A comprehensive geriatric evaluation (CGE) is essential to fully understand the health needs of older adults. The CGE is performed by a multidisciplinary team, which typically includes a geriatric nurse, geriatric physician, and social worker. Other members of the team may include a pharmacist, physical therapist, and dietitian. The Hartford Institute for Geriatric Nursing provides many tools for assessment of older adults on their Web site (www. consultgerirn. org/resources).
Normal Changes of Aging
There are a number of normal age-related changes that occur in all major systems of the body. These may present at different times for different people. It is important to be able to differentiate between normal and abnormal changes in older adults and to educate patients and families about these differences.
Presbyopia (farsightedness) due to decreased visual accommodation from loss of lens elasticity.
Decreased color discrimination due to the yellowing of the lens; short wavelength colors, such as blues and greens, are more difficult to see.
Increased sensitivity to glare.
Decreased depth perception.
Decreased tear production.
Assessment Findings
Arcus senilis—deposits of lipid around the eye, seen as a white circle around the iris; causes no vision impairments.
Cataracts—clouding of the normally clear lens of the eye. (This results in lens thickening and decreased permeability; noted on examination with an ophthalmoscope; fuzziness of vision, like looking through wax paper. Cataracts cause blurring, sensitivity to light, and/or double vision.)
Macular degeneration—due to damage to macula that results in loss of central vision. (Objects seem blurred, distorted, or are not seen.)
Glaucoma—increased intraocular pressure with tonometer testing. (Results in blurring, colored “halos” around lights, pain or redness of eyes, loss of peripheral vision.)
Smaller pupil size.
Complaints of decreased ability to read, discomfort from light, changes in depth perception, falls, collisions, difficulty handling small objects, difficulty with activities of daily living (ADLs), and tunnel vision.
Dry, red eyes.
Vitreous floaters, which are lightning flashes in the visual field.
Nursing Considerations and Teaching Points
Make sure objects are in the patient’s visual field, and do not move objects around.
Use large lettering to label medications and any distributed written information.
Allow the person more time to focus and adjust to the environment.
Avoid glare—may help to wear sunglasses.
Use nightlights to help with dark adaptation problems.
Use red and yellow to stimulate vision.
Mark the edges of stairs and curbs to help with depth perception problems.
Use microspiral telescopes or magnifying glasses and highintensity lighting.
Encourage yearly eye examination and/or refer for examination if vision changes worsen (flashing lights in fields or “veil over the eye”).
Encourage use of isotonic eyedrops as needed for dry eyes.
Encourage use of low vision aids, such as magnifying lens, light filtering lens, telescopic lenses, or electronic devices.
Refer patients to the following resources for vision impairments:
Prevent Blindness America 800-331-2020
www.preventblindness.org
American Foundation for the Blind 800-232-5463
www.afb.org
American Council of the Blind 800-242-8666
www.acb.org
National Institutes of Health Low Vision & Blindness Educational Resources
http://health.nih.gov/topic/LowVisionBlindness
Hearing
Characteristics
Approximately 30% to 50% of people older than age 65 have significant hearing loss.
Two major types of hearing disorders are common in the older population.
Sensorineural—progressive, irreversible bilateral loss of high-tone perception often associated with aging. This results in difficulty with discriminating sounds. Sound waves reach the inner ear but are not properly transmitted to the brain.
Conduction deafness—results from blockage or impairment of the mechanical movement in the outer or middle ear (also a pathologic condition). Sound waves are not conducted to the inner ear, resulting in sounds that are muffled.
Hearing loss in older adults is usually a combined problem. The majority of the loss is due to auditory nerve changes or deterioration of the structures of the ear. There may also be nerve damage beyond the ear. Presbycusis and central deafness can result in permanent hearing loss; conduction deafness is reversible.
Usual progression from high-tone or high-frequency loss to a general loss of both high and low tones.
Consonants (higher-pitched sounds) are not heard well.
Hearing loss increases with age and is greater in men.
Increase in the sound threshold (ie, greater sound needed to stimulate the older adult).
Decreased speech discrimination, especially with background noise.
Cerumen impaction, the most common cause of conductive hearing loss, is reversible.
Assessment Findings
Increased volume of patient’s own speech.
Turning of head toward speaker.
Requests of a speaker to repeat.
Inappropriate answers, but otherwise cognitively intact.
The person may withdraw, demonstrate a short attention span, and become frustrated, angry, and depressed.
Lack of response to a loud noise.
Nursing Considerations and Teaching Points
Be aware that hearing loss can impact the safety and quality of life for older adults in many ways. For example, the older adult may not hear instructions, alerting signals, telephones, or oncoming traffic. Hearing loss can contribute to social isolation and lower self-esteem.
Suggest hearing testing with an audiologist for further evaluation and consideration of an assistive device.
Face the person directly so he can lip-read.
Use gestures and objects to help with verbal communication. 5 Touch the person to get his or her attention before talking.
Speak into the patient’s “good ear.”
Do not shout. Shouting increases the tone of the voice, and older adults are unable to hear these high tones. Try speaking in a deeper or lower tone of voice.
Speak slowly and clearly.
Suggest amplifiers on telephones and alarms.
Allow the person more time to answer your questions.
Evaluate the person’s ear canals regularly and assist with cerumen removal. Cerumen removal is facilitated by:
Use of ceruminolytic agents, such as carbamide peroxide, 10 drops in the affected ear twice per day for 5 days, followed by flushing the ear with warm water via a 50-mL irrigation syringe or an electronic irrigation device.
Careful use of an ear spoon to mechanically remove cerumen.
Refer patients to the following organizations:
American Speech—Language—Hearing Association: www.αshα.org
HearingLoss.com: www.hearingloss.com
National Institute on Deafness and Other Communication Disorders: www.nidcd.nih.gov/health/hearing/pages/older.aspx
Smell
Characteristics
Changes in smell (olfaction) are due to nasal sinus disease preventing odors from reaching smell receptors, a decrease in nerve fibers, chronic injury from infections, or bleeding.
Discrimination of fruity odors seems to persist the longest.
Generally, olfaction decreases in men more than in women.
Assessment Findings
Inability to notice unpleasant odors, such as fire, body odor, or excessive perfume.
Decreased appetite.
Nursing Considerations and Teaching Points
Age-related changes can impact safety and quality of life. For example, an older individual may not be able to recognize the smell of smoke or gas.
The inability to smell food may cause a decrease in the consumption of nutritious food.
At mealtimes, name food items and give the person time to think of the smell/taste of the food.
Suggest use of stronger spices and flavorings to stimulate sense of smell.
Taste
Characteristics
Taste buds decrease with age, especially in men. People over age 60 have lost half of their taste buds. By age 80, only one sixth of the taste buds remain.
Taste buds are lost from the front to the back (ie, sweet and salty tastes are lost first, whereas bitter and sour tastes remain longer).
Assessment Findings
Complaints that food has no taste.
Excessive use of sugar and salt.
Inability to identify foods.
Decrease in appetite and weight loss.
Decreased pleasure from food.
Nursing Considerations and Teaching Points
Age-related changes can impact safety. For example, the older individual may not be able to detect spoiled food.
Serve food attractively, and separate different types of foods.
Vary the texture of foods.
Encourage good oral hygiene.
Season food.
Kinesthetic Sense
Characteristics
With age, the receptors in the joints and muscles that tell us where we are in space lose their ability to function. Therefore, there is a change in balance.
Walking with shorter step length, less leg lift, a wider base, and a tendency to lean forward.
With age, less ability to stop a fall from occurring.
Assessment Findings
Alterations in posture, ability to transfer, and gait
Complaint of dizziness
Nursing Considerations and Teaching Points
Position items within reach.
Give person more time to move.
Take precautions to prevent falls.
Suggest physical therapy with balance training after periods of prolonged immobility.
Cardiovascular
Characteristics
With age, the valves of the heart become thick and rigid as a result of sclerosis and fibrosis, compounding any cardiac disease already present.
Blood vessels also become thick and rigid, resulting in elevated blood pressure, which is present in half of the U.S. population over age 65.
Maximum heart rate and aerobic capacity decrease with age.
Slower response to stress. Once the pulse rate is elevated, it takes longer to return to baseline.
Decline in maximum oxygen consumption.
About 50% of older adults have an abnormal resting electrocardiogram.
Subtle changes in artery walls result in a less flexible vasculature.
Decreased baroreceptor sensitivity.
Assessment Findings
Normal blood pressure (BP) is less than 120/80 mm Hg; prehypertension, 120 to 139/80 to 89; stage 1 hypertension, 140 to 159/90 to 99; stage 2 hypertension, 160/100 mm Hg and greater.
Prolonged tachycardia may occur following stress.
Nursing Considerations and Teaching Points
Encourage regular BP evaluation as well as lifestyle modifications and medication adherence, if indicated, for hypertension.
Check for postural BP changes to detect orthostatic hypotension and prevent falls. Instruct patients to rise slowly from lying to sitting to standing.
Encourage longer cool-down period after exercise to return to baseline cardiac function.
Encourage moderate physical activity: walking, biking, or swimming for 30 minutes five times per week (150 minutes per week), in addition to muscle strengthening exercises two times a week.
Pulmonary
Characteristics
With age, there is a weakening of the intercostal respiratory muscles, and the elastic recoil of the chest wall diminishes.
There is no change in total lung capacity; however, residual volume and functional residual capacity increase.
Partial pressure of oxygen decreases with age due to ventilation—perfusion mismatches. However, older adults are not hypoxic without coexistent disease.
There is a decrease in the mucus transport/ciliary system. Therefore, there is decreased clearance of mucus and foreign bodies, including bacteria.
Assessment Findings
Prolonged cough, inability to raise secretions.
Increased frequency of respiratory infections.
Nursing Considerations and Teaching Points
Older adults who are undergoing surgical treatment should engage in deep-breathing exercises.
Teach measures to prevent pulmonary infections—avoid crowds during cold and flu season, wash hands frequently, report early signs of infection.
Avoid smoking and exposure to secondhand smoke.
Encourage annual flu vaccine and pneumonia vaccine at age 65 or as needed.
Immunologic
Characteristics
The function of T-cell lymphocytes, such as cell-mediated immunity, declines with age due to involution and atrophy of the thymus gland.
Declining B-cell function as a result of T-cell changes.
Assessment Findings
More frequent infections.
Increased incidence of many types of cancer.
Nursing Considerations and Teaching Points
Teach older adults that they are at increased risk of infection, cancer, and autoimmune disease; therefore, routine follow-up and screening are essential.
Encourage healthy lifestyle practices to maintain optimal health.
Neurologic
Characteristics
There is gradual loss in the number of neurons with age, but no major change in neurotransmitter levels.
Some brain tissue atrophy is normal and does not relate to cognitive impairment.
Decrease in muscle tone, motor speed, and nerve conduction velocity.
Decrease in gait speed of 1.6% per year after age 63; decreased step length, stride length, and arm swing.
Assessment Findings
Decreased position and vibration sense.
Diminished reflexes, possible absent ankle jerks.
Complaint of falls and impaired balance.
Wide-based gait with decreased arm swing.
Nursing Considerations and Teaching Points
Because of these changes in combination with sensory changes, it is essential to teach older adults fall-prevention techniques.
Environmental safety techniques include nonslip surfaces, securely fastened handrails, sufficient light, glare-free lights, avoidance of low-lying objects, chairs of the proper height with armrests, skidproof strips or mats in the tub or shower, toilet and tub grab bars, elevated toilet seats.
Home safety evaluations should be done on all communitydwelling older adults to reduce the risk of falls. A home safety checklist can be obtained from the National Safety Council at www.nsc.org.
Musculoskeletal
Characteristics
Declining muscle mass and endurance with age, although deconditioning may be an associated factor.
Decreased bone density, less so in men than in women.
Decreased thickness and resiliency of cartilage, with a resulting increase in the stiffness of joints.
Bone resorption exceeds bone formation, resulting in a decline in bone density.
Injuries to the cartilage accumulate with age.
Assessment Findings
Muscle atrophy.
Increased incidence of fractures.
Complaint of joint stiffness in absence of arthritis.
Decreased bone density (less than 2.5 standard deviations below normal).
Nursing Considerations and Teaching Points
Early intervention to encourage regular exercise (including weight-bearing exercise and resistance training) in older adults is important to prevent exacerbation of these normal changes.
Encourage increased intake of calcium and vitamin D and decreased alcohol and nicotine use.
Community and Home Care Considerations
Encourage older adults to engage in 30 minutes of moderate physical activity, including walking, biking, or swimming, at least five times per week, in addition to muscle strengthening exercises at least two times a week.
For older adults who will be exercising at less than 80% of the maximum heart rate (220 — age), stress testing before starting an exercise program is not needed.
To help with adherence to the exercise program, older adults should be encouraged to exercise at a set time, to relieve pain before exercising, and to do an activity they enjoy. Provide positive reinforcement for those who do exercise, and continually reinforce the benefits of exercise (increased bone strength, cardiovascular fitness, decreased risks of falls, overall sense of well-being).
Endocrine
Characteristics
Decreased secretion of trophic hormones from the pituitary gland.
Blunted growth hormone release during stress.
Elevated vasopressin (antidiuretic hormone); exaggerated response to osmotic challenge.
Elevated levels of follicle-stimulating hormone and luteinizing hormone because of reduced end-organ response.
Decreased insulin secretion after meals; this may be a function of weight or genetic factors.
Assessment Findings
Usually asymptomatic.
Nursing Considerations and Teaching Points
Encourage routine screening for elevated blood glucose— both fasting and postprandial.
Provide education about a well-balanced diet.
Reproductive
Characteristics
In women, menopause leads to decreases in the size of the ovaries and hormone production. This results in uterine involution, vaginal atrophy, and loss of breast mass.
With age, there is increased risk in females of cystocele, rectocele, and uterine prolapse.
In men, testosterone production and secretion decrease with age. However, serum levels may be in the low-normal range through age 80.
Assessment Findings
Vaginal dryness, painful intercourse.
Atrophic vaginitis.
Urinary incontinence.
Nursing Considerations and Teaching Points
Suggest the use of additional lubrication during sexual intercourse.
Advise sexually active older men that spermatogenesis may continue into advanced age.
Address risks and benefits of time-limited hormone replacement therapy for symptomatic relief related to menopause.
Renal and Body Composition
Characteristics
Increased body fat and decreased lean muscle mass, even when weight remains stable.
Decreased renal function, measured by the glomerular filtration rate, or creatinine clearance.
Despite reduced total body creatinine due to decreased muscle mass in the older adult, serum creatinine often remains within normal range. This is because of decreased elimination of creatinine by the kidneys.
About 10% decline in creatinine clearance per decade after age 40; however, relatively unchanged serum creatinine.
Assessment Findings
Usually asymptomatic.
Increased incidence of anemia.
Nursing Considerations and Teaching Points
Be aware that although serum creatinine may be within normal range, creatinine clearance may be decreased. To obtain an accurate creatinine clearance in an older adult, the following formula may be used: (140 — age)(weight [kg])/(72) (serum creatinine [mg/dL]).
Drugs that are cleared through the kidneys may be given in decreased dosage. Adverse effects and toxicity must be closely monitored.
Consider the advantages and disadvantages of drug management for anemia associated with renal disease.
Skin
Characteristics
Thinning of all three layers of the skin—epidermis, dermis, and subcutaneous tissue—leads to greater fragility of the skin and decreased ability of the skin to function as a barrier to external factors.
Fewer melanocytes and decreased tanning.
Less efficient thermoregulation of heat because of fewer sweat glands.
Drier skin because the decreased number of sebaceous glands results in reduced oil production.
Other changes in aging skin include reduced sensory input, decreased elasticity, and impaired cell-related immune response.
Assessment Finding
Dry, irritated skin.
Nursing Considerations and Teaching Points
Excessive use of soap, which can be drying to the skin, should be avoided.
Careful skin evaluation and lubrication are necessary to prevent fissures and breakdown.
Heat regulation needs to be controlled by proper clothing and avoidance of extreme temperatures.
Avoid direct application of extreme hot or cold to skin because damage may occur without feeling it.
Encourage use of sunscreen during all outdoor activities.
Community and Home Care Considerations
Xerosis (dry skin) is a common problem for older adults. Treatment should include:
Drinking 2,000 mL of liquid daily.
Total body immersion in warm water (90° to 105° F [32.2° to 40.6° C]) for 10 minutes.
Use of nonperfumed soap without hexachlorophene.
Application of emollient, particularly those with alphahydroxy acids, after bathing and at bedtime.
Hematopoietic
Characteristics
Unchanged number of stem cells of all three cell lines; however, bone marrow cellularity is decreased by 33% during adult life.
Declining marrow activity, especially in response to stress, such as with blood loss or infection.
Assessment Finding
Asymptomatic
Nursing Considerations and Teaching Points
Anemia and granulocytopenia are not normal consequences of aging and should be investigated.
Teach patients that there is no need to take oral iron unless there is an actual documented decrease in iron levels.
Encourage oral B12 and folate replacement to manage associated anemias.
Altered Presentation of Disease
Characteristics
In part due to the physiologic changes that occur with aging, the manifestations of illness in the older patient are less dramatic than in younger patients.
Most older adults have at least one chronic condition. These coexisting conditions can complicate the evaluation of new symptoms.
Some risk factors make it more likely that they will present with an altered presentation of disease: over age 85, multiple comorbid conditions, taking over five medications, and having cognitive or functional impairment.
Evidence Base
Samaras, N., Chevalley, T., Samaras, D., et al. (2010). Older patients in the emergency department: a review. Annals of emergency medicine, 56(3), 261-269.
Assessment Findings
The classic indicators of disease are usually absent or disorders present atypically (see Table 9-1).
Older people are less likely to report new symptoms but, rather, attribute them to aging or existing conditions. Many older adults minimize symptoms because of fears of hospitalization or health care costs.
Table 9-1 Atypical Presentation of Disorders in the Older Adult
DISORDER
ATYPICAL PRESENTATION
Acute intestinal infection
• Abdominal pain may be absent.
•May present with acute confusional state, leukocytosis, and acidosis.
Appendicitis
•Pain may be diffuse, not localized in right lower quadrant.
Biliary disease
•Confusion, declining function, and other nonspecific symptoms.
•Abnormal liver function tests may be only sign.
Heart failure
•Initially, may have change in mental status and fatigue.
Hyperthyroidism
•Apathy, palpitations, weight loss, weakness.
Hypothyroidism
•Presents with weight loss.
Myocardial infarction
•Chest pain may be absent.
•May present with syncope, dyspnea, vomiting, or confusion.
Perforated ulcer
•Rigidity may be absent until late.
Pneumonia
•May present with confusion.
•Fever and cough may be absent.
Pulmonary embolism
•May present with change in mental status.
•May not have fever, leukocytosis, or tachycardia.
Septicemia
•May be afebrile.
Systemic lupus erythematosus
•Pneumonitis, subcutaneous nodules, and discoid lesions are more common.
•Malar rash, Raynaud’s phenomenon, and nephritis are less common.
Urinary tract infection
•Confusion.
Nursing Considerations and Teaching Points
Have a high index of suspicion for underlying illness if the older adult presents with an acute change in cognition, behavior, or function.
Functional Assessment
Functional assessment is the measurement of a patient’s ability to complete functional tasks and fulfill social roles, specifically addressing a patient’s ability to complete tasks ranging from simple self-care to higher-level activities. It provides the nurse with objective data to help determine the older adult’s needs and plan interventions.
Purpose
Functional assessment is essential in the care of the older adult because it:
Offers a systematic approach to assessing older adults for deficits that commonly go undetected.
Helps the nurse to identify problems and utilize appropriate resources.
Provides a way to assess progress and decline over time.
Helps the nurse evaluate the safety of the patient’s ability to live alone.
Functional status includes the evaluation of sensory changes, ability to complete ADLs and instrumental ADLs, gait and balance problems, and elimination.
Instruments to Measure Functional Ability
Functional status may be assessed by several methods: self-report, direct observation, or family report. Direct observation is the method of choice, when possible.
The instrument chosen should be based on the specific goal or purpose for the evaluation. For example, if the focus is on basic self-care and mobility, the Barthel index should be used. See references, page 195 (Mahoney & Barthel).
The Katz Index for Activities of Daily Living and Instrumental Activities of Daily Living is another rating scale for measuring functional ability. Use this scale to determine level of independence of the older adult and repeat periodically to compare level of functioning over time. See references, page 195.
Performance measures, such as the Tinetti Gait and Balance measure or the Chair Rise test, can be used to evaluate higher-level functioning.
Psychosocial Assessment
Altered Mental Status
Assessment of mental status to detect altered cognition involves examination of memory, perception, communication, orientation, calculation, comprehension, problem solving, thought processes, language, visual—spatial abilities, abstraction, attention, aphasia, and apraxia.
Assessment can be facilitated by use of cognitive screening tools. A commonly utilized instrument is the Mini-Mental State Examination (MMSE), a 30-point cognitive screening instrument that assesses orientation to time and place, registration and recall, calculation, language skills, and visual—spatial abilities.
The total possible score is 30. A score of 24—30 suggests intact cognitive function; 20—23, mild cognitive impairment; 16—19, moderate cognitive impairment; 15 or less, severe cognitive impairment. The MMSE can help to follow the patient’s cognition over time and assess for acute and/or chronic changes.
Although success on scales such as this has been associated with language abilities, education, and socioeconomic status, this scale continues to be used as an appropriate screening tool for abnormal cognitive function.
Another cognitive screening instrument is the Mini-Cog examination, which is composed of a three-item recall and the Clock Drawing Test (CDT). The Mini-Cog can be administered under 3 minutes, does not appear to be affected by the patient’s education or language abilities, and has been successfully used to screen for dementia across a variety of clinical settings. The Mini-Cog can be administered as follows:
Tell the patient to listen carefully and remember and repeat three unrelated words.
Tell the patient to draw the face of a clock including numbers and hands to read a specific time. The CDT is considered normal if all numbers are present in the correct sequence and position and the hands display the requested time.
Ask the patient to repeat the three previously stated words.
Unsuccessful recall of all three items suggests dementia. Successful recall of all three items suggests intact cognition. An abnormal CDT with one to two errors on recall suggests dementia. A normal CDT with one to two errors on recall suggests no dementia.
Assessment of altered mental status or behavior may elicit criteria that lead to a diagnosis of dementia. It is essential to differentiate dementia from delirium (which is treatable and reversible).
Delirium is abrupt in onset and is commonly due to an underlying medical condition, such as infection, electrolyte imbalance, medication intolerance or toxicity, and cardiac decompensation. Disorientation occurs early, and the behavior is variable hour to hour. There is a clouded, altered, or changing level of consciousness, short attention span, and disturbed sleep—wake cycle. Hallucinations are common. The condition is reversible with treatment of the underlying cause.
Dementia has a gradual onset. Behavior is usually stable, and disorientation occurs late. Consciousness is not clouded, attention span is generally not reduced, and daynight reversal of sleep—wake cycles can occur rather than hour-to-hour variation. Delusions (fixed false beliefs) are more common than hallucinations.
Social Activities and Support
Social support for older adults is generally instrumental, informational, or emotional. The social environment is important with regard to recovery of acute medical problems and management of chronic illness.
Elicit information by asking such questions as:
How often do you socialize with others?
With whom do you socialize?
What type of activities do you enjoy?
Do you enjoy socializing?
Who can you call for help?
Do you know of any church or community groups you can call for help?
Emotional and Affective Status
Characteristics
Depression may occur for the first time in older age and has been related to the many changes that occur with aging:
The independence of one’s children.
The reality of retirement.
The loss of roles, income, spouse, friends, family, home, pets, functional ability, health, and ability to participate in leisure activities such as reading.
Ageist messages from society supporting and encouraging the value of youth.
Depression may also be associated with underlying illnesses, such as Parkinson’s disease and stroke, and by medications, such as antihypertensives (beta blockers), anti-arthritics, and anti-anxiety agents.
Depression is usually difficult to identify in the older adult because the presentation is different than in younger people. Obtain the following information to assess for depression:
Complaints of insomnia, weight loss, anorexia, and constipation (vegetative symptoms).
Presence of anhedonia (lack of joy in usually pleasurable activities).
Decrease in concentration, memory, and decision making (pseudodementia syndrome).
Other somatic complaints, such as decreased appetite, musculoskeletal aches and pains, chest pain, fatigue.
History of chronic illness or other health problems.
Current medications.
Evaluate depression using the Geriatric Depression Scale as a screening tool.
Suicide is sometimes associated with depression, with suicides being especially high in older white men. Assess for suicide risk.
Pain is underdetected and undertreated in older adults and may be contributing to depression. Assess pain by asking and observing the patient, and provide appropriate measures to make patient more comfortable.
Nursing and Patient Care Considerations
Treatment of depression should be given to older adults and includes drugs, psychotherapy, and, in some cases, electroconvulsive therapy.
Complement other therapeutic measures by providing opportunities to increase the patient’s self-esteem.
Encourage participation in meaningful activities.
Promote the patient’s positive self-image.
Help the patient develop a sense of mastery.
Encourage reminiscence of meaningful past events.
Help patient identify and use social supports.
For behavioral problems (agitation, combative behavior, or irritability) consider options such as aromatherapy, music therapy, pet therapy, relaxation techniques, massage, or physical activity.
Motivation in Older Adults
Characteristics
Motivation is an important variable in the older adult’s ability to recover from any disabling event and the ability to maintain his or her highest level of wellness.
Understanding individual motivational factors for engaging in health promotion activities like exercise is an approach that can improve adherence. It is possible to evaluate a patient’s motivation to comply with a given treatment plan and adopt interventions to help to improve the older adult’s motivation.
Factors that influence motivation in an older adult include:
Needs such as hunger.
Past experiences, specifically with health care providers.
Negative attitudes toward aging.
Self-efficacy expectations, or the belief in one’s ability to perform a specific activity.
Outcome expectations, or the belief that if a specific activity is performed there will be an expected outcome.
The cost of performing a specific activity in terms of time, money, pain, fatigue, or fear.
Internal factors, such as sensory changes, cognitive status, and adverse drug effects.
External factors, such as social norms (particularly if those norms conflict with treatment) and the influence of social supports.
Problems in motivation due to age-related differences include:
A shift from achievement motivation to conservative motivation.
Increasing difficulty in the establishment of rewards for older people, due to their many losses.
A tendency to see a task as being more difficult than a younger person would.
A tendency to become easily discouraged; the older adult may not initiate behavior as readily.
Greater significance placed on the meaning of a task; it must be meaningful to the older person.
Evidence that older adults do not do well on tasks if they are asked to do them rapidly, under a time limit, or in a stressful situation.
Increased importance placed on the cost of participating in an activity; fear of failing can be expressed either as increased anxiety or decreased willingness to take risks.
Increased need for older adults to get approval for their effort.
The Motivation Wheel (see Figure 9-1) can be used to evaluate motivation in the older adult.
Motivation is influenced by beliefs about physical and emotional benefits, mastery experiences, individualized care, social support, the environment, goals, physical sensations, and new activities.
Motivation can be increased by strengthening beliefs about potential benefits, providing opportunities for mastery, identifying individualized care approaches and goals, using social supports, accessing supportive environments, decreasing unpleasant sensations, and trying new activities.
Evidence Base
Quindry, J. C., Yount, D., O’Bryant, H., et al. (2011). Exercise engagement is differentially motivated by age-dependent factors. American Journal of Health Behavior, 35(3), 334-345.
Figure 9-1. The wheel that moves.
Nursing and Patient Care Considerations
Strategies to improve motivation include:
Establish whose motives are being discussed—patient’s, family’s, or health care provider’s; involve patient in setting the goals.
Explore with patient any indication of fear or other unpleasant sensation associated with the activity, such as pain or fatigue, and implement interventions to decrease these unpleasant sensations.
Evaluate the spokes of the wheel to consider the many factors that influence motivation and implement interventions as appropriate.
Encourage patient to verbally express emotional factors associated with the activity.
Examine the setting for the desired behavior to occur. Is the environment too stressful, too dark, or too noisy?
Attempt to use role models. Older adult role models can change ageist attitudes and stimulate patients to perform the desired behavior.
Set small goals to be met either daily or each shift. This provides frequent rewards.
Do not be afraid to use yourself. Research has indicated that being nice, demonstrating caring, using humor, verbal encouragement, and support can all help motivate the older adult.
Educate the older adult about the benefits of the activity, whether these are physical or psychological.
HEALTH MAINTENANCE
Evidence Base
United States Preventive Services Task Force. (2012). The guide to clinical preventive services: Recommendations of the U.S Preventive Services Task Force. Available: www.uspreventiveservices taskforce.org/index.html.
Primary Prevention
The goal of health promotion and disease prevention is to add more quality years to life. There are three levels of health promotion and disease prevention.
Primary prevention is the prevention of disease before it occurs. Primary prevention can be broken down into counseling, immunizations, and chemoprophylaxis.
Counseling
Encourage smoking cessation.
Approximately 10% of people in the United States age 65 and older are smokers.
Tobacco use has been linked to heart disease; peripheral vascular disease; cerebrovascular disease; chronic obstructive pulmonary disease; cancer such as lung, bladder, and esophageal malignancies; and numerous other health problems that decrease quality of life or cause premature death.
Although much damage has been done to the lungs and blood vessels by many years of smoking, older adults can still benefit from smoking cessation by increasing quality of life.
The U.S. Preventive Service Task Force recommends the “5-A” behavioral counseling framework as a useful strategy for engaging patients in smoking cessation discussions: (1) Ask about tobacco use; (2) Advise to quit through clear personalized messages; (3) Assess willingness to quit; (4) Assist to quit; and (5) Arrange follow-up and support.
Encourage physical activity.
It has been stated that 75% of older Americans are inactive.
It has been recommended that older adults participate in regular activity, especially aerobic activities that promote cardiovascular fitness, such as walking, cycling, or swimming.
Refer to a physical, occupational, or rehabilitation therapist. An individualized exercise prescription should be developed and cleared with the health care provider.
Identify alcohol abuse in older adults.
The consequences of alcoholism include liver disease, gastrointestinal (GI) bleeding, and motor vehicle accidents.
Question older adults about drug or alcohol abuse. Although street drug use is rare, prescription drug abuse may be occurring or alcohol may be used for pain.
Recognize the signs and symptoms of alcohol abuse in older adults (see Box 9-1).
Refer for counseling.
Evaluate and counsel on dental health.
Dental problems in older adults include missing teeth, illfitting dentures, periodontal disease, and tooth decay.
Dental problems commonly lead to poor eating habits, apathy, and fatigue.
Regular dental care should be encouraged to improve nutrition and the quality of life.
Immunizations
Evidence Base
Centers for Disease Control and Prevention. (2012). Advisory Committee for Immunization Practices (ACIP) recommendations. Atlanta, GA: CDC. Available: www.cdc.gov/vaccines/pubs/ACIP-list. htm#pcv.
BOX 9-1 Signs of Alcohol Abuse in Older Adults
Difficulty with gait and balance
Acute change in cognition
Frequent falls or accidents
Change in drinking patterns
Poor nutritional intake
Poor hygiene and self-care
Lack of physical exercise
Social isolation
Pneumococcal pneumonia and influenza are significant causes of mortality and morbidity in older adults.
It is recommended that a single dose of the pneumococcal vaccine be given to all people age 65 or over.
A second dose is recommended for individuals aged 19 to 64 who have functional or structural asplenia or immunocompromising conditions 5 years after the first.
Influenza may cause significant complications in older adults. Annual influenza vaccination is recommended for all people over age 6 months. Several antiviral agents are effective against influenza. These agents can be effective in ameliorating symptoms if given within 48 hours of onset of illness.
Tetanus-diphtheria (Td) immunization is an important but frequently forgotten component of health maintenance, especially in older adults.
The mortality rate of tetanus exceeds 50% in those over age 65.
Combined tetanus-diphtheria boosters should be given every 10 years; no age for discontinuation has been stated.
Due to an increase in pertussis cases, a single dose of acellular pertussis is also recommended as a component (Tdap) for adults aged 65 years and older who anticipate having close contact with an infant less than 12 months of age and who previously have not received Tdap. Tdap can be administered regardless of interval since the last tetanus booster.
For those with no history of immunization or unknown immunization status, a primary series should be initiated, consisting of two doses of tetanus-diphtheria vaccine at least 4 weeks apart, followed by a third dose 6 to 12 months later.
A single dose of the herpes zoster vaccine is recommended for older adults to prevent the dermatologic reoccurrence of varicella and the possible painful sequela known as postherpetic neuralgia.
Age is the most important factor in the development of herpes zoster, with a large increase beginning between age 50 and 60, and about 50% of people experience herpes zoster by age 85.
Chemoprophylaxis
The risk and benefits of oral anticoagulation therapy should be considered for older adults at risk of cardiovascular disease, particularly stroke. The United States Preventive Services Task Force (USPSTF) strongly recommends that clinicians discuss aspirin therapy with patients at risk for coronary heart disease.
Contraindicated if patient is at risk for GI bleeding.
Should be discussed with older adults with regard to prevention of deep vein thrombosis, nonvalvular atrial fibrillation, cardiomyopathy, valvular heart disease, mechanical prosthetic heart valves, and acute myocardial infarction.
Calcium, vitamin D, and other agents, such as selective estrogen receptor modulators or bisphosphonates, may be considered for those at risk for osteoporosis.
Secondary Prevention
Secondary prevention is the detection of disease in an early stage for best treatment outcomes, such as cancers, cardiovascular disease, osteoporosis, and tuberculosis.
Screening Recommendations
Evidence Base
United States Preventive Services Task Force. (2012). The guide to clinical preventive services: Recommendations of the U.S Preventive Services Task Force. Available: www.uspreventiveservices taskforce. org/index.html.
Age alone is not a criterion as to when to stop screening. Rather, the patient and health care provider should discuss values, expectations, functional status, and quality of life. A guide to shared decision making for cancer screening is available at the USPSTF website at www. uspreventiveservicestaskforce.org/3rduspstf/shared/sharedba.htm. The USPSTF has made the following recommendations for cancer screenings for older adults:
The precise age at which to discontinue screening mammography is uncertain. No clinical trials have been conducted on women over age 74. Furthermore, although older women face a higher probability of developing breast cancer, they also have a greater chance of dying from other causes.
Regarding cervical cancer, it is appropriate for older women to discontinue cervical cancer screening after age 65 only if they have had adequate recent screening with normal results and are not at high risk for cervical cancer.
The age to discontinue colorectal cancer screening has not been determined; however, the USPSTF recommends against routine colorectal cancer screening in adults ages 75—85, unless there are conditions that support screening for these individuals.
The USPSTF states that there is insufficient evidence to recommend for or against screening for prostate cancer. Older men and men with other significant medical conditions who have a life expectancy of fewer than 10 years are unlikely to benefit from the prostate-specific antigen test and digital rectal examination.
Tertiary Prevention
Tertiary prevention addresses the treatment of established disease to avoid complications and death. The major areas of focus for the older adult are preventing the complications of immobility and rehabilitation
Preventing Complications of Immobility
Positioning
The goal of frequent position changes is to prevent contractures, stimulate circulation and prevent pressure sores, prevent thrombophlebitis and pulmonary embolism, promote lung expansion and prevent pneumonia, and decrease edema of the extremities. Changing position from lying to sitting several times per day can help prevent changes in the cardiovascular system, which is known as deconditioning.
The recommendation is to change body position at least every 2 hours and, preferably, more frequently in patients who have no spontaneous movement.
Evidence Base
Only gold members can continue reading. Log In or Register to continue
 Evidence Base
Evidence Base Evidence Base
Evidence Base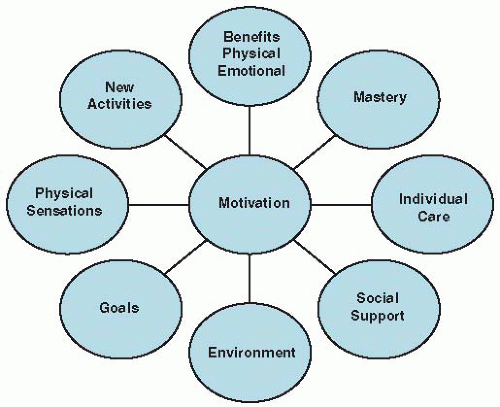
 Evidence Base
Evidence Base Evidence Base
Evidence Base Evidence Base
Evidence Base



