion from Britain and Ireland (Jupp 2002). In New Zealand, Māori people constitute 14.2% of the total population; 1 in 15 New Zealanders is of Asian descent, and 19.5% of the population has been born overseas (Statistics New Zealand 2003) — the majority of these have come from the United Kingdom and Ireland or the Pacific (including Australia). New Zealand’s consistent refugee policy has seen an increase in the number of refugees accepted into the country from Eastern Europe, Indochina and Africa (Statistics New Zealand 2001).
This is the context in which health care providers are expected to practise. They will encounter clients, their immediate and at times extended families, who belong to cultural groups different from their own. Consequently clients’ beliefs and values may appear, or indeed be, at odds with their own, the practices of Western medicine and nursing philosophies. How nurses respond to their clients’ beliefs and behaviours will determine how effective they will be in caring for and promoting their clients’ wellness.
WHAT IS CULTURE?
Over the years, writers have attempted to identify some of the more important aspects of culture which impact on people, their rules for operating, beliefs and values, history and tradition. Figure 9.1 sets out diagrammatically some of the many influences identified as shaping cultures and individuals within cultures.
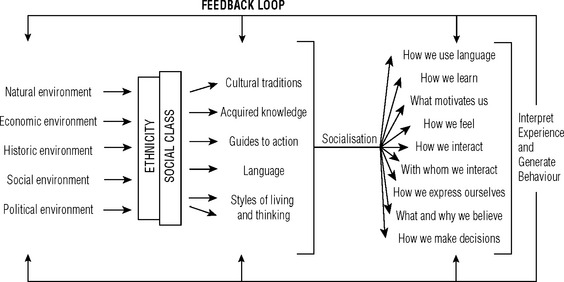
Figure 9.1 illustrates that socioeconomic, religious, political, historical and natural environments shape cultural values, beliefs, traditions and patterns of decision making. People learn about what is right and wrong, good and bad, important and unimportant; that is, their values, through socialisation, education and enculturation processes; from their families/friends/peers; through schools and training; and by contact with other groups. However, the environments in which individuals operate will influence their language, ethnicity and class and shape their preferred styles of interacting, learning and identity. These styles determine what motivates them to interact, with whom they prefer to interact and in what way.
This process of adaptation is important. Eckermann et al (2006) cite Bennett (1969:19) who defines adaptation as the ‘problem solving, creative, or coping element in human behaviour that permits a dynamic approach to environment [and culture]’.
Because cultures do not exist in a vacuum, people adapt on the basis of the particular social group with whom they share a distinct organisation, continuity and identity. Eckermann et al (2006) have argued that this group is not only ‘cultural’ — it is also based on socioeconomic–political characteristics; that is, social class. Individuals from different social classes are afforded different opportunities — they have access to varying levels of power, are permitted varying levels of input into decision-making processes and their power to change their life circumstances for the better vary greatly. Indeed Spencer and Inkeles (1976: 222–3) argue that:
Everyone belongs to at least one culture; that is, culture of origin. Many are also members of the culture(s) of their profession(s). They will also belong to a social class. In Australia and New Zealand there are many minority groups, groups which share cultural traditions different from the mainstream, but which belong to the same class as members of the mainstream do. Box 9.1 asks nurses to consider their own group membership.
Box 9.1 Considering personal culture
Look at yourself — how many cultures, personal and professional, have influenced you?
In what way, then does culture and class differ from ethnicity?
Some writers (e.g. Leininger 1978, 1995) believe that ethnicity and culture are different. They maintain that ethnicity relates to a group’s identity, history, language, nationality and religion, while culture refers to a group’s shared and learned values and beliefs, which guide action, thinking and decision making. The approach adopted in this chapter is different. As outlined in Figure 9.1, ethnicity and culture are considered part of the same thing. People cannot separate their environments — whether these be historical, religious or political — from their values and beliefs.
Eckermann et al (2006), have argued that ‘ethnic’ has come to mean ‘minority’ and has been used largely to eliminate labels such as ‘race’. Social scientists (see the work of Gould 1998, for example) have become aware of how inaccurate the concept ‘race’ is in terms of defining or categorising anyone, and how destructively it has seeped into people’s perceptions of others and their treatment of those who basically ‘look different’. Consequently, ‘ethnicity’ has become the less emotive categorisation, and in Australia the term ‘ethnics’ has taken over from labels such as ‘migrants’, ‘wogs’ or ‘reffos’.
Members of ethnic groups also belong to a variety of classes, because no single ethnic group fits neatly into one specific class. Consequently, both class and ethnicity affect people’s life chances — and their health — which is the reason why ethnicity has been specified as yet another ‘filter’ which affects the way people interpret, experience and generate behaviour, as outlined in Figure 9.1.
HOW DOES CULTURE INFLUENCE HEALTH?
Holistic definitions such as that of the World Health Organization (WHO), or of the National Aboriginal and Islander Health Organisation (NAIHO), emphasise the link between culture and health when they stress that health concerns ‘not just the physical wellbeing of the individual but the social, emotional and cultural wellbeing of the whole community’ (NAIHO 1982: 2). A similar viewpoint in New Zealand focuses on the synergy between people and the wider social, cultural, economic, political and physical environment (Durie 2001).
Lay and professional health behaviours and care practices are generally based on particular values and beliefs about health and the causes of illness and disease. Consequently, how people feel pain, how they interpret wellness ‘… will all depend on a person’s beliefs and value systems which are learned within a particular society and within a number of cultural contexts’ (Kanitsaki 1992: 2).
Despite the fact that health care providers know and accept that health beliefs and practices vary between cultures, and despite the fact that they tend to support a holistic view of health and wellness, the biomedical model of health dominates in Australia and New Zealand and has the most legitimacy, both socially and politically (Macdonald, in Davis & Dew 1999).
Nurses’ understanding of health and illness is influenced by their socialisation into the professional culture of nursing. Their training and the values and behaviours they accept as appropriate to their profession — that is, the professional culture of nursing — provides the blueprint for determining the definition of health and associated values, beliefs and practices. It is undoubtedly dominated by the biomedical ideology. Andrews (2003: 73–4) suggests that nurses often assume that their clients share their professional symbols and knowledge, assumptions and beliefs, and that they can speak and understand the same language. This can obviously lead to enormous misunderstandings.
Consequently, turn to Box 9.2 and reflect on your own attitudes, values, beliefs, practices and traditions acquired through the culture of nursing.
CULTURE CLASH AND CULTURE CONFLICT
If nurses are to develop appropriate skills to work across cultures, they need to understand the processes, which shape the way differences within and between groups are evaluated. Eckermann et al (2006) have argued that perceptions of differences depend on a number of complex interrelated factors such as ethnocentrism, stereotypes, prejudice, discrimination, power and powerlessness. Matsumoto and Juang (2004: 63) define ethnocentrism as follows:
Stereotypes are over-generalisations (see Allport 1982). They, too, are part of human life and thinking because people are encouraged, from an early age, to categorise the things around them. For example, it is possible to categorise an object as ‘table’ — whether it has four legs or one, it makes no difference. Consequently, over-generalisations always deprive the ‘object’ of individuality. As a result, when stereotypes are applied to people, they develop into ‘mindsets’ (whether these are positive or negative) which deny individual talents and abilities; for example, all southern Europeans are hot blooded.
The world is experiencing a particularly stressful period in this first part of the 21st century — mutual fear of ‘the other’ has been escalated by the 11 September 2001 terrorist acts in New York, the Bali bombings in 2002, the continuing war in the Middle East and political assassination in Pakistan in 2007. It would be naïve to assume that these events do not affect attitudes and beliefs; that is, stereotypes about Muslim immigrants and asylum seekers, or, indeed, the feelings of members of such minorities about themselves and mainstream society generally. As with other types of societal attitudes and beliefs, these stereotypes may influence interactions in many aspects of life, including hospitals, clinics and community health settings. Consequently it is important to be constantly vigilant when it is claimed that all Germans, Aboriginal people or Italians do this, or think that.
Obviously, our attitudes towards ‘the other’ — that is, people who are little known — would make no difference at all, if they were never encountered. However, when those who are prejudiced and hold stereotypes about the ‘other’ do have contact and belong to a powerful group, such as service providers, then their attitudes and beliefs can have a major impact on the people who are stereotyped. The issue of power, then, becomes extremely important. One way of understanding power comes from the work of the sociologist Max Weber (Bendix 1966), who identified three kinds of power: political, economic and social power.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


