7 Caring for the patient with a disorder of the urinary system
ANATOMY AT A GLANCE
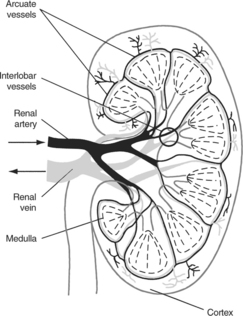
Each kidney consists of a fatty capsule containing the medulla and cortex, which collectively is known as the renal parenchyma (see Figure 7.1). The medulla is divided up into a series of subunits known as the renal pyramids (between 8 and 18 per kidney). The functional units of the kidneys are the nephrons, which are contained within the medulla and cortex, totalling approximately one million per kidney.
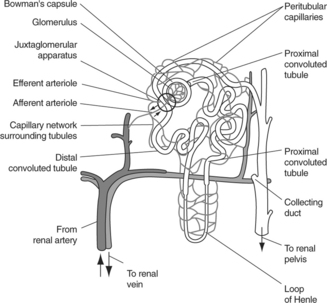
 Blood supply: as can be seen from Figure 7.2, each nephron is supplied with blood via an afferent arteriole, which divides into a tangled web of capillaries called the glomerulus before reuniting to form an efferent arteriole that is narrower than the original afferent arteriole. The efferent arteriole then subdivides into a network of peritubular capillaries, which surrounds the tubule before reuniting to form the peritubular venules which feed into the renal vein.
Blood supply: as can be seen from Figure 7.2, each nephron is supplied with blood via an afferent arteriole, which divides into a tangled web of capillaries called the glomerulus before reuniting to form an efferent arteriole that is narrower than the original afferent arteriole. The efferent arteriole then subdivides into a network of peritubular capillaries, which surrounds the tubule before reuniting to form the peritubular venules which feed into the renal vein.



PHYSIOLOGY YOU NEED TO KNOW
As adults we are 55% (women) to 60% (men) water. Some 66% of that water resides within cells and is known as intracellular fluid; the rest is extracellular fluid divided between plasma and interstitial fluid in a ratio of about 1 : 4. We excrete an average of 1500 mL of urine per day, but also lose some 600 mL of water in evaporation from the skin, 300 mL in breathing out and a further 100 mL in faecal matter. Fluid intake therefore needs to be around 2500 mL per day to achieve fluid balance.
The functions of the renal system may be summarized as follows:
 To regulate fluid and electrolyte balance within the body. This ensures that
To regulate fluid and electrolyte balance within the body. This ensures that



 Filtration: occurs in the glomerulus, the narrower diameter efferent arteriole helps generate filtration pressure within the glomerulus as does overall blood pressure. Filtration rate depends largely on the rate of supply of blood to the kidneys via the renal arteries. Average rate is 105–125 mL/min.
Filtration: occurs in the glomerulus, the narrower diameter efferent arteriole helps generate filtration pressure within the glomerulus as does overall blood pressure. Filtration rate depends largely on the rate of supply of blood to the kidneys via the renal arteries. Average rate is 105–125 mL/min. Reabsorption: this occurs as molecules move from the filtrate through the wall of the tubule into the interstitial fluid, and finally into the network of tubular blood vessels. The proximal convoluted tubule sees the reabsorption of large quantities of glucose, sodium, potassium, chloride and water, to name but a few substances. Lesser amounts of water, sodium, potassium and chloride are absorbed in the loop of Henle and further small amounts of water, sodium and chloride in the distal convoluted tubule.
Reabsorption: this occurs as molecules move from the filtrate through the wall of the tubule into the interstitial fluid, and finally into the network of tubular blood vessels. The proximal convoluted tubule sees the reabsorption of large quantities of glucose, sodium, potassium, chloride and water, to name but a few substances. Lesser amounts of water, sodium, potassium and chloride are absorbed in the loop of Henle and further small amounts of water, sodium and chloride in the distal convoluted tubule.

URINARY TRACT INFECTION (P641)
PATHOLOGY: Key facts
Infection and inflammation of the urethra is called urethritis, and when the bladder is involved, cystitis. Approximately, 20% of women will experience at least one episode of urinary tract infection (UTI). This high incidence is thought to be due to the short female urethra (4 cm) making the entry of organisms from the rectum (e.g. Escherichia coli) and vagina much easier. Poor toilet hygiene and sexual activity increase the risk of infection, as does the presence of an indwelling urinary catheter or compression of the bladder by the uterus during pregnancy. UTI is much rarer in men, although men aged over 65 developing urinary obstructive problems due to an enlarged prostate are prone to UTI.
PRIORITIES FOR NURSING CARE
The focus is on preventing UTI:

 Patient education about personal hygiene associated with defecation (wipe from front to rear and wash hands thoroughly) and sex (both partners should wash their hands and genitals thoroughly before sex and, if problems persist, use condoms).
Patient education about personal hygiene associated with defecation (wipe from front to rear and wash hands thoroughly) and sex (both partners should wash their hands and genitals thoroughly before sex and, if problems persist, use condoms).
If the patient has an indwelling catheter:




There is no evidence to support the use of:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


