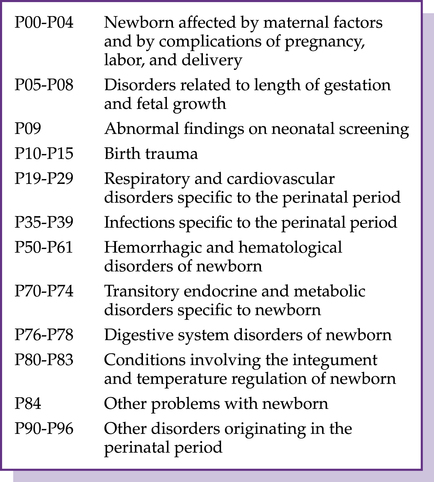
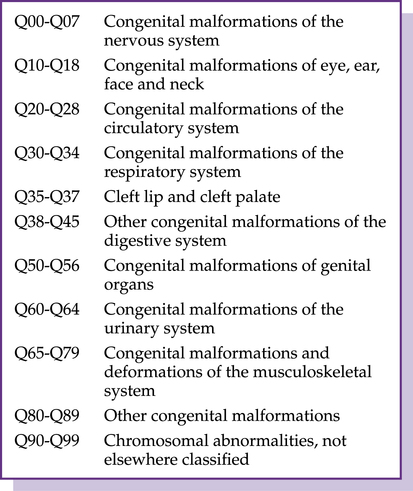
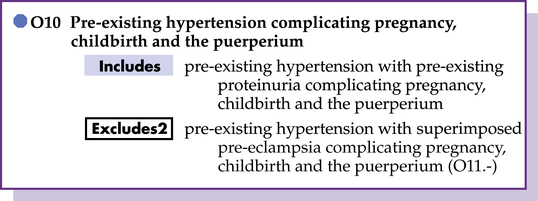
Chapter 6 Patricia Cordy Henricksen, MS, CHCA, CPC-I, CPC, CCP-P, PCS Education Director, Lexington Local Chapter AAPC After completing this chapter you should be able to 1. Review the pregnancy, childbirth, and puerperium coding. 2. Report services of certain conditions originating in the perinatal period. 3. Examine the congenital malformations, deformities, and chromosomal abnormalities. 4. Define the rules of symptoms, signs, and abnormal clinical and laboratory findings that are not elsewhere classified. 5. Identify the elements of coding injury, poisonings, and certain other consequences of external causes. There are times when the first-listed diagnosis for a pregnant female will not be a Chapter 15 code: There are conditions that are due to pregnancy, and those same conditions that may have been present prior to pregnancy, such as hypertension, are shown in Figure 6-1. If the category does not state pre-existing or pregnancy-related condition, the category may be assigned to either. TOOLBOX 1. When you reference “Pregnancy, complicated by, fetal, damage from, maternal, alcohol addiction,” what code are you directed to locate in the Tabular ____________________________ 2. Within the Tabular, the code you reference only has 4 characters, but there are 7th characters to assign to the code. What symbol is placed in the 5th and 6th character position? ___________________________________ 3. What 7th character is assigned to the code to indicate the fetal number? ___________________________ 4. What would be the code to report the diagnosis for Carol Jean? ________ The blocks of Chapter 17 are as illustrated in Figure 6–4. NEWBORN CONGENITAL ANOMALIES Example Newborn (infant) (liveborn) (single) Z38.2
Chapter-specific guidelines (ICD-10-CM chapters 15-21)
Pregnancy, childbirth, and the puerperium
Trimesters
less than 14 weeks 0 days from LMP
14 weeks 0 days to less than 28 weeks 0 days from LMP
28 weeks 0 days from LMP until delivery occurs

 If the physician documents that the pregnancy is incidental to the encounter, report Z33.1, Pregnant state, incidental, as a supplemental diagnosis and the reason for the encounter as the first-listed diagnosis.
If the physician documents that the pregnancy is incidental to the encounter, report Z33.1, Pregnant state, incidental, as a supplemental diagnosis and the reason for the encounter as the first-listed diagnosis.
Fetal conditions

Congenital malformations, deformations and chromosomal abnormalities
Diagnosis:
Newborn male delivered in the hospital by cesarean section and with Down syndrome (Trisomy 21)
Index:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



 “Education will be even more important for successful ICD-10 implementation. Understanding the Official Guidelines and the format of the new codes, learning the new codes, and translating the medical record documentation for this new system will be essential.”
“Education will be even more important for successful ICD-10 implementation. Understanding the Official Guidelines and the format of the new codes, learning the new codes, and translating the medical record documentation for this new system will be essential.”









 Exercise 6-1
Exercise 6-1