Chapter 7 Change and Adaptation in Pregnancy
Physiological changes in the reproductive system
The body of the uterus
Decidua


Myometrium
Uterine growth is due to hyperplasia (increase in number due to division) and hypertrophy (increase in size) of myometrial cells under the influence of oestrogen (Table 7.1). The dimensions of the uterus vary considerably, however, depending on the age and parity of the woman.
Table 7.1 Uterine growth during pregnancy
| Prior to pregnancy | At term | |
|---|---|---|
| Weight of uterus | 60–80 g | 1000 g |
| Size of uterus | 7.5 × 5 × 2.5 cm | 30 × 22.5 × 20 cm |
The three layers of the myometrium become more clearly defined during pregnancy.
Muscle layers



Uterine activity in pregnancy
 The contractile ability of the myometrium is dependent on the interaction between two contractile proteins, actin and myosin.
The contractile ability of the myometrium is dependent on the interaction between two contractile proteins, actin and myosin.


 The formation of gap junctions is promoted by oestrogens and prostaglandins.
The formation of gap junctions is promoted by oestrogens and prostaglandins.

In the last few weeks of pregnancy, prelabour occurs:



Perimetrium



Changes in uterine shape and size
For the first few weeks the uterus maintains its original pear shape, but as pregnancy advances the corpus and fundus assume a more globular form (Box 7.1).
Box 7.1 Changes in the pregnant uterus
12 weeks
• The uterus is about the size of a grapefruit
• It is no longer anteverted and anteflexed and has risen out of the pelvis and become upright
• The fundus may be palpated abdominally above the symphysis pubis
• The globular upper segment is sitting on an elongated stalk formed from the isthmus, which softens and which will treble in length from 7 to 25 mm between the 12th and 36th weeks
38 weeks
• The uterus reaches the level of the xiphisternum
• As the upper segment muscle contractions increase in frequency and strength, the lower uterine segment develops more rapidly and is stretched radially; along with cervical effacement and softening of the tissues of the pelvic floor, this permits the fetal presentation to begin its descent into the upper pelvis
• This leads to a reduction in fundal height known as lightening, relieving pressure on the upper part of the abdomen but increasing pressure in the pelvis. In the majority of multiparous women, however, engagement rarely occurs prior to labour
The cervix




Changes in the cardiovascular system
The heart





Cardiac output
 The increase in cardiac output ranges from 35 to 50% in pregnancy, from an average of 5 L/min before pregnancy to approximately 7 L/min by the 20th week; thereafter the changes are less dramatic.
The increase in cardiac output ranges from 35 to 50% in pregnancy, from an average of 5 L/min before pregnancy to approximately 7 L/min by the 20th week; thereafter the changes are less dramatic.
 The increased cardiac output is due to rises in both stroke volume and heart rate.
The increased cardiac output is due to rises in both stroke volume and heart rate.

 Heart rates are typically 10–15 beats per minute faster than those of the non-pregnant woman.
Heart rates are typically 10–15 beats per minute faster than those of the non-pregnant woman.

Blood
Blood pressure
 Early pregnancy is associated with a marked decrease in diastolic blood pressure but little change in systolic pressure. With reduced peripheral vascular resistance the systolic blood pressure falls an average of 5–10 mmHg below baseline levels and the diastolic pressure falls 10–15 mmHg by 24 weeks’ gestation.
Early pregnancy is associated with a marked decrease in diastolic blood pressure but little change in systolic pressure. With reduced peripheral vascular resistance the systolic blood pressure falls an average of 5–10 mmHg below baseline levels and the diastolic pressure falls 10–15 mmHg by 24 weeks’ gestation.


Blood volume
The total maternal blood volume increases 30–50% in singleton pregnancies.
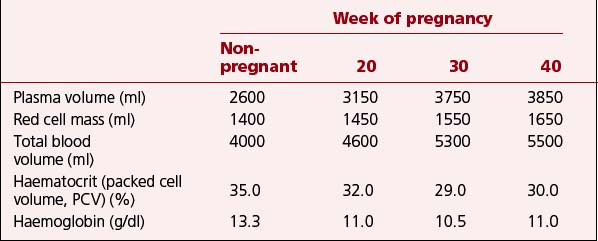
Red cell mass increases during pregnancy in response to the extra oxygen requirements of maternal and placental tissue. Approximately 10–15% of women will have an increase in and reactivation of maternal fetal haemoglobin. The increase in red cell mass appears to be constant throughout pregnancy but it is most marked from about 20 weeks. In spite of the increased production of red blood cells, the marked increase in plasma volume causes dilution of many circulating factors. As a result, the red cell count, haematocrit and haemoglobin concentration all decrease (Table 7.2).
Table 7.2 Falling haemoglobin and haematocrit in pregnancy despite rising blood volume and red cell mass
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


