Cardiac disease is a factor in only 1% to 2% of pregnancies, yet it is now the leading cause of indirect pregnancy-related mortality in the United States. Indirect pregnancy-related mortality is defined as deaths from preexisting disease influenced by physiologic changes of pregnancy (Kuklina & Callaghan, 2011; Main, 2010). This trend has been detected in other developed countries, notably the United Kingdom and the Netherlands (Main, 2010). Approximately 10% to 25% of pregnancy-related deaths in the United States are associated with cardiac disease (Foley, Rokey, & Belfort, 2010). The prominence of cardiac disease in maternal mortality and morbidity is attributed to several factors. More women with congenital heart disease (CHD) are reaching childbearing age. Lifestyle trends such as delaying pregnancy until later in life, sedentary routine, obesity, and tobacco use all play a contributory role. The presence of other chronic medical conditions such as diabetes in conjunction with cardiac disease also increases the risk of complications during pregnancy (Bowater & Thorne, 2010; Harris, 2011; Jastrow et al., 2011; Kuklina & Callaghan, 2011). The conditions and complications described above, individually or in combination, place an additional burden on the cardiac muscle during pregnancy, labor, and birth, leading to increased risk.
The incidence of women with cardiac disease in the United States has not changed significantly since 1995; however, the morbidity of pregnant women hospitalized with cardiac disease appears to be increasing (Kuklina & Callaghan, 2011). A cross-sectional review of over 47,800,000 intrapartum and postpartum hospitalizations from across the United States during the years of 1995 to 2006 was undertaken to examine the prevalence of chronic heart disease and to approximate the impact of chronic heart disease on severe obstetric morbidity. Steady increases were seen in CHD, valvular disease from rheumatic fever, cardiomyopathy and/or congestive heart failure (CHF), and cardiac arrhythmias (Kuklina & Callaghan, 2011). Examination of ICD-9-CM codes for CHD revealed more reports of septal defects, circulatory abnormalities, and valvular disorders while nonspecific congenital disease decreased (Kuklina & Callaghan, 2011). The incidence of cardiac arrest, sepsis, and fluid/electrolyte abnormalities all increased during intrapartum hospitalizations. The number of postpartum hospitalizations tripled, with CHD and cardiac arrhythmias/conduction disorders showing significant increases (Kuklina & Callaghan, 2011).
The impact of maternal cardiac function on the fetus and neonate has also been examined. In a study about the effect of maternal cardiac disease on fetal growth and neonatal outcomes, 331 women with cardiac disease were compared to 662 women without cardiac disease (Gelson et al., 2011). Both groups had similar incidence of maternal hypertension and illicit drug and tobacco use. Perinatal complications in the group with cardiac disease were 50% higher than the control group. The most common complications were small-for-gestational-age neonates and preterm birth. No difference in preterm premature rupture of membranes was seen between the two groups. Maternal characteristics most associated with fetal and neonatal adverse outcomes were decreased cardiac output, cyanosis, or a combination of the two (Gelson et al., 2011).
Earlier studies have also demonstrated the effect reduced maternal cardiac function has on fetal growth. Twenty cases of singleton pregnancies with severe fetal growth restriction were compared to 107 normal singleton pregnancies (Bamfo, Kametas, Turan, Khaw, Nicolaides, 2006). Two-dimensional and M-mode echocardiography was used to evaluate maternal cardiac function in both groups. Reduction in cardiac output and stroke volume was seen along with an increase in systemic vascular resistance in the group with severe fetal growth restriction as compared to pregnancies with normal fetal growth (Bamfo et al., 2006). Another study compared 302 pregnancies with cardiac disease to 572 pregnancies without cardiac disease for neonatal complications (Siu et al., 2002). Neonatal complications included small for gestational age (SGA), preterm birth, respiratory distress, intraventricular hemorrhage, and fetal or neonatal death. Neonatal complications occurred over 50% more often in the group with cardiac disease. The subgroup with the highest neonatal complication rate included women with cardiac disease who had the following characteristics: younger than 20 years or older than 35 years, obstetric risk factors, multiple gestation, smoker, anticoagulant therapy, and at least one cardiac risk factor present (Siu et al., 2002).
Despite the significantly increased risk of adverse outcomes, most pregnant women with cardiac disease do well. Careful planning and monitoring prior to, during, and after the pregnancy by an interdisciplinary healthcare team increases the likelihood that the best possible outcome will occur for the mother and baby (Arafeh & Baird, 2006). All members of the team need to possess a thorough understanding of normal cardiac anatomy and physiology, knowledge of how the physiologic changes of pregnancy will influence cardiac function and the mother’s cardiac disease, the ability to estimate the risk pregnancy poses to the mother and her baby, and the ability to use the most recent and best knowledge to plan comprehensive care for the duration of the pregnancy, including follow-up in the postpartum period until the effects of pregnancy have resolved.
CARDIOVASCULAR PHYSIOLOGY
ANATOMY
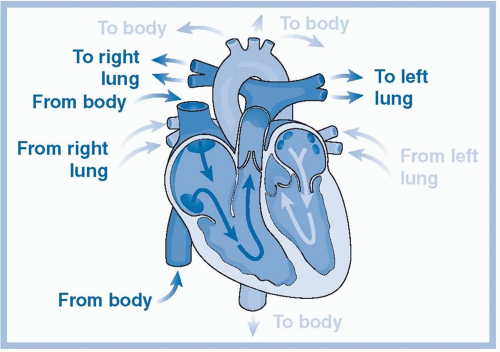
The purpose of the cardiovascular system is to deliver nutrient-rich oxygenated blood and remove waste products in response to the metabolic needs of the body (Darovic, 2002a). The cardiovascular system functions with three components: the heart, an electrical conduction system, and a vascular distribution network. The heart has four muscular chambers: two atria or upper chambers and the lower chambers or ventricles. Chamber walls have three layers: the pericardium or sac that surrounds the heart, the myocardium or the muscular layer, and the endocardium or inner lining of the chambers, which forms the valves of the heart (Darovic, 2002a). Although considered one organ, the heart functions as two pumps. The right side of the heart pumps deoxygenated blood to the lungs from the venous circulation (i.e., venous return → right atrium → right ventricle → pulmonary artery → pulmonary capillaries → pulmonary vein) (Blackburn, 2007). The left side of the heart receives oxygenated blood from the lungs and pumps it back to the systemic circulation (i.e., pulmonary vein → left atrium → left ventricle → aorta → systemic circulation) (Blackburn, 2007; Torgersen & Curran, 2006). There are four valves located in the heart that allow only forward flow when functioning normally. The two valves that connect the upper and lower chambers of the heart are called atrioventricular valves. The mitral valve is located on the left side of the heart, and the tricuspid valve is located on the right side. Semilunar valves attach the ventricles on each side of the heart to the large arteries they pump into; the pulmonic valve joins the right ventricle and pulmonary artery, and the aortic valve joins the left ventricle and the aorta. Figure 9-1 offers a conceptualization of the conduit of flow through the heart.
Once blood enters the systemic circulation, a fine meshwork of arteries and veins transport blood through the body. Arteries are muscular vessels that regulate blood flow based on cellular metabolic requirements. Veins return blood back to the heart and serve as a reservoir for as much as 70% of the circulating blood volume. Dilation or constriction of the venous bed occurs to accommodate the needs of the circulatory system. For example, in circumstances of low circulating blood volume, constriction of the veins can redistribute volume to augment circulation (Darovic, 2002a). Capillaries are thin-walled vessels with a large cross-sectional area where transfer of nutrients and metabolic waste occurs (Blackburn, 2007). The capillaries also regulate the distribution of extracellular fluid.
The conduction system in the cardiac muscle induces regular coordinated contractions between the upper and lower chambers of the heart to help optimize forward flow of blood. The sinoatrial (SA) node is in the right atria and is established as the primary pacemaker of the heart, initiating and setting the pulse (Blackburn, 2007). The atrioventricular node offers backup if conduction through the SA node is impaired or damaged. The heart is innervated or stimulated by the autonomic nervous system (i.e., sympathetic and parasympathetic nervous systems). Nerve receptors in the heart are stimulated by the release of epinephrine and norepinephrine from the sympathetic nervous system. Stimulation of beta-adrenergic receptors results in an increase in discharge from the SA node, augments the automaticity of cells in the heart, and improves contractility of the atria and ventricles (Darovic, 2002a). During pregnancy, the occurrence of arrhythmias is more frequent regardless of the presence of heart disease. For example, approximately 1.3% of women without heart disease will experience sustained supraventricular tachycardia during pregnancy (Szumowski et al., 2010).
Table 9-1. NORMAL PHYSIOLOGIC CHANGES OF PREGNANCY
Body System
Change
Cardiovascular System
Total blood volume
Increased 30%-50% (1,450-1,750 mL)
Plasma volume
Increased 40%-60% (1,200-1,600 mL)
Red cell volume
Increased 20%-32% (250-450 mL)
Cardiac output
Increased 40%-45% (positional)
Heart rate
Increased 15%-20% (10-20 bpm)
Systolic blood pressure
Unchanged (dependent on patient position and gestation of pregnancy)
Diastolic blood pressure
Decreased 10-15 mm Hg 24-32 weeks
Systemic vascular resistance
Decreased 20%-30%
Central venous pressure
Unchanged
Pulmonary capillary wedge pressure
Unchanged
Ejection fraction
Unchanged
Left ventricular stroke work index
Unchanged
Uterine blood flow
Increased 20%-40% depending on gestation
Respiratory System
Minute ventilation
Increased 30%-50%
Alveolar ventilation
Increased 50%-70%
Tidal volume
Increased 30%-40% (500-700 mL)
Respiratory rate
Unchanged
Functional residual capacity
Decreased 20%-30%
Residual volume
Decreased 20%-30%
Oxygen consumption
Increased 20% (up to 60% increase during labor)
Arterial pH
Slightly increased (average 7.40-7.45)
PaO2 (mm Hg)
Increased (101-104 mm Hg)
PaCO2 (mm Hg)
Decreased (27-32 mm Hg)
Renal System
Renal blood flow
Increased 50% (by fourth month)
Glomerular filtration rate
Increased 50% (by fourth month)
Upper limit of blood urea nitrogen
Decreased 50%
Upper limit of serum creatinine
Decreased 50%
Hepatic System
Total plasma protein concentration
Decreased 20%
Pseudocholinesterase concentration
Decreased
Coagulation factors
Variable
Gastrointestinal System
Gastric emptying
Delayed
Gastric fluid volume
Unchanged
Gastroesophageal sphincter tone
Decreased
Data from Bobrowski, R. A. (2010) . Maternal-fetal blood gas physiology. In M. Belfort, G. Saade, M. Foley, J. Phelan, & G. Dildy (Eds.), Critical Care Obstetrics (5th ed., pp. 53-68 ). Oxford, UK: Wiley-Blackwell; Norwitz, E. R., & Robinson, J. N. (2010) . Pregnancy-induced physiologic alterations. In M. Belfort, G. Saade, M. Foley, J. Phelan, & G. Dildy (Eds.), Critical Care Obstetrics (5th ed., pp. 30-52 ). Oxford, UK: Wiley-Blackwell.
The cardiovascular system undergoes tremendous physiologic change during pregnancy to support the growing fetus and prepare the mother for birth. The tissues of the heart go through a remodeling process during pregnancy that results in enlargement or hypertrophy and expansion of the capillary bed to supply adequate oxygenation for the increased workload. These changes are similar to those seen with endurance training (Cruz, Briller, & Hibbard, 2010; Vitarelli & Capotosto, 2011). Other systems in the body also experience significant physiologic changes. See Table 9-1 for a summary of the major changes associated with normal pregnancy.
HEMODYNAMICS AND CARDIAC OUTPUT
The movement of blood through the body is essential for life. A major component of the movement of blood or hemodynamics is cardiac output. Cardiac output can be defined as the amount of blood pumped through the heart and is measured in liters per minute (Darovic, Graham, & Pranulis, 2002). Cardiac output is determined by four variables: preload, afterload, contractility, and heart rate. Normal hemodynamic values in pregnancy are listed in Table 9-2. Preload is the volume of blood in the ventricle or tension placed on the myocardial fibers as contraction begins at end-diastole. Preload is primarily influenced by circulating blood volume available to fill the ventricle (Darovic, 2002b). If the volume of blood returning to the heart is diminished, as in hypotension, the subsequent decrease in preload reduces cardiac output. The cardiac muscle has the intrinsic ability to respond to variances in filling pressures, which allows for healthy adaptation to stress. This adaptation is challenged by the 2 to 3 L/min and 40% to 50% overall rise in cardiac output during pregnancy (Bonow et al., 2006). A commensurate increase in cardiac output usually peaks between the midportion of the second and third trimesters (Bonow et al., 2006). Preload is reported as central venous pressure in the right side of the heart and as pulmonary capillary wedge pressure in the left side of the heart (Darovic, 2002b; Darovic & Kumar, 2002).
Afterload is defined as the resistance the ventricle has to overcome to eject blood during systole (Darovic, 2002b). Afterload the right ventricle pumps against is expressed by pulmonary artery pressure or pulmonary vascular resistance. Systemic vascular resistance or the patient’s blood pressure provides afterload to the left ventricle. During pregnancy, the influence of progesterone is thought to decrease peripheral vascular resistance, thereby decreasing afterload. As a result, a drop in blood pressure during the second trimester is a common finding (Norwitz & Robinson, 2010).
Table 9-2. NORMAL HEMODYNAMIC VALUES IN LATE PREGNANCY
Parameter
Value and Standard Deviation
Cardiac output (L/min)
6.2 ± 1.0
Systemic vascular resistance (dyne/sec/cm-5)
1,210 ± 266
Pulmonary vascular resistance (dyne/sec/cm-5)
78 ± 22
Mean arterial pressure (mm Hg)
90 ± 6
Pulmonary capillary wedge pressure (mm Hg)
8 ± 2
Central venous pressure (mm Hg)
4 ± 3
Left ventricular stroke index (g/m/m-2)
48 ± 6
Data from Norwitz, E. R., & Robinson, J. N. (2010) . Pregnancy-induced physiologic alterations. In M. Belfort, G. Saade, M. Foley, J. Phelan, & G. Dildy (Eds.), Critical Care Obstetrics (5th ed., pp. 30-52 ). Oxford, UK: Wiley-Blackwell.
Contractility is an independent intrinsic ability of the cardiac muscle to shorten aside from influences by preload and afterload (Darovic, 2002b). Contractility is measured indirectly by the left ventricular stroke work index. Heart rate is the final component of cardiac output. The speed at which the cardiac muscle pumps can influence output either positively or negatively. Excessively high heart rates lead to a decrease in filling time of the ventricles and reduction in output. Typically during trauma, dysfunction, or disease, the human heart will alter heart rate (i.e., pulse) prior to detectable influences on any of the other remaining parameters (Belfort, Saade, Foley, Phelan, & Dildy, 2010). In cases of severe hypovolemia, the heart rate may rise appreciably before changes in the peripheral vascular resistance (i.e., blood pressure) are evident. Therefore, blood pressure and pulse are two vital signs reflective of cardiac output and cardiac disease. As a result, accuracy of assessment for both parameters and careful evaluation of trends is a key part of thorough patient assessment.
CARDIAC ADAPTATIONS OF PREGNANCY
Normal pregnancies may precipitate signs and symptoms of dizziness, dyspnea, orthopnea, fatigue, syncope, rales in the lower lung fields, jugular vein distention, systolic murmurs, dysrhythmias, and cardiomegaly (Blanchard & Shabetai, 2004; Torgersen & Curran, 2006). For this reason, it can be difficult to determine whether symptoms experienced by the mother are normal changes found in pregnancy or an indication of cardiac disease. Table 9-3 outlines normal cardiac changes during pregnancy compared to abnormal signs and symptoms of cardiac disease. Symptoms indicative of heart disease include severe dyspnea; syncope with exertion; hemoptysis; paroxysmal nocturnal dyspnea; cyanosis; clubbing; diastolic murmurs; sustained cardiac arrhythmias; loud, harsh systolic murmurs; and chest pain with exertion (Blanchard & Shabetai, 2004). Prompt intervention is warranted if signs or symptoms abnormal for pregnancy are present.
The physiologic changes of pregnancy that tend to be problematic for women with cardiac disease include the increase in blood volume, decrease in systemic vascular resistance, the hypercoagulable state of pregnancy, and fluctuations in cardiac output (Foley et al., 2010). The increase in blood volume may be problematic for women with stenotic heart valves, impaired ventricular function, or congenital artery disease. The inability of the heart to handle the extra volume can lead to failure or an ischemic event. In diseases associated with weakened arterial vessels such as Marfan syndrome or coarctation, the pressure from extra blood volume may cause an aneurysm or dissection (Curry, Swan, & Steer, 2009; Foley et al., 2010).
Table 9-3. NORMAL PREGNANCY SYMPTOMS VERSUS SYMPTOMS OF CARDIAC DISEASE
Pregnancy: May Be Present
Cardiac Disease from Any Cause: May Be Present
Fatigue
Exertional dyspnea (usually limited to third trimester)
Irregular or infrequent syncope
Palpations (brief, irregular, and asymptomatic)
Jugular venous distention
Mild tachycardia <15% rise
Third heart sound
Grade II/VI systolic murmur
Pedal edema
Decreased ability to perform activities of daily living
Severe breathlessness, orthopnea, paroxysmal nocturnal dyspnea, cough, or syncope
Chest pain (not normal in pregnancy)
Systemic hypotension
Cyanosis, clubbing
Persistent jugular venous distention
Sinus tachycardia >15% normal heart rate
Fourth heart sound
Ventricular murmurs
Pulmonary edema
Pleural effusion
Data from Curran, C. (2002) . Multiple organ dysfunction syndrome (MODS) in the obstetrical population. Journal of Perinatal & Neonatal Nursing, 15(4), 37-55; Thorne, S. A. (2004) . Pregnancy in heart disease. Heart, 90(4), 450-456. doi:10.1136/hrt.2003.027888
Decrease in systemic vascular resistance is problematic for women with abnormal connections between the right and left heart or shunts. Typically, the left side of the heart is under higher pressure than the right side of the heart due to the task of pumping blood to the large systemic circulation against the pressure of the systemic vascular resistance. In this situation, oxygenated blood will shunt through defects between the two sides of the heart from the left side to the right side. In the short term, this can be tolerated by the heart and the body as oxygenated blood is being recirculated through the lungs. When the systemic vascular resistance drops in pregnancy, this dynamic can change, with potential for blood to shunt from the right side of the heart to the left. In this case, deoxygenated blood is contributing to cardiac output, ultimately resulting in decreased oxygen content in arterial blood (Foley et al., 2010).
The hypercoagulable state of pregnancy increases the risk of clot formation for women with artificial heart valves and some forms of arrhythmia. Particularly in atrial fibrillation, blood can collect and clots can form in the atria due to ineffective emptying from the lack of coordinated atrial and ventricular contractions. The need to achieve anticoagulation can increase the risk of postpartum hemorrhage following birth (Foley et al., 2010). Finally, the dynamic changes in cardiac output throughout pregnancy can precipitate a crisis when disease is present that requires a constant amount of blood volume to maintain output, as in pulmonary hypertension, or when the cardiac output is fixed, as in mitral stenosis.
During pregnancy, cardiac output steadily increases until it is nearly double. The following changes in cardiac output occur during the active phase of labor: increases 17% at ≤3 cm dilated, 23% from 4 to 7 cm dilated, and 34% at ≥8 cm dilated (Blackburn, 2007). Uterine contractions may enhance cardiac output by as much as 15% to 20% due to the increased metabolic demands (Barth, 2009; Belfort et al., 2010). Uterine contractions can result in marked increases in both systolic and diastolic blood pressure (Bonow et al., 2006). The first 15 minutes following evacuation of the uterus at birth includes a return of approximately 600 to 800 mL of uterine blood to the maternal vascular compartment. Therefore, immediate postpartum is one of the most stressful times (from the standpoint of the cardiovascular system) of all pregnancy, labor, and birth, with a 65% maximum increase in cardiac output (Blackburn, 2007; Foley et al., 2010).
OBSTETRIC OUTCOMES AND ASSESSMENT OF RISK
When the woman with cardiac disease presents prenatally or ideally for preconception counseling, estimating the risk pregnancy and birth poses to her and her baby is an important part of counseling and developing a plan of care. Risk may occur from cardiac disease as well as other factors such as obesity, tobacco use, and presence of other chronic disease states. Assessment of the risk that cardiac disease presents can be evaluated by different methods. While it may seem redundant to routinely use each method, given the relative rarity of cardiac disease in pregnancy and lack of established guidelines to manage cardiac disease in pregnancy, it may be worthwhile to examine risk to the woman from the perspective of each method. The first method is the New York Heart Association (NYHA) Functional Classification (Table 9-4). This is the oldest of the three methods and is based on the functional ability of the person with cardiac disease, regardless of what that disease may be. The patient is assessed either by questioning or direct observation of symptoms in response to activity. Symptoms of interest include dyspnea, chest pain, and shortness of breath. This risk assessment is particularly helpful in pregnancy to document changes in functional status that are expected in response to the physiologic changes of pregnancy. Progression to a higher NYHA classification should prompt further evaluation due to the association with higher maternal mortality. Determining functional classification on a regular basis such as during prenatal visits, frequently during labor, and with each postpartum assessment can uncover a trend that may indicate a decline in status.
Table 9-4. NEW YORK HEART ASSOCIATION FUNCTIONAL CLASSIFICATION SYSTEM
Class
Description
I
Asymptomatic No limitation of physical activity
II
Asymptomatic at rest; symptomatic with heavy physical activity and exertion Slight limitation of physical activity
III
Asymptomatic at rest; symptomatic with minimal or normal physical activity Considerable limitation of physical activity
IV
Symptomatic at rest; symptomatic with any physical activity
Severe limitation of physical activity
American Heart Association, Inc. http://www.heart.org. Reprinted with permission.
DISPLAY 9-1 Mortality Risk Associated with Pregnancy
GROUP I: MORTALITY <1%
Atrial septal defect
Ventricular septal defect (uncomplicated)
Patent ductus arteriosus
Pulmonic and tricuspid disease
Corrected Tetralogy of Fallot
Biosynthetic valve prosthesis (porcine and human allograft)
Mitral stenosis, New York Heart Association (NYHA) Class I & Class II
Mortality risk can be estimated based on the type of lesion or disease present. In Display 9-1, cardiac disease is divided into three groups based on a combination of several risk estimates and appropriate management by a team knowledgeable in providing care to women with cardiac disease. Group I consists of lesions that generally have a low mortality rate. Group II have moderate risk of an adverse event with a higher mortality rate of 5% to 15%. The risk of complications is considerable in Group III, with an estimated mortality rate in excess of 25%. In the majority of cases, women who are in Group III may be counseled that the risk of achieving or continuing pregnancy is too great to consider (Foley et al., 2010).
In Display 9-2, Siu and colleagues (2001) offer additional guidance regarding potential risk of a cardiac event during pregnancy; 562 women with cardiac disease were followed during pregnancy to determine occurrence of cardiac events. Cardiac events were divided into two groups: primary and secondary. A primary cardiac event was defined as pulmonary edema, persistent symptomatic tachycardia or bradycardia necessitating treatment, stroke, cardiac arrest, or cardiac death. Secondary cardiac events included decrease in functional ability as defined by the NYHA classification and the need for emergent invasive cardiac procedures during pregnancy through 6 months postpartum (Siu et al., 2001). Four predictors of events were identified: previous cardiac complication or arrhythmia, presence of cyanosis or NYHA Class II or greater at the beginning of pregnancy, left heart obstruction, and decreased left ventricle function. As the number of predictors that are present increase, so does the risk of a cardiac event. If the patient’s cardiac history has all four predictors, then a healthcare provider should counsel the women to reconsider attempting pregnancy. It should also be noted that even with no predictors present, risk of having an event is assessed at 5% (Siu et al., 2001).
DISPLAY 9-2 Predictors of Cardiac Events
Prior cardiac event before pregnancy
Heart failure
Stroke or transient ischemic attack
Arrhythmia
New York Heart Association >Class II
Cyanosis
Obstruction left heart
Gradient >30 peak
Aortic valve <1.5 cm
Mitral valve prolapse <2 cm
Ejection fraction <40%
Number of predictors equals risk of cardiac events during pregnancy: 0 = 5%, 1 = 27%, >1 = 75%
Drenthen and colleagues (2010) used the risk assessment tool just described in 1,302 pregnancies complicated with CHD. Arrhythmias and heart failure were the most common cardiac events noted in this cohort. When comparing the risk assessment tool prediction to outcomes, it was found that risk was overestimated. The authors caution that use of a risk assessment tool be merely one part of a comprehensive evaluation of the woman and her specific cardiac disease (Drenthen et al., 2010). Other types of parameters may be used to determine risk. One such parameter is serum B-type natriuretic peptide (BNP). BNP levels increase in conjunction with worsening heart failure in nonpregnant cardiac patients under circumstances that are similar to pregnancy. A study of 78 pregnant women was conducted, 66 with heart disease and 12 without, that followed BNP levels throughout pregnancy. BNP levels were low throughout pregnancy in the group without heart disease. Elevations in BNP were not conclusively predictive of a cardiac event, but levels of less than 100 pg/mL in women with cardiac disease was found to have a negative predictive value of 100% (Tanous et al., 2010).
The risk of cardiac events late after birth can also be predicted. Balint and colleagues (2010) reviewed 405 pregnancies to determine characteristics predictive of cardiac events that occur more than 6 months after birth. Late events included cardiac arrest/death, pulmonary edema, arrhythmia, and stroke. Characteristics associated with late events were NYHA Class II or higher, presence of cyanosis, subaortic ventricular dysfunction, subpulmonary ventricular dysfunction, pulmonary regurgitation, left heart obstruction, and cardiac complications before pregnancy (Balint et al., 2010). Evaluation for these characteristics can assist in determining how long to carefully assess and hospitalize the woman after birth as well as how to direct home instructions and guide frequency of follow-up after discharge.
CONGENITAL HEART DISEASE IN PREGNANCY
CHD occurs in approximately 0.8% of live births (Harris, 2011). Advances in neonatal care and pediatric cardiac surgery have resulted in a significant improvement in survival rates for babies born with CHD, and 85% of these infants can be expected to survive to adulthood (Gelson, Gatzoulis, Steer, & Johnson, 2009; Kafka, Johnson, & Gatzoulis, 2006). As these infants are coming of age, more women are beginning pregnancy with medical histories of significant cardiac surgical repairs from CHD (Kafka et al., 2006). Women with congenital heart defects are at increased risk of passing the defect to the baby. Maternal conditions (e.g., diabetes, lupus erythematosus, phenylketonuria, drug abuse), medication ingestion (e.g., Lithium, alcohol), genetics, or infections (e.g., rubella, rheumatic fever, viruses) may also result in structural defects in the fetal heart (Blanchard & Shabetai, 2004).
Blood flow is critical to the development of cardiac structures during the embryonic period. If flow through cardiac structures is limited or absent, abnormal development occurs. If flow restriction occurs in early gestation during fetal cardiac development, the specific region and structures “downstream” will become small (hypoplastic) or even completely absent (atretic) (Linker, 2001). As a result, one of four structural defects may develop: hole (defect), narrowing due to stiffness causing obstruction (stenosis), underdevelopment or absence (hypoplasia or atresia), or wrong connection (transposition, inversion, anomalous connection) (Linker, 2001).
For ease of discussion, congenital lesions will be categorized as acyanotic, cyanotic, or aortic.
Only gold members can continue reading. Log In or Register to continue