Cardiovascular Function and Therapy
Cardiovascular Function and Therapy
OVERVIEW AND ASSESSMENT
Common Manifestations of Heart Disease
In patients with cardiac disease, chest pain is the most common manifestation and is the second most common chief complaint presenting to emergency departments. Heart disease may also be characterized by shortness of breath, palpitations, weakness, fatigue, dizziness, syncope, diaphoresis, or GI complaints.
Chest Pain
Characterization
How does the patient describe chest pain? Is it mild or severe, transient or constant? What activity or other factors make it worse, or better? Can it be characterized as tightness, discomfort, fullness, pressure-like, crushing, or searing? Does it radiate to the jaw, neck, back, or arm (particularly left)?
Assess chest pain systematically. See
Box 12-1. Most pain management scales (visual analogues or numerical scales) are fast and easy to use, but can only be used to measure the intensity
of the pain; these scales do not measure the other essential elements for describing chest pain. In your assessment, ascertain the character and quality of the pain; location and radiation of the pain; factors that precipitate, aggravate, or relieve the pain; the duration of the pain; and any associated symptoms.
Use one of two popular and similar assessment mnemonics— OLDCARTS or the PQRST assessment (see
Chapter 5, page 47) to evaluate chest pain.
Significance
Ischemia caused by an increase in demand for coronary blood flow and oxygen delivery, which exceeds available blood supply; may result from coronary artery disease (CAD) or a decreased supply without an increased demand due to coronary artery spasm or thrombus.
Pain that is brought on by exertion and relieved by rest suggests angina pectoris or psychogenic pain. Psychogenic pain differs from angina in that it is usually associated with other symptoms, such as headache, back pain, stomach pain, and hyperventilation. Angina is usually caused by three Es: exercise, emotion, and eating.
Chest pain that worsens on deep inspiration or cough is suggestive of pleural, pericardial, or chest wall type pain.
Chest wall tenderness and pain on inspiration is suggestive of costochondritis.
Chest pain that is relieved by leaning forward and aggravated by lying down suggests pericarditis.
Sudden onset of chest pain accompanied by dyspnea is suggestive of pulmonary emboli or pneumothorax.
Dissecting aortic aneurysm is likely in the hypertensive patient who complains of a sudden onset of tearing, ripping pain.
If the patient reports chest pain while eating, this suggests angina or esophageal spasm or biliary (cholecystitis), pancreatic (pancreatitis), or gastric disease (gastroesophageal reflux disease or ulcers).
A panic attack may imitate a heart attack but is more common in younger individuals and in women more than in men.
Shortness of Breath (Dyspnea)
Characterization
What precipitates or relieves dyspnea?
How many pillows does patient sleep with at night?
How far can patient walk or how many flights of stairs can patient climb before becoming dyspneic?
Determine the type of dyspnea.
Exertional—breathlessness on moderate exertion that is relieved by rest.
Paroxysmal nocturnal—sudden dyspnea at night; awakens patient with feeling of suffocation; sitting up relieves breathlessness.
Orthopnea—shortness of breath when lying down. Patient must keep head elevated with more than one pillow to minimize dyspnea.
Significance
Exertional dyspnea occurs as a result of an elevated pulmonary artery pressure (PAP) due to left ventricular dysfunction.
Paroxysmal (nocturnal) dyspnea, also known as cardiac asthma, is precipitated by stimuli that aggravate previously existing pulmonary congestion, resulting in shortness of breath that generally occurs at night and usually awakens the patient.
Orthopnea (dyspnea in the supine position) is caused by alterations in gravitational forces resulting in an elevation in pulmonary venous pressure and PAP. These, in turn, increase the pulmonary closing volume and reduce vital capacity. Orthopnea indicates advanced heart failure.
Palpitations
Characterization
Does patient feel heart pounding, fluttering, beating too fast, or skipping beats?
Does patient experience dizziness or faintness with palpitations?
What brings on this sensation?
How long does it last?
What does patient do to relieve these sensations?
Significance
Pounding, jumping, fluttering sensations occur in the chest due to a change in the patient’s heart rate or rhythm or an increase in the force of its contraction.
Palpitations can occur as a result of cardiac arrhythmia as well as many other cardiac and noncardiac conditions.
Palpitations can be a manifestation of depression and panic disorders.
Palpitations can be intermittent, sustained and regular, or irregular.
Palpitations are most significant if dizziness and difficulty breathing occur simultaneously.
Palpitations that have a gradual onset and terminate in a pounding heartbeat may indicate sinus tachycardia.
Palpitations may be caused by noncardiac causes, such as thyrotoxicosis, hypoglycemia, pheochromocytoma, and fever.
Certain substances, such as tobacco, coffee, tea, and alcohol, as well as certain drugs, including epinephrine, ephedrine, aminophylline, and atropine, may also precipitate arrhythmias and palpitations.
Weakness and Fatigue
Characterization
What activities can you perform without becoming tired?
What activities cause you to become tired, weak, or fatigued?
Is the fatigue relieved by rest?
Is leg weakness accompanied by pain or swelling?
Significance
Fatigue can be produced by low cardiac output (CO) due to right- or left-sided heart failure. The heart can’t provide sufficient blood to meet the increased metabolic needs of cells.
As heart disease advances, fatigue is precipitated by less effort.
Weakness or tiring of the legs may be caused by peripheral arterial or venous disease.
Weakness and tiredness may be related to electrolyte imbalances, such as hypokalemia, hyperkalemia, hypercalcemia, hypernatremia, hyponatremia, hypophosphatemia, and hypermagnesemia.
Other disorders, such as chronic fatigue syndrome, multiple sclerosis, fibromyalgia, influenza, and Lyme disease, may also cause weakness and fatigue.
Dizziness and Syncope
Characterization
Is the dizziness characterized as lightheadedness, feeling faint, off balance, vertigo, or spinning?
How many episodes of syncope or near syncope have been experienced?
Did a hot room, hunger, sudden position change, defecation, or pressure on your neck precipitate the episode?
Significance
Patients who experience anxiety attacks and hyperventilation syndrome frequently experience faintness and dizziness.
Patients who suffer repeated bouts of unconsciousness may be experiencing seizures rather than syncope.
Syncope can be a result of hypoglycemia, anemia, or hemorrhage.
Vasovagal (vasodepressor or neurocardiogenic) syncope can be precipitated by a hot or crowded environment, alcohol, extreme fatigue, severe pain, hunger, prolonged standing, and emotional or stressful situations. Vasovagal syncope is caused by temporary slowing of the heart and reduction of brain perfusion.
Orthostatic or postural hypotension, another cause of dizziness, occurs when the patient stands up suddenly.
Cardiac syncope results from a sudden reduction in CO due to bradyarrhythmias and/or tachyarrhythmias.
Cerebrovascular disease such as carotid stenosis can cause dizziness and syncope due to reduced cerebral blood flow.
Nursing History
Past Medical History
Medical and Surgical History
Review of Allergies
Ask if the patient is allergic to any drugs, foods, environmental agents, or animals, and what reaction occurred.
Allergies to penicillin or other commonly used emergency drugs, such as lidocaine or morphine, may influence the choice of drug treatments, if needed.
Allergies to shellfish indicate iodine allergy; many contrast dyes used in radiologic procedures contain iodine.
Does the patient have allergies to aspirin or nonsteroidal anti-inflammatory drugs, such as naproxen and ibuprofen? (An upset stomach or indigestion from aspirin is not an allergy—rather, it is sensitivity; the patient may still be able to take an enteric-coated aspirin.)
Medications
Assess the patient’s prescription drugs, if any. Many cardiac drugs must be tapered to prevent a “rebound effect,” whereas other drugs affect heart rate and may cause orthostatic hypotension. Estrogen preparations may lead to thromboembolism.
Assess the patient’s use of over-the-counter medications, which may cause an increase in heart rate and blood pressure.
Assess the patient’s use of herbal preparations, vitamin and mineral supplements, and other alternative or complementary
therapies. Herbal preparations can interact with other drugs, anesthesia, and interfere with normal blood clotting.
Family History
Note the ages and health status of patient’s family members (parents, grandparents, siblings, and other blood relatives).
A family history of CAD, MI, sudden death, hypertension, hyperlipidemia, hypercholesterolemia, or diabetes could place the patient at an increased risk for heart disease.
Personal and Social History
Physical Examination
General Appearance
Is the patient awake and alert or lethargic, stuporous, or comatose?
Does the patient appear to be in acute distress; for example, clenching the chest (Levine’s sign)? Focus the physical assessment on what is essential when examining a patient in acute distress.
Observe the patient’s general build (eg, thin, emaciated, or obese) and skin color (eg, pink, pale, ruddy, flushed, or cyanotic).
Assess the patient for shortness of breath and distention of jugular veins.
Vital Signs
Obtain temperature and note route.
Determine heart rate and rhythm.
Assess pulse rate and rhythm using the radial artery.
Time for 1 full minute; note regularity.
Compare apical and radial heart rate (pulse deficit).
Rhythm should be noted as regular, regularly irregular, or irregularly irregular.
Monitor blood pressure.
Blood pressure can be measured indirectly using a sphygmomanometer and a stethoscope, electronic devices (dynamo), or directly by way of an arterial catheter.
Avoid taking blood pressure in an arm with an atriovenous shunt or fistula or on the same side as a mastectomy site or any type of lymphedema.
If possible, take pressure in both arms and note differences (5 to 10 mm Hg difference is normal). Differences of more than 10 mm Hg may indicate subclavian steal syndrome or dissecting aortic aneurysm.
Determine pulse pressure (systolic pressure minus diastolic pressure), which reflects stroke volume, ejection velocity, and systemic resistance, and is a noninvasive indicator of CO (30 to 40 mm Hg, normal; less than 30 mm Hg, decreased CO).
Note presence of pulsus alternans—loud sounds alternate with soft sounds with each auscultatory beat (hallmark of left-sided heart failure).
Note presence of pulsus paradoxus—abnormal fall in blood pressure more than 10 mm Hg during inspirations (cardinal sign of cardiac tamponade).
Assess for orthostatic hypotension.
Orthostatic hypotension occurs when a patient’s blood pressure drops 15 to 20 mm Hg or more (with or without an increase in heart rate of at least 20 beats/minute) when rising from a supine to sitting or standing position.
Autonomic compensatory factors for upright posture are inadequate due to volume depletion; bed rest; drugs, such as beta- or alpha-adrenergic blockers; or neurologic disease; prompt hypotension occurs with assumption of the upright position.
Note changes in heart rate and blood pressure in at least two of three positions: lying, sitting, standing; allow at least 3 minutes between position changes before obtaining rate and pressure.
Head, Neck, and Skin
Examination of the head includes assessment of facial characteristics and facial expressions, color of skin, and eyes, any of which can reveal underlying cardiac disease.
Earlobe creases in a patient younger than age 45 may indicate a genetic tendency toward CAD.
Facial color: look for a malar flush, cyanotic lips, or slightly jaundiced skin (rheumatic heart disease).
De Musset’s sign (head bobbing with each heartbeat) may indicate severe aortic insufficiency.
Facial edema may be noted with constrictive pericarditis and associated tricuspid valve disease.
Examine neck for jugular venous pulse. Jugular vein distention is characteristic of heart failure and other cardiovascular disorders, such as constrictive pericarditis, tricuspid stenosis, and obstruction of the superior vena cava.
Examine skin for temperature, diaphoresis, cyanosis, pallor, jaundice.
Warm, dry skin indicates adequate CO; cool, clammy skin indicates compensatory vasoconstriction due to low CO.
Cyanosis may be central (noted on tongue, buccal mucosa, and lips) due to bronchiectasis, COPD, heart failure, lung cancer, pneumothorax, polycythemia vera, pulmonary
edema, pulmonary emboli, shock, and sleep apnea; or peripheral (noted on distal aspects of extremities, tip of nose, and earlobes) due to chronic arteriosclerotic occlusive disease, Buerger’s disease, deep vein thrombosis (DVT), heart failure, acute peripheral occlusions, and Raynaud’s disease and cold exposure.
Jaundice may be a sign of right-sided heart failure or chronic hemolysis from prosthetic heart valve.
Xanthelasmas are yellow plaque (fatty deposits) evident on skin, commonly seen along the nasal side of one or both eyelids. Xanthelasmas are associated with hyperlipidemia and CAD and may occur normally in the absence of hyperlipidemia.
Pallor indicates decreased peripheral oxyhemoglobin or decreased total oxyhemoglobin. Onset may be sudden or gradual and extent may be generalized (most apparent on the face, conjunctiva, oral mucosa, and nail beds) or local (seen only in the affected limb).
Extremities
Inspect nail beds for color, splinter hemorrhages, clubbing, and capillary refill.
Color—pale nail beds may be indicative of anemia, whereas cyanosis may be indicative of decreased oxygenation.
Splinter hemorrhages are thin brown lines in nail bed and are associated with endocarditis. Janeway lesions (nontender, small erythematous or hemorrhagic macular or nodular lesions on the palm and soles) is indicative of infective endocarditis.
Clubbing (swollen nail base and loss of normal angle) is associated with chronic pulmonary or cardiovascular disease.
Capillary refill indicates an estimate of the rate of peripheral blood low.
Inspect and palpate for edema—if pitting edema, describe degree of edema in terms of depth of pitting that occurs with slight pressure: 1+ or mild—0 to ¼ inch (0 to 0.6 cm), 2+ or moderate—½ inch (1.3 cm), 3+ to 4+ or severe—¾ to 1 inch (2 to 2.5 cm).
Palpate arterial pulses (see
page 68).
Laboratory Studies
Cardiovascular function and disease are evaluated by blood tests that indirectly monitor heart function and structural damage.
Enzymes and Isoenzymes
The diagnostic utilization of cardiac markers has evolved dramatically over the past 50 years. When myocardial tissue is damaged (eg, due to MI), cellular injury results in the release of intracellular enzymes and proteins (cardiac enzymes, isoenzymes, and biochemical markers) into the bloodstream, which, in turn, causes elevated peripheral blood enzyme levels (see
Table 12-1).
Creatine kinase (CK) has a 98% sensitivity for acute myocardial infarction (AMI) 72 hours after infarction. CK is a catalyst for energy production and is found in brain, myocardium, and skeletal muscle. CK is sensitive but not specific for myocardial injury.
CK isoenzymes are more specific than CK. Three CK isoenzymes have been identified: CK-MM, CK-MB, and CK-BB,
with only CK-MB related to the heart. The specificity of CK-MB is greater than 85% and in some cases as high as 100%, but false positives do occur. Two types of CK-MB assays (CK-MB mass and CK-MB activity) are presently used.
CK-MB mass assays are found to be more sensitive than CK-MB activity assays.
CK-MB mass increases about 3 hours after onset of chest pain, whereas CK-MB activity requires another hour to elevate.
CK-MB index is the ratio of CK-MB to the total CK and is considered abnormal when it exceeds 3% to 5%.
Eventually, electrophoresis further breaks down CK-MB into its isoforms or subforms (CK-MB1 and CK-MB2). Normally, the ratio of CK-MB2 to CK-MB1 is 1:1. In myocardial injury, the CK-MB2/MB1 ratio increases to greater than 1.5 within 1 to 1½ hours. CK-MB isoforms have 56% sensitivity for patients presenting within 4 hours of the onset of symptoms.
The troponin complex is located on the thin filament of the contractile apparatus of striated and skeletal muscle and consists of three subunits: troponin C (TnC), troponin T (TnT), and troponin I (TnI). In the presence of myocardial damage, the troponin complex on the myofibril breaks down and the subunits of troponin are slowly released into the bloodstream.
TnC is not sensitive or specific for myocardial injury.
TnT has a sensitivity of approximately 50% within 4 hours of the onset of chest pain, but increases to approximately 75% sensitivity after 6 hours of onset and approximately 100% sensitivity in 12 hours. However, its specificity for myocardial injury is lower.
TnI has been found to be the most sensitive and specific for myocardial injury. It has little sensitivity within 4 hours of the onset of chest pain, but increases to 96% sensitivity after 6 hours of the onset of symptoms.
Myoglobin is a small, oxygen-binding protein found in cardiac and skeletal muscles and is rapidly released into the bloodstream. Myoglobin is sensitive very early after injury, but has poor sensitivity over time and can generate many false-positive results. When myoglobin levels are assessed with CK-MB results, sensitivity increases (as high as 96%), but specificity can drop to as low as 81%.
Myoglobin is directly related to muscle mass and is affected by age (levels increase with age), race (blacks have higher levels), gender (women have higher levels), and physical activity.
Myoglobins can be elevated in the presence of reinfarction, skeletal muscle or neuromuscular disorders, trauma, severe burns, electrical shock, alcohol withdrawal delirium, metabolic disorders, systemic lupus erythematosus, strenuous exercise, renal failure, I.M. injections, cardiac bypass surgery, seizures, and heart failure.
Other Biochemical Markers
Homocysteine is a toxic by-product of the metabolism of the amino acid methionine into cysteine. Homocysteine exerts a direct cytotoxic effect on the endothelium of blood vessels by blocking the production of nitrous oxide, resulting in decreased pliability of vessels and development of atherosclerotic plaque. Increased homocysteine levels ultimately result in atherosclerosis, CAD, MI, stroke, thromboembolism, and peripheral vascular disease.
Hyperhomocystinemia (increased homocysteine levels) are related to gender (male), advanced age, smoking, hypertension, elevated cholesterol, decreased folate, decreased levels of vitamin B6 and B12, and lack of exercise.
Homocysteine can also be elevated in the presence of other diseases, drug use, and caffeine intake.
B-type natriuretic peptide (BNP) is synthesized in the ventricular myocardium and released as a response to increased wall stress. BNP is used for diagnosis and prognosis of suspected heart failure. Plasma levels of BNP increase in the presence of left ventricular systolic and diastolic dysfunction, particularly in the presence of decompensating heart failure.
An increased BNP level identifies patients at the highest risk of developing sudden cardiac death and those who are in need of heart transplant. It is also associated with heart failure readmissions.
BNP is considered a useful marker of myocardial function and is used to guide therapy.
C-reactive protein (CRP) is an inflammatory marker that may be an important risk factor for atherosclerosis and ischemic heart disease. CRP is produced by the liver in response to systemic cytokinesis. Elevated CRP is associated with AMI, stroke, and the progression of peripheral vascular disease. However, it can also be elevated with any inflammatory process. In addition to revealing events associated with CAD, CRP can also be used to identify patients at risk for developing CAD.
Lipoprotein (a) is a molecule that is similar to low-density lipoprotein cholesterol (LDL-C). It increases cholesterol deposits in the arterial wall, enhances oxidation of LDL-C, and inhibits fibrinolysis, resulting in the formation of atherosclerotic plaque and thrombosis. Treatment of elevated lipoprotein (a) is suggested only for patients with a history of premature vascular disease without other risk factors.
Factor I, or fibrinogen, is directly linked to increased cardiovascular risk. It is involved in the coagulation cascade (converting fibrinogen to fibrin by thrombin), stimulates smooth-muscle cell migration and proliferation, and promotes platelet aggregation, which increases blood viscosity.
Nursing and Patient Care Considerations
Make sure that enzymes are drawn in a serial pattern, usually on admission and every 6 to 24 hours until three samples are obtained; enzyme activity is then correlated with the extent of heart muscle damage.
Maintain standard precautions while obtaining blood specimens and properly dispose of all equipment.
Advise patient that results of blood tests will be interpreted based on time and within the context of risk factors and other diagnostic tests.
Radiology and Imaging
Chest X-ray
Chest x-rays can be used to assess heart size, contour, and position and may also reveal cardiac and pericardial calcification as well as physiologic alterations in pulmonary circulation. For further description and nursing considerations, see
page 206.
Myocardial Imaging
Description
With the use of radionuclides and scintillation cameras, radionuclide angiograms can be used to assess left ventricular performance.
Thallium-201 is a radionuclide (an unstable atom that produces a small amount of energy) that behaves like potassium in the body and is distributed throughout the myocardium in proportion to blood flow.
Technetium-99m-labeled sestamibi is a myocardial perfusion marker used to assess cell membrane and mitochondrial integrity and to reveal myocardial perfusion.
Sestamibi is not taken up by acute or chronic infarct tissue, and the amount of uptake of the radionuclide by other tissue correlates with the size of the infarction, the amount of CK released in the blood, and the postinfarction left ventricular ejection fraction (LVEF).
“Hot spot” or positive imaging with technetium-99m stannous pyrophosphate is used when diagnosis of MI is unclear.
Negative result of “cold spot” imaging with thallium-201 rules out MI. A positive result, on the other hand, is inconclusive because it cannot differentiate between old and new infarction or areas of ischemia versus infarction.
Radionuclide ventriculogram with technetium-99m is used to evaluate valve structure and ventricular function. In this test, a contrast medium is injected through a catheter, opacifying the ventricular cavity to enable measuring of right and LVEF. The test also distinguishes regional from global ventricular wall motion and allows subjective analysis of cardiac anatomy to detect intracardiac shunts as well as valvular or congenital abnormalities.
Complications of ventriculography include arrhythmias, intramyocardial or pericardial injection of contrast medium, and, possibly, development of emboli due to injection of air or a thrombosis through the catheter.
Dual single-photon emission computed tomography with simultaneous imaging with 99m-Tc PYP and 201-Tl improves the accuracy of detecting 99m-Tc PYP accumulation and assessing the infarcted area. The overlap of both isotopes may reflect the presence of salvaged myocardium adjacent to necrotic tissue.
Nursing and Patient Care Considerations
Advise patient that a radionuclide will be injected through a central venous, Swan-Ganz, or IV catheter, or into an antecubital vein.
Reassure patient that the radionuclide will not cause radiation injury or affect heart function.
Explain to patient that hot flashes and nausea or vomiting may occur. A test dose will be administered before the dose required for contrast to assess patient’s tolerance of radionuclide.
Results of the study will be discussed by the patient’s health care provider after the study is interpreted by the radiologist.
Treadmill Stress Testing
Description
In treadmill stress testing, the patient walks a treadmill or rides a stationary bicycle until reaching a target heart rate, typically 70% to 80% of the maximum predicted heart rate. Treadmill stress testing has 70% sensitivity and specificity among the general population.
Indications for stress testing have been adapted from the American Heart Association (AHA) and the American College of Cardiology (see
Box 12-2).
Reasons for terminating a stress test include:
ST-segment elevations of 2 mm or more.
20 mm Hg drop in systolic blood pressure.
Drop in heart rate or the development of heart block.
Progressively increasing angina.
ST-segment depression of 2 mm or greater.
Three or more premature ventricular contractions (PVCs).
Supraventricular arrhythmias.
Severe hypertension.
ST-segment depression at baseline that progresses during the test.
Claudication.
Fatigue, dyspnea, or feelings of light-headedness.
Equipment malfunction.
Sustained ventricular tachycardia.
Complications of stress testing include supraventricular tachyarrhythmias, bradycardias, heart failure, hypotension, ventricular ectopy (due to ventricular tachycardia), ventricular fibrillation, stroke, MI, and death.
Contraindications for performing a stress test include:
AMI within 2 days.
Unstable coronary syndrome.
Wolff-Parkinson-White syndrome.
Uncontrolled arrhythmias.
High-degree atrioventricular (AV) blocks.
Acute myocarditis.
Acute pericarditis.
Severe aortic stenosis.
Uncontrolled hypertension.
Acute aortic dissection.
Acute pulmonary embolism or pulmonary infarct.
Nursing and Patient Care Considerations
Explain to patient how the procedure will be done and screen for contraindications.
Advise patient to abstain from eating, smoking, and consuming caffeine for 2 hours before the test.
Inform patient that monitoring will occur throughout the test for signs of complications.
Advise patient to inform you of how he or she is feeling during the test.
Monitor patient throughout testing for color, respirations, ECG changes, and blood pressure.
Echocardiography (Ultrasound Cardiography)
Description
Echocardiography is used to visualize and assess cardiac function, structure, and hemodynamic abnormalities. It is the most commonly used noninvasive cardiac imaging tool.
It records high-frequency sound vibrations that are sent into the heart through the chest wall. The cardiac structures return the echoes derived from the ultrasound. The motions of the echoes are traced on an oscilloscope and recorded on film, CD, or DVD.
Clinical usefulness includes demonstration of valvular and other structural deformities, detection of pericardial effusion, evaluation of prosthetic valve function, and diagnosis of cardiac tumors of asymmetric thickening of interventricular septum, cardiomegaly (heart enlargement), clots, vegetations on valves, and wall motion abnormalities.
Types include two-dimensional (2-D), M-mode, and Doppler mode. The methods are complementary and are commonly used in conjunction.
2-D echocardiography—provides a wider view of the heart and its structures because it involves a planar ultrasound beam.
M-mode—utilizes a single ultrasound beam and provides a narrow segmental view.
Doppler mode—evaluates pressures and blood flow across the valves; also assesses for atrial and ventricular septal defects.
Nursing and Patient Care Considerations
Advise patient that traditional echocardiography is noninvasive and that no preparation is necessary.
Position patient on left side, if tolerated, to bring the heart closer to the chest wall. Assist patient to clean chest of transducer gel after the test.
Transesophageal Echocardiography
Description
In transesophageal echocardiography (TEE), an ultrasound transmitter located at the end of a catheter is passed through the esophagus to the stomach, where flexion of the tip permits imaging of the heart through the stomach wall and the diaphragm, thus allowing clearer and more accurate diagnostic evaluation. It is particularly useful in evaluating valvular disease.
As the catheter is slowly withdrawn, views of cardiac structures are obtained at several levels in various 2-D planes.
TEE can be used for continuous monitoring of cardiac and noncardiac patients during surgery.
Atrial fibrillation is the most common indication for performing a TEE, used to evaluate for thromboembolism.
Nursing and Patient Care Considerations
Explain procedure to patient and provide written information, if possible.
This is an invasive procedure; patient will require mild sedation and must be kept on nothing-by-mouth status (NPO) for a specified time—usually 4 to 6 hours—before the procedure.
The entire procedure takes less than 30 minutes.
Results of the study will be discussed with patient by the patient’s health care provider after it is interpreted by the radiologist.
Stress Echocardiography
Description
Stress (treadmill) echocardiography has been found to have better sensitivity and specificity than treadmill stress testing alone.
Stress echocardiography is used to evaluate changes in wall motion when the patient is at rest and under stress.
Stress echocardiography can be coupled with pharmacologic stress testing. Myocardial perfusion imaging with dobutamine, adenosine, and dipyridamole is an alternative for patients who cannot exercise due to degenerative joint disease, physical deconditioning, neurologic disorders, COPD, or peripheral vascular disease.
Nursing and Patient Care Considerations
Explain procedure to patient and provide written information, if possible.
Withhold caffeine-containing products for 24 hours before adenosine and dipyridamole stress testing.
Discuss with cardiologist which medications should be withheld before test.
Maintain NPO status before testing for 2 hours or according to facility policy.
Establish a patent IV access.
Results of the study will be discussed with patient by the patient’s health care provider after fully interpreted.
Cardiac MRI
Magnetic resonance imaging (MRI) is used to evaluate diseased heart muscle. Currently three techniques are being used. Resting MRI can assess end-diastolic wall thickness and contractile function. Dobutamine MRI is used to evaluate contractile reserve. Contrast enhanced MRI allows for the visualization of the in vivo regions of microvascular obstruction. The extent of microvascular obstruction determines the magnitude of myocardial scarring. Once determined, the extent of microvascular obstruction is a strong predictor of myocardial remodeling and outcome after revascularization. It may eventually replace cardiac catheterization. Safety has been demonstrated in patients with permanent pacemakers and implantable cardioverter-defibrillators. For further description and nursing considerations, see
page 206.
Phlebography (Venography)
Description
An x-ray visualization of the vascular tree after the injection of a contrast medium to detect venous occlusion.
Nursing and Patient Care Considerations
Inform patient that an intense burning sensation in the vessel where the solution is injected may be experienced. This will last for only a few seconds.
Note evidence of allergic reaction to the contrast medium; this may occur as soon as the contrast medium is injected, or it may occur after the test.
Perspiring, dyspnea, nausea, vomiting.
Rapid heart rate, numbness of extremities.
Hives.
Advise patient to notify health care provider of signs of allergic reaction.
Observe injection site for redness, swelling, bleeding, and thrombosis.
Positron Emission Tomography
Description
Considered the most sensitive modality for detecting hibernating viable myocardium and predicting left ventricular recovery after coronary revascularization.
F-FDG, a glucose analog that is transported into cells through glucose membrane transportes is injected. It does not undergo any further metabolism (unlike glucose) and essentially is trapped within the cell.
Trapped F-FDG accumulates and becomes an index of cellular glucose utilization signifying ongoing cellular metabolism. Reduced FDG uptake (reduced or absent glucose metabolism) signifies myocardial scar. Also see
page 206.
Used to determine blood flow to the heart muscle and viability of areas with decreased function due to previous MI.
Allows for the differentiation of nonfunctioning heart muscle from heart muscle that would benefit from a procedure.
Nursing and Patient Care Considerations
Inform patient not to eat for 4 hours prior to the scan.
Check blood glucose prior to test for diabetic patients; if greater than 200, may need to reschedule test.
Encourage patient to drink water following the scan to assist excretion of contrast medium.
Other Diagnostic Tests
Electrocardiogram
Basic Principles
Despite its limited sensitivity and specificity, the 12-lead ECG is still the standard for the evaluation of myocardial ischemia.
Electrical activity is generated by the cells of the heart as ions are exchanged across cell membranes.
Electrodes that are capable of conducting electrical activity from the heart to the ECG machine are placed at strategic positions on the extremities and chest precordium (see
Figure 12-1).
The electrical energy sensed is then converted to a graphic display by the ECG machine. This display is referred to as the ECG.
Each ECG lead consists of a positive and negative pole; each lead also has an axis that represents the direction in which current flows.
Each lead takes a different view of the heart; therefore, the tracing will be different with each view obtained.
The direction in which electrical current flows determines how the waveform will appear.
There are three sets of leads:
Standard limb or bipolar leads (I, II, III) utilize three electrodes; these leads form a triangle known as Einthoven’s Triangle.
Augmented unipolar leads (AVR, AVL, AVF).
Precordial unipolar leads (V1, V2, V3, V4, V5, V6).
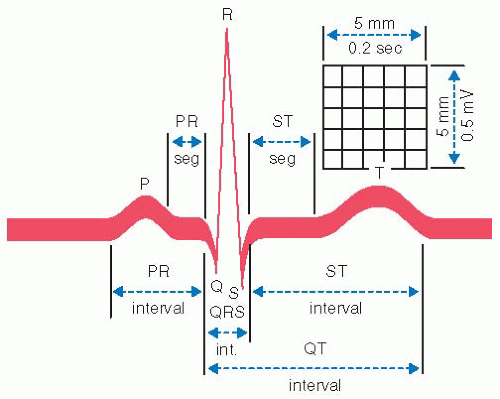
A heart contraction is represented on the ECG graph paper by the designated P wave, QRS complex, and T waves.
The P wave is the first positive deflection and represents atrial depolarization or atrial contraction.
The PR interval represents the time it takes for the electrical impulse to travel from the sinoatrial node to the AV node and down the bundle of His to the right and left bundle branches.
The Q wave is the first negative deflection after the P wave; the R wave is the first positive deflection after the P wave.
The S wave is the negative deflection after the R wave.
The QRS waveform is generally regarded as a unit and represents ventricular depolarization. Atrial repolarization (relaxation) occurs during the QRS complex, but cannot be seen.
The T wave follows the S wave and is joined to the QRS complex by the ST segment. The ST segment represents ventricular repolarization or relaxation. The point that represents the end of the QRS complex and the beginning of the ST segment is known as the J point.
The T wave represents the return of ions to the appropriate side of the cell membrane. This signifies relaxation of the muscle fibers and is referred to as repolarization of the ventricles.
The QT interval is the time between the Q wave and the T wave; it represents ventricular depolarization (contraction) and repolarization (relaxation).
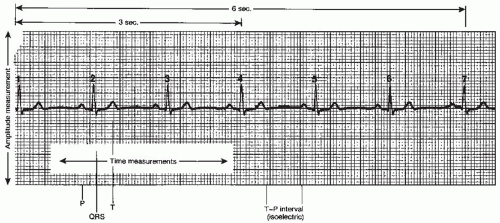
ECG Leads and Normal Waveform Interpretation
The normal amplitude of the P wave is 3 mm or less; the normal duration of the P wave is 0.04 to 0.11 second. P waves that exceed these measurements are considered to deviate from normal.
The PR interval is measured from the upstroke of the P wave to the QR junction and is normally between 0.12 and 0.20 second. There is a built-in delay in time at the AV node to allow for adequate ventricular filling to maintain normal stroke volume.
The QRS complex contains separate waves and segments, which should be evaluated separately. Normal QRS complex should be between 0.06 and 0.10 second.
The Q wave, or first downward stroke after the P wave, is usually less than 3 mm in depth. A Q wave of significant deflection is not normally present in the healthy heart. A pathologic Q wave usually indicates a completed MI.
The R wave is the first positive deflection after the P wave, normally 5 to 10 mm in height. Increases and decreases in amplitude become significant in certain disease states. Ventricular hypertrophy produces very high R waves because the hypertrophied muscle requires a stronger electrical current to depolarize.
The ST segment begins at the end of the S wave, the first negative deflection after the R wave, and terminates at the upstroke of the T wave.
The T wave represents the repolarization of myocardial fibers or provides the resting state of myocardial work; the T wave should always be present.
The P, Q, R, S, and T waves all appear differently depending on which lead you are viewing.
Nursing and Patient Care Considerations
Angiography
Description
Invasive imaging procedure that enables visualization of blood vessels for their patency of blood flow versus blockage through the insertion of a catheter into an artery or vein followed by injection of contrast dye.
Various types include coronary, aortic, renal, peripheral, cerebral, and pulmonary angiography; lymphangiogram; ventriculography; and fluorescein angiography.
Provides information that may direct assessment and management of cardiovascular and cerebrovascular disease, peripheral blockage (arterial and venous), aneurysms, arterial and venous malformations, thrombosis (deep vein or pulmonary embolus), fistulae; guide mapping prior to interventional procedures; and diagnose internal bleeding.
Nursing and Patient Care Considerations
Preprocedure
Question patient for known allergies, particularly to iodine (shellfish). If so, notify health care provider, who may want to prepare patient with oral corticosteroids and diphenhydramine before the study.
Make sure there is a signed consent and that patient/family questions have been answered.
Make sure fasting guidelines have been followed, varying from NPO to liquid or light diet. Follow facility policy; should be in accordance with American Society of Anesthesiologists guidelines (minimum fasting 6 hours from light meal, 2 hours from clear liquids) to minimize risk of pulmonary aspiration should emesis occur.
Make sure laboratory testing has been ordered and results reviewed, including blood urea nitrogen (BUN) and creatinine, to evaluate kidney function for ability to clear contrast dye; hemoglobin/hematocrit; platelet count and coagulation values, to ensure clotting and anticoagulation baseline; white blood cell (WBC) count, to rule out infection that may be exacerbated by invasive procedure; electrolytes; and blood type and screen, in case blood transfusion is necessary.
Make sure baseline ECG is on file.
Ensure IV patency for medication administration.
Make sure patient has voided.
Administer premedication, if ordered.
Postprocedure
Record vital signs according to facility policy and stability of patient.
Check for bleeding or hematoma formation at insertion site.
Check distal extremity for normal color and intact pulses.
Patient may complain of discomfort in the groin or other site depending on route by which contrast medium was administered. Check for bed rest/activity progression and special fluid instructions. Encourage fluids/hydration to ensure clearance of contrast dye.
Provide patient with discharge instructions, including follow-up care, medications, and driving and activity restrictions.
Diagnostic Electrophysiology Studies
Description
Electrophysiology studies (EPS) are a complex invasive procedure in which flexible catheters (with 2 to 10 electrodes) are placed percutaneously in the right or left femoral vein, the subclavian vein, the internal jugular vein, or the median cephalic veins. EPS assesses pacing thresholds and measures conduction intervals in the high right atrium, the right ventricular apex, the right ventricular outflow tract, the coronary sinuses, the bundle of His, and, occasionally, the left ventricle. The test is followed by programmed stimulation protocols to evaluate the heart’s conduction system.
Indications for EPS
Definite indications for EPS include:
Sustained ventricular tachycardia.
Cardiac arrest in the absence of AMI, antiarrhythmic drug toxicity, or electrolyte imbalance.
Syncope of uncertain origin (for which noncardiac causes have been ruled out).
Wide QRS tachycardia of uncertain etiology.
To evaluate the effectiveness of a device for the detection and electrical termination of tachycardias (pacemakers or implanted defibrillators).
Symptomatic Wolff-Parkinson-White syndrome.
Frequent symptomatic regular supraventricular tachycardia unresponsive to medications.
Possible indications for EPS include:
Asymptomatic Wolff-Parkinson-White syndrome.
Post-myocardial infarction.
Nonsustained ventricular tachycardia.
Cardiomyopathy.
Frequent ventricular ectopy.
Supraventricular tachycardia.
Contraindications for EPS include:
Asymptomatic sinus bradycardia.
Asymptomatic bundle-branch blocks.
Palpitation.
Atrial fibrillation or flutter.
Third-degree AV blocks.
Second-degree Mobitz type II AV blocks.
Nursing and Patient Care Considerations
Anticoagulants (warfarin) should be discontinued at least 3 days before EPS.
Discuss with health care provider which cardiac medications should be discontinued and when they should be discontinued.
Instruct patient to fast for at least 6 hours before the study.
Place electrodes for a 12-lead ECG, which will be recorded during the procedure.
Discuss with patient any feelings about the procedure and his or her physical condition. Patients frequently experience anxiety, fear of loss of control, denial, depression, and uncertainty.
Explain the procedure, its purpose, and the preparation involved.
Inform patient that pain medication and conscious sedation will be used during the procedure.
Postprocedure care includes:
Keeping extremity used for IV straight, restraining if necessary.
Monitoring patient’s groin for bleeding or hematoma formation.
Monitoring vital signs as ordered.
Providing emotional support to patient and family.
Cardiac Catheterization
Description
Cardiac catheterization is a diagnostic procedure in which a catheter is introduced into the heart and blood vessels to provide physiologic data to guide treatment; measure cardiovascular hemodynamics; acquire radiographic images of coronary arteries, cardiac chambers, and aorta; collect blood from various chambers for analysis; and evaluate pulmonary blood flow and shunts.
The access site of choice is the femoral vein; however, when there is peripheral vascular disease or morbid obesity, radial or brachial access is used, depending on distal pulses. The catheter is directed up the aorta and into the coronary vasculature to visualize coronary anatomy (right or left) and measure hemodynamics. In rare instances of aortic disease, a transseptal approach may be used.
Right-sided heart catheterization—right side of the heart is accessed to evaluate pulmonary shunts, cardiac anomalies, and valvular disease. A radiopaque catheter is passed from the femoral vein and through the inferior vena cava or from the basilic vein and through the superior vena cava into the right atrium, right ventricle, and pulmonary vasculature under direct visualization with a fluoroscope.
Right atrium and right ventricle pressures are measured; blood samples are taken for hematocrit and oxygen saturation.
After entering the right atrium, the catheter is then passed through the tricuspid valve and similar tests are performed on blood within the right ventricle.
Finally, the catheter is passed through the pulmonic valve and as far as possible beyond that point; capillary samples are obtained, capillary wedge pressure is recorded, and CO can be determined.
Complications include cardiac dysrhythmias, venous spasm, thrombophlebitis, infection at insertion site, cardiac perforation, and cardiac tamponade.
Left-sided heart catheterization—primarily done to diagnose coronary artery disease; usually done by retrograde approach by advancing the catheter up the aorta into the coronary anatomy.
Retrograde approach—catheter may be introduced percutaneously by puncture of the femoral artery or by direct brachial approach and advanced under fluoroscopic control into the ascending aorta and into the left ventricle.
Transseptal approach—catheter is passed from the right femoral vein (percutaneously or by saphenous vein cutdown) upward into right atrium. A long needle is passed up through the catheter and is used to puncture the septum separating the right and left atria; needle is withdrawn and the catheter is advanced under fluoroscopic control into left ventricle.
The catheter tip is placed at the coronary sinus and contrast medium is injected directly into one or both of the coronary arteries to evaluate patency.
Gives hemodynamic data—permits flow and pressure measurements of left side of heart.
Usually performed to evaluate the patency of coronary arteries and function of the left ventricular muscle and mitral and aortic valves; may also be done to evaluate patients before surgery.
Ventriculography—study of the left ventricle; catheter is passed into the left ventricle and dye is injected with a rapid, uniform rate via an injector machine to measure ejection fraction or function of the left ventricle.
Complications of left-sided heart catheterization and implications for nursing assessment include dysrhythmias (ventricular fibrillation), syncope, vasospasm, pericardial tamponade, MI, pulmonary edema, allergic reaction to contrast medium, perforation of great vessels of heart, systemic embolization (stroke, MI), loss of pulse distal to arteriotomy, and possible ischemia of lower arm and hand.
Angiography is usually combined with heart catheterization for coronary artery visualization.
Contraindications for cardiac catheterization include uncontrolled ventricular irritability, electrolyte imbalance, medication toxicity (digitalis), uncontrolled heart failure, renal failure, recent stroke (within past 3 months), active GI bleeding, active infection, uncontrolled hypertension, patient’s refusal, and pregnancy. Some of these conditions can be reversed or improved prior to catheterization.
Nursing and Patient Care Considerations Preprocedure
Question patient for known allergies, particularly iodine (shellfish), and make health care provider aware so that premedication with corticosteroid and antihistamine may be considered.
Make sure that there is a signed consent form and that patient and family questions have been answered.
Make sure that fasting guidelines have been followed, varying from NPO to liquid or light diet. Follow facility policy; should be in accordance with American Society of Anesthesiologists guidelines (minimum fasting 6 hours from light meal, 2 hours from clear liquids).
Make sure laboratory testing has been ordered and results reviewed, including BUN/creatinine, to evaluate kidney function for ability to clear contrast dye; hemoglobin/hematocrit; platelet count and coagulation values, to ensure clotting and anticoagulation baseline; WBC count, to rule out infection that may be exacerbated by invasive procedure; electrolytes; and blood type and screen, in case blood transfusion is necessary.
Make sure baseline ECG is on file.
Ensure IV patency for administration of medications.
Mark distal pulses.
Explain to patient that he or she will be lying on an examination table for a prolonged period and may experience certain sensations:
Occasional thudding sensations in the chest—from extrasystoles, particularly when the catheter is manipulated in ventricular chambers.
Strong desire to cough, which may occur during contrast medium injection into right side of heart during angiography.
Transient feeling of hot flashes or nausea as the contrast medium is injected.
Evaluate patient’s emotional status before catheterization, dispel myths, and provide factual information.
Have patient void before the procedure.
Allow for premedication (if any) to take effect prior to procedure.
Postprocedure
Record vital signs according to facility protocol and patient’s condition.
Check for bleeding or hematoma formation at insertion site.
Check distal extremity for normal color and intact pulses, and evaluate complaints of pain, numbness, or tingling sensation to determine signs of arterial insufficiency.
Assess for complaints of chest pain and respond immediately.
Follow activity restriction/progression directions, which are based on coagulation status and whether a vascular closure method was employed.
Evaluate complaints of back, thigh, or groin pain (may indicate retroperitoneal bleeding).
Obtain postprocedure ECG and labs according to facility protocol.
Be alert for signs and symptoms of vagal reaction (nausea, diaphoresis, hypotension, bradycardia); treat as directed with atropine and fluids.
Assess neurological status if receiving IIB/IIIA platelet inhibitors or thrombolytics according to facility protocol.
Provide discharge instructions, including follow-up care, medications, driving and activity restrictions, and the need to report any pain or above-listed problems.
GENERAL PROCEDURES AND TREATMENT MODALITIES
Hemodynamic Monitoring
Hemodynamic Monitoring is the assessment of the patient’s circulatory status; it includes measurements of heart rate (HR), intra-arterial pressure, CO, central venous pressure (CVP), PAP, pulmonary artery wedge pressure, and blood volume. It describes the intravascular pressure and flow of blood that occurs when the heart muscle contracts and pumps blood throughout the body.
The primary purpose is the early detection, identification, and treatment of life-threatening conditions, such as heart failure, cardiac tamponade, and all types of shock (septic, cardiogenic, neurogenic, anaphylactic). See
Procedure Guidelines 12-1, pages 338 to 341;
Procedure Guidelines 12-2, pages 342 to 345; and
Procedure Guidelines 12-3, pages 346 to 347.
Cardiac Output
Cardiac output (CO) is the amount (volume) of blood ejected by the left ventricle into the aorta in 1 minute. Normal CO is 4 to 8 L/minute.
Underlying Considerations
CO is determined by stroke volume (SV) and HR. Thus, CO = SV × HR. CO must be maintained to adequately oxygenate the body.
HR = number of cardiac contractions per minute. The integrity of the conduction system and nervous system innervation of the heart influence functioning of this determinant.
SV = amount of blood ejected from ventricle per beat (normal SV is 50 to 100 mL/beat). The amount of blood returning to the heart (preload), venous tone, resistance imposed on the ventricle before ejection (afterload), and the integrity of the cardiac muscle (contractility) influence the functioning of this determinant.
The body alters CO through increases or decreases in one or both of these parameters. CO is maintained if the HR falls by an increase in SV. Likewise, a decrease in SV produces a compensatory rise in HR to keep the CO normal.
CO will decrease if either of the determinants cannot inversely compensate for the other.
CO measurements are adjusted to patient size by calculating the cardiac index (CI). CI equals CO divided by body surface area (BSA); BSA is determined through standard charts based on individual height and weight. Normal CI is 2.5 to 4 L/minute/m2.
Assessment of Cardiac Output
Signs of low CO include:
Changes in mental status.
An increase in HR.
Shortness of breath.
Cyanosis or duskiness of buccal mucosa, nail beds, and earlobes.
Falling blood pressure.
Low urine output.
Cool, moist skin.
Decreased or no appetite.
Methods
CO is measured by various techniques. In the clinical setting, it is usually measured by the thermodilution technique in conjunction with a flow-directed balloon-tipped pulmonary artery catheter (commonly known as Swan-Ganz catheter after the inventors).
The Swan-Ganz catheter is positioned in its final position in a branch of the pulmonary artery; it has a thermistor (external sensing device) situated 1½ inches (4 cm) from the tip of the catheter, which measures the temperature of the blood that flows by it.
To ensure accuracy of hemodynamic values, the transducer must be at the appropriate level and zeroed according to facility policy.
Leveling is performed to eliminate the effects of hydrostatic pressure in the transducer. It must be done with every change in bed height and elevation of the bed and prior to zeroing and calibration.
Zeroing is performed to eliminate the effects of atmospheric pressure in the transducer. It should be performed before connecting the pressure system to the patient, with any leveling, and whenever there is a significant change in hemodynamic variables.
All values should be rated at the end of expiration.
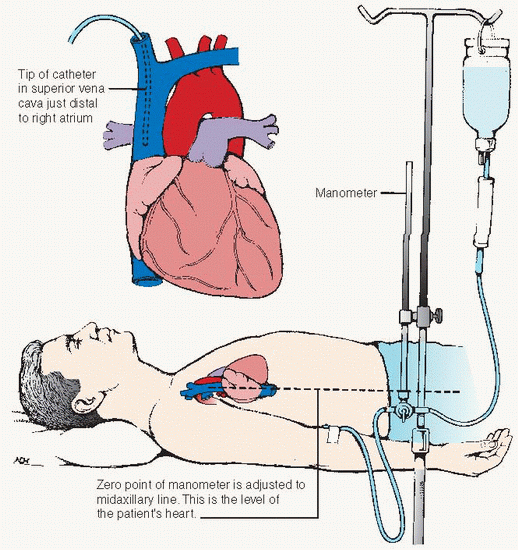
Central Venous Pressure Monitoring
Refers to the measurement of right atrial pressure or the pressure of the great veins within the thorax (normal range: 5 to 10 cm H2O or 2 to 8 mm Hg).
Right-sided cardiac function is assessed through the evaluation of CVP.
Left-sided heart function is less accurately reflected by the evaluation of CVP, but may be useful in assessing chronic right- and left-sided heart failure and differentiating right and left ventricular infarctions.
Requires the threading of a catheter into a large central vein (subclavian, internal or external jugular, median basilic, or femoral). The catheter tip is then positioned in the right atrium, upper portion of the superior vena cava, or the inferior vena cava (femoral approach only).
Purposes of CVP monitoring are to serve as a guide for fluid replacement and to monitor pressures in the right atrium and central veins.
The CVP catheter can also be used:
To obtain venous access when peripheral vein sites are inadequate.
To obtain central venous blood samples.
To administer blood products, total parenteral nutrition, and some drug therapies contraindicated for peripheral infusion.
To insert a temporary pacemaker.
 NURSING ALERT
NURSING ALERT NURSING ALERT
NURSING ALERT DRUG ALERT
DRUG ALERT NURSING ALERT
NURSING ALERT NURSING ALERT
NURSING ALERT NURSING ALERT
NURSING ALERT NURSING ALERT
NURSING ALERT DRUG ALERT
DRUG ALERT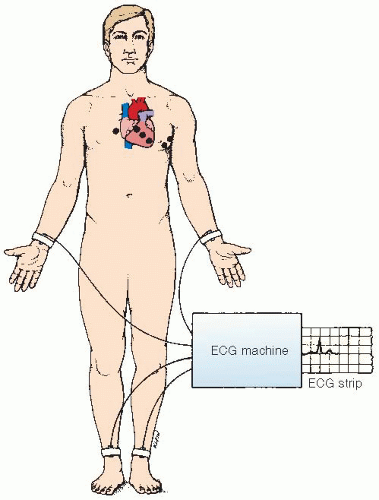
 NURSING ALERT
NURSING ALERT


