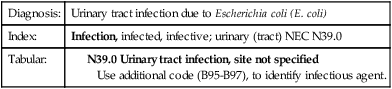
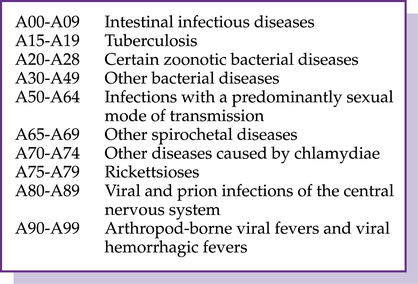
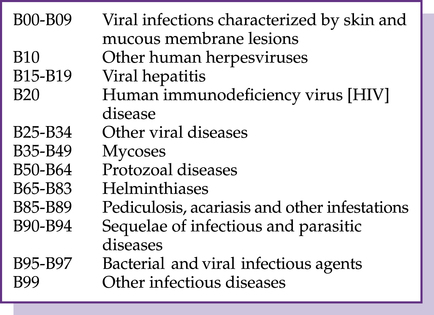
CHAPTER 4 After completing this chapter you should be able to 1. Review certain infectious and parasitic disease codes. 3. Assess the blood and blood-forming organs and certain disorders involving the immune mechanism codes. 4. Examine the endocrine, nutritional, and metabolic diseases codes. 5. Understand the mental, behavioral and neurodevelopmental disorder codes. 6. Examine the diseases of the nervous system codes. 7. Analyze the diseases of the eye and adnexa codes. 8. Comprehend the organization and reporting of the ear and mastoid process codes. 9. Recognize the diseases of the circulatory system codes. 10. Evaluate the diseases of the respiratory system codes. 11. Demonstrate the ability to report diagnoses with I-10 codes for Chapters 1-10. Chapter 1 in the I-10 Tabular is Certain Infectious and Parasitic Diseases (A00-B99), which classifies diseases according to the etiology (cause) of the disease. Because infectious and parasitic conditions can affect various parts of the body, the chapter contains a wide variety of codes and complex terminology. Examples The urinary tract infection is sequenced first, followed by the bacterial organism. The A codes include the blocks illustrated in Figure 4–1. B95.61 Methicillin susceptible Staphylococcus aureus infection as the cause of diseases classified elsewhere (MSSA) B95.62 Methicillin resistant Staphylococcus aureus infection as the cause of diseases classified elsewhere (MRSA) Examples TOOLBOX Robert has sepsis resulting from a postprocedural infection that is now complicating his care. 1. Sepsis resulting from a postprocedural infection is considered a ________________. 2. If the documentation stated that Robert’s sepsis was severe, you would reference what subcategory for code assignment? ______________________________ 3. When reporting severe sepsis, you would also report what dysfunction? ______________________________ The B codes include viral infections, mycoses (fungi), protozoal (microscopic animals), helminthiases (parasitic worms), pediculosis (louse), acariasis (mites), sequelae of infectious disease, and other infectious agents. The B codes are illustrated in Figure 4–2. Common codes reported with the B codes are herpes (B00), chickenpox (B01), herpes zoster (shingles, B02), measles (B05), and German measles (Rubella, B06). Chapter 2 of the I-10 contains codes C00-D49 to report neoplasms. There are extensive Guidelines that must be understood and followed to correctly code neoplasms. QUICK CHECK 4-2 1. According to the Neoplasm Guidelines, you would report a category _____________ code for a patient in leukemia remission and code _________________ for a personal history of leukemia. 2. When an encounter for a pathological fracture is due to a neoplasm, and if the focus of treatment is the fracture, a code from subcategory _____________ should be sequenced first, followed by the code for the _______________.
Chapter-specific guidelines (ICD-10-CM chapters 1-10)
Certain infectious and parasitic diseases
Diagnosis:
Urinary tract infection due to Escherichia coli (E. coli)
Index:
Infection, infected, infective; urinary (tract) NEC N39.0
Tabular:
Index:
Infection, bacterial, as cause of disease classified elsewhere, Escherichia coli B96.2
Tabular:

Codes:
N39.0, B96.2 Urinary tract infection due to Escherichia coli (E. coli)
A codes (a00-a99)
Sepsis, severe sepsis, and septic shock
 hypothermia or fever (<97°F or >100°F or < 38°C or > 36°C)
hypothermia or fever (<97°F or >100°F or < 38°C or > 36°C)
 increased respiratory rate (>20 breaths per minute or PaCO2 < 32 mm Hg)
increased respiratory rate (>20 breaths per minute or PaCO2 < 32 mm Hg)
 increased or decreased white blood count (<4,000 or >12,000)
increased or decreased white blood count (<4,000 or >12,000)

B codes (b00-b99)
Neoplasms

![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Chapter-specific guidelines (ICD-10-CM chapters 1-10)












 Exercise 4-1
Exercise 4-1


 EXERCISE 4-2
EXERCISE 4-2
Get Clinical Tree app for offline access
