4 Caring for the patient with a disorder of the gastrointestinal system
ANATOMY AT A GLANCE
The main structures of the gut are shown in Figure 4.1.
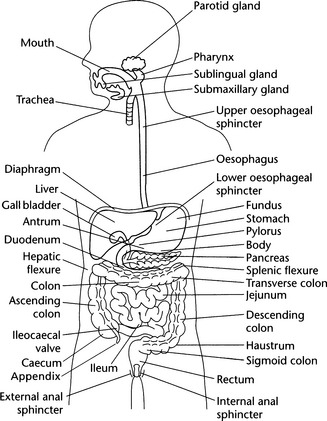
 The inner layer is the mucosa which in the stomach and small intestine contains specialized cells with secretory or absorptive functions.
The inner layer is the mucosa which in the stomach and small intestine contains specialized cells with secretory or absorptive functions.


The gut terminates with the internal anal sphincter which connects the rectum to the anus (under involuntary control) and the external anal sphincter which connects the anus to the outside (under voluntary control).
PHYSIOLOGY YOU NEED TO KNOW
The Stomach
Food is passed from the mouth via the oesophagus to the stomach where digestion begins. Ingested food and gastric secretions form a semi-liquid substance known as chyme which is continually churned and mixed by regular waves of muscle contraction in the stomach wall (peristalsis). The stomach mucosa contains many small gastric pits which are lined by:
 Chief cells which secrete pepsinogen. This is converted to pepsin when it comes into contact with hydrochloric acid. Pepsin is a powerful enzyme which breaks down proteins.
Chief cells which secrete pepsinogen. This is converted to pepsin when it comes into contact with hydrochloric acid. Pepsin is a powerful enzyme which breaks down proteins.

The Colon
The large intestine (colon) is predominantly the site of water and electrolyte absorption. A great deal of bacterial activity takes place in the colon but these bacteria are normally not pathogenic and help the body by synthesizing useful substances such as vitamin K (essential for the manufacture of prothrombin), folic acid and thiamine. Large quantities of mucus are also produced in the colon. Irritation of the colon wall increases mucus output and also causes the outpouring of water and electrolytes in an attempt to dilute and wash away the irritant. The result is diarrhoea.
NEOPLASTIC DISEASE
PATHOLOGY: Key facts
 Oesophageal cancer (p440) is increasing in frequency. It is more common in men, typically aged 50–70 and most commonly occurs in the lower third. The ability to swallow is progressively impaired and the growth spreads to involve surrounding organs such as the trachea, bronchi and stomach. The prognosis is poor with few patients surviving more than a year from diagnosis.
Oesophageal cancer (p440) is increasing in frequency. It is more common in men, typically aged 50–70 and most commonly occurs in the lower third. The ability to swallow is progressively impaired and the growth spreads to involve surrounding organs such as the trachea, bronchi and stomach. The prognosis is poor with few patients surviving more than a year from diagnosis.
 Bowel cancer (p477) most frequently occurs in the rectum. The sigmoid colon, caecum and ascending colon are the next most common sites. Cancers of the small bowel are very rare. Cancer of the colon is multifactorial in cause. A high-fat diet rich in red meat but poor in fruit and vegetables and lack of exercise are associated with an increased risk whilst some 20% of colorectal cancers have a genetic cause (e.g. familial polyposis) or a familial predisposition.
Bowel cancer (p477) most frequently occurs in the rectum. The sigmoid colon, caecum and ascending colon are the next most common sites. Cancers of the small bowel are very rare. Cancer of the colon is multifactorial in cause. A high-fat diet rich in red meat but poor in fruit and vegetables and lack of exercise are associated with an increased risk whilst some 20% of colorectal cancers have a genetic cause (e.g. familial polyposis) or a familial predisposition.WHAT TO LOOK OUT FOR
 Oesophageal cancer Difficulty in swallowing (dysphagia) solids occurs first followed by problems with swallowing liquids. Discomfort and pain in the sub-sternal region may be accompanied by regurgitation. Loss of weight and strength develop as the person’s food intake diminishes.
Oesophageal cancer Difficulty in swallowing (dysphagia) solids occurs first followed by problems with swallowing liquids. Discomfort and pain in the sub-sternal region may be accompanied by regurgitation. Loss of weight and strength develop as the person’s food intake diminishes.

MEDICAL MANAGEMENT
Stomach cancer is diagnosed after endoscopy and biopsy, barium meal radiography and cytological studies of gastric juice. Computerized tomography may also be ordered to investigate the size and spread of the tumour in the abdomen and thorax. Surgery is the treatment of choice, the exact nature of the operation depending upon the tumour and its development. The lower oesophagus, omentum, spleen, pancreas or sections of the duodenum may also be involved in the surgery, depending upon the spread of the tumour. Radiotherapy and chemotherapy have so far not made any significant contribution to treatment of this cancer.
PRIORITIES FOR NURSING CARE
 Oesophageal cancer patients need:
Oesophageal cancer patients need:Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


