2 Caring for the patient with respiratory problems
ANATOMY AT A GLANCE
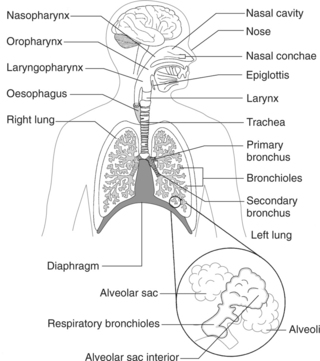
The basic structure of the respiratory system is summarized for you in Figure 2.1. Refer to this diagram whilst reading about the physiology in the next section.
PHYSIOLOGY YOU NEED TO KNOW
 Pulmonary ventilation is the movement of air into and out of the lungs. It is carried out by increasing the volume of the thorax on inspiration thereby reducing pressure within the lungs to less than atmospheric. At rest this is accomplished by the diaphragm being lowered 1 cm which is sufficient to pull in some 500 mL of air. Exercise requires greater volumes of air to be inhaled. Contraction of the external intercostal and shoulder muscles further increases the volume of the thorax as the chest wall moves upwards and outwards, reducing pressure further and drawing larger volumes of air into the lungs. Expiration is a passive process of elastic recoil aided by the action of the internal intercostal muscles pulling the chest wall inwards during exertion.
Pulmonary ventilation is the movement of air into and out of the lungs. It is carried out by increasing the volume of the thorax on inspiration thereby reducing pressure within the lungs to less than atmospheric. At rest this is accomplished by the diaphragm being lowered 1 cm which is sufficient to pull in some 500 mL of air. Exercise requires greater volumes of air to be inhaled. Contraction of the external intercostal and shoulder muscles further increases the volume of the thorax as the chest wall moves upwards and outwards, reducing pressure further and drawing larger volumes of air into the lungs. Expiration is a passive process of elastic recoil aided by the action of the internal intercostal muscles pulling the chest wall inwards during exertion. External respiration is the gas exchange taking place within the alveoli. Oxygen diffuses across the very thin respiratory membrane of each alveolus from atmospheric air into the pulmonary capillaries. Carbon dioxide moves in the opposite direction. Both gases move down their partial pressure gradients.
External respiration is the gas exchange taking place within the alveoli. Oxygen diffuses across the very thin respiratory membrane of each alveolus from atmospheric air into the pulmonary capillaries. Carbon dioxide moves in the opposite direction. Both gases move down their partial pressure gradients. Internal respiration. This term describes the movement of gases between the capillaries of the systemic circulation and tissue cells. This occurs by diffusion down partial pressure gradients with O2 entering cells and CO2 entering the capillaries.
Internal respiration. This term describes the movement of gases between the capillaries of the systemic circulation and tissue cells. This occurs by diffusion down partial pressure gradients with O2 entering cells and CO2 entering the capillaries.



CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) (P337)
PATHOLOGY: Key facts
 COPD is a term that covers several different diseases such as chronic bronchitis, emphysema and bronchiectasis. Patients are usually elderly and have a history of smoking for many years which has greatly contributed to the disease process. As the term COPD implies, the person is suffering from a slowly progressive airway obstruction which leads to a gradual deterioration in ventilation and gas exchange such that the person can no longer meet their body requirements for oxygen. Gradually respiratory failure develops.
COPD is a term that covers several different diseases such as chronic bronchitis, emphysema and bronchiectasis. Patients are usually elderly and have a history of smoking for many years which has greatly contributed to the disease process. As the term COPD implies, the person is suffering from a slowly progressive airway obstruction which leads to a gradual deterioration in ventilation and gas exchange such that the person can no longer meet their body requirements for oxygen. Gradually respiratory failure develops.

 Bronchiectasis is a term used to describe abnormal dilation of the bronchi. In adults it is frequently caused by the accumulation of pus beyond a lesion which is obstructing a bronchus such as a bronchial carcinoma. It is seen in people with cystic fibrosis as a result of the accumulation of thick mucus and recurrent infections and may also be secondary to serious lung diseases such as suppurative pneumonia or pulmonary tuberculosis. Chronic inflammatory changes occur together with the accumulation of pus within the cavities that form leading to coughing, copious production of purulent sputum and a general deterioration in the patient’s condition.
Bronchiectasis is a term used to describe abnormal dilation of the bronchi. In adults it is frequently caused by the accumulation of pus beyond a lesion which is obstructing a bronchus such as a bronchial carcinoma. It is seen in people with cystic fibrosis as a result of the accumulation of thick mucus and recurrent infections and may also be secondary to serious lung diseases such as suppurative pneumonia or pulmonary tuberculosis. Chronic inflammatory changes occur together with the accumulation of pus within the cavities that form leading to coughing, copious production of purulent sputum and a general deterioration in the patient’s condition.WHAT TO LOOK OUT FOR
 Respiratory failure, therefore respiratory rate and depth should be carefully monitored along with other vital signs.
Respiratory failure, therefore respiratory rate and depth should be carefully monitored along with other vital signs.






PHARMACOLOGY FOCUS
Short-acting β2 agonists such as salbutamol and terbutaline are helpful for symptom relief. If symptoms are persistent in more serious cases then an antimuscarinic bronchodilator such as ipratropium will be used. This group of drugs are considered more effective in treating COPD than asthma. Antimicrobial therapy is discussed elsewhere, but generally amoxicillin is prescribed for exacerbations of chronic bronchitis.
PRIORITIES FOR NURSING CARE
 Respiratory support involves helping the patient with an acute episode of breathlessness by positioning (sitting upright to maximize chest expansion) and coaching the patient in slower deeper respirations whilst providing psychological support. Close cooperation with the physiotherapist is essential to help with breathing exercises and pulmonary rehabilitation. Always check that oxygen cannulae are in place and are delivering the required flow rate.
Respiratory support involves helping the patient with an acute episode of breathlessness by positioning (sitting upright to maximize chest expansion) and coaching the patient in slower deeper respirations whilst providing psychological support. Close cooperation with the physiotherapist is essential to help with breathing exercises and pulmonary rehabilitation. Always check that oxygen cannulae are in place and are delivering the required flow rate.Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


