 Evidence Base
Evidence Base
According to the American Cancer Society (ACS), 1,638,910 new diagnoses of invasive cancer were diagnosed in the United States in 2012. This did not include basal and squamous cell skin cancers as well as noninvasive cancers, or DCIS (ductal carcinoma in situ).
According to the International Agency for Research on Cancer, there were 12.7 million new cancer cases in 2008 worldwide. This number is expected to rise as developing countries adopt Western lifestyles such as smoking and lack of exercise.
Although the death rate continues to decline, cancer is the second leading, under heart disease, cause of death in the United States, with 577,190 predicted for 2012.
Age is the most outstanding risk factor for cancer.
Cancer incidence increases progressively with age.
Approximately 78% of people diagnosed with cancer are over age 55.
Two thirds of all cancers in the United States are related to lifestyle habits (eg, smoking, alcohol consumption, diet, physical activity) and environmental carcinogens.
Tobacco is the single greatest cause of cancer-related deaths and is attributed to more than 443,000 deaths annually from various cancers.
Excessive alcohol intake is associated with cancers of the mouth, larynx, throat, esophagus, and liver, especially when combined with smoking. In addition, regular consumption of alcohol is associated with an increased risk of breast cancer. This may be due to alcohol-induced increases in circulating estrogens.
Exposure to carcinogens, such as asbestos, benzene, and radiation, increases the risk of developing certain types of cancer.
Solar ultraviolet radiation exposure is related to an increased risk of skin cancers.
There is a hereditary predisposition to specific forms of cancers that have been linked to certain events within a gene (eg, BRCA1 and BRCA2 in breast cancer; MLH1, MSH2, and MSH6 in colon cancer).
Infections and viruses are associated with an increased risk of certain forms of cancer.
Human papilloma virus (HPV)—cervical cancer, anal cancers, upper airway cancers.
Epstein-Barr virus—lymphoma, nasopharyngeal cancers, gastric cancer, Kaposi’s sarcoma.
Cytomegalovirus—Kaposi’s sarcoma, colon cancer.
Human immunodeficiency virus (HIV)—Kaposi’s sarcoma, lymphoma.
Human T-lymphocyte virus—T-cell lymphoma/leukemia.
Hepatitis B and C—hepatocellular cancer.
Helicobacter pylori—gastric lymphoma (possibly).
Five-year survival rates are increasing with improved therapy and earlier detection.
Ongoing genetic research is searching for the ability to correct and modify hereditary susceptibility.
Patterns of incidence and death rates vary with sex, age, race, and geographic location (see Table 8-2).
Table 8-1 Differences Between Malignant and Benign Tumors | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
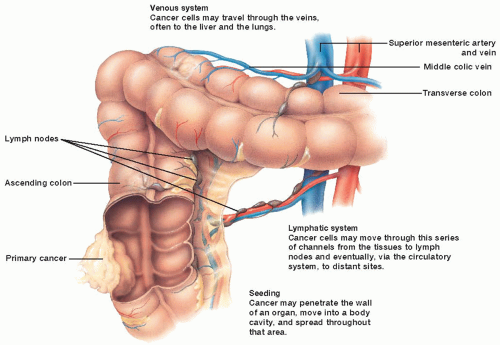 Figure 8-1. How cancer spreads. Cancer cells may invade nearby tissues or metastasize (spread) to other organs. Cancer cells may move to other tissues by any or all of three routes: venous, lymphatic, or seeding. |
 Evidence Base
Evidence BaseTable 8-2 Leading New Cancer Cases and Deaths – 2012 Estimates | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Diet does influence the risk of cancer. Among nonsmokers, dietary choices and physical activity are the most important modifiable risks of cancer. The ACS has established guidelines on nutrition and physical activity to promote optimal health and prevent cancer. These recommendations are consistent with the USDA 2010 Dietary Guidelines for Americans.
Maintain healthy weight.
Balance calorie intake with physical activity.
Avoid excessive weight gain.
Achieve and maintain a healthy weight if currently overweight or obese.
Adopt a physically active lifestyle.
Adults should engage in 150 minutes of moderate intensity or 75 minutes of vigorous activity each week, preferably spread throughout the week.
Children and adolescents should engage in 60 minutes per day of moderate to vigorous physical activity at least 5 days per week.
Eat a healthy diet with an emphasis on plant sources.
Choose foods and drinks in amounts that help achieve and maintain a healthy weight.
Eat five or more servings of a variety of vegetables and fruits daily.
Choose whole grains over processed (refined) grains.
Limit intake of processed and red meats.
Limit alcoholic beverages to no more than 2 drinks per day for men and 1 drink per day for women.
ACS recommendations for community action:
Increase access to healthful foods in schools, worksites, and communities.
Provide safe, enjoyable spaces for physical activity in schools.
Provide for safe, physically active transportation (such as biking and walking) and recreation in communities.
Table 8-3 ACS Recommendations for the Early Detection of Cancer in Average-Risk, Asymptomatic Individuals | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Make appropriate lifestyle changes.
Stop smoking.
Limit alcohol intake.
Eat a healthy diet as outlined above.
Be physically active: maintain a healthy weight and follow exercise guidelines outlined above.
Avoid sun exposure, especially during the hours of 10 a.m. and 4 p.m. and cover exposed skin with sunscreen with a skin protection factor of 15 or higher.
Those at high risk for certain cancers should consider genetic counseling and testing.
Chemoprevention—the use of natural or synthetic substances to reduce the risk of developing cancer.
Aspirin—doses of at least 75 mg daily can decrease the risk of colorectal cancer.
Tamoxifen and raloxifene—can reduce the risk of breast cancer in women who are at high risk by nearly 50%.
Finasteride—may reduce the risk of prostate cancer.
COX-2 inhibitors—may reduce the risk colorectal cancer.
Vitamin D—may play a role in reducing the risk of breast cancer.
Statins—may reduce the risk of prostate, lung, colorectal, and breast cancers.
Vaccinations—HPV is now known to cause about 70% of cervical cancers. HPV vaccines are aimed at preventing genital warts, precancerous cervical lesions, cervical cancer, and anal, penile, and oropharyngeal cancers in both men and women. The Advisory Committee on Immunization Practices in conjunction with the Centers for Disease Control and Prevention has established guidelines on the use of this vaccine.
Routine HPV vaccination is recommended for males and females ages 11 to 13, may begin as early as age 9.
HPV vaccination is also recommended for males and females ages 13 to 18 to “catch up” missed doses of the vaccine or complete the vaccination series.
HPV vaccination is not currently recommended for persons over age 26.
Screening for cervical cancer should continue in both vaccinated and unvaccinated women according to current ACS early detection guidelines.
 Evidence Base
Evidence Base Evidence Base
Evidence Base
The goal of screening is early detection to improve overall outcome and survival. Performing routine screening tests should be based on whether these tests are adequate to detect a potentially curable cancer in an otherwise asymptomatic person and are also cost-effective.
Screening should be based on an individual’s age, sex, family history of cancer, ethnic group or race, previous iatrogenic factors (prior radiation therapy or drugs such as DES), and history of exposure to environmental carcinogens. See Table 8-3 for ACS recommendations for screening.
The ACS has not issued guidelines for detection of early lung cancer in asymptomatic individuals, but it does recognize that patients at high risk may decide to undergo testing. Currently, the National Comprehensive Cancer Network recommends lung cancer screening in high-risk individuals using low-dose computed tomography (CT). High-risk individuals are men or women age 55 to 74 with at least a 30 pack per year history of smoking and smoking cessation for less than 15 years; or men or women at least 50 years old with a 20 or more pack per year history of smoking and one additional risk factor.
The ACS recommends that men, starting at age 50, make an informed decision with their health care providers about whether to be tested for prostate cancer. Research has not yet proven that the potential benefits of testing outweigh the harms of testing and treatment. The ACS position is that men should not be tested without learning about what we know and don’t know regarding the risks and possible benefits of testing and treatment.
 Evidence Base
Evidence Base
Complete medical history and physical examination.
Biopsy of tumor site to determine pathologic diagnosis. Biopsy results are used to determine the histology and/or grade of a tumor, which is a prerequisite for planning definitive therapy.
Fine-needle aspiration (FNA)—technique in which cells are aspirated from the tumor using a needle and syringe. FNA cannot distinguish invasive from noninvasive malignancy. Negative results do not rule out malignancy. However, it is inexpensive, causes little discomfort, and can be performed in an outpatient or office setting.
Needle core—needle biopsies are performed with a largebore needle. This technique retrieves a small piece of intact tumor tissue, which yields enough tissue to adequately
diagnose most tumor types. It is highly accurate and can be performed in an office or outpatient setting.
Open biopsy— may be required for some lesions to determine a definitive diagnosis. This is done in the operating room, is more expensive, and requires a longer period of recovery. The biopsy may be incisional, sampling only part of the tumor, or excisional, removing the total tumor.
Classification of tumor type is based on tissue and cellular staining. Differences in cytoplasmic and nuclear staining distinguish one cell type from another and identify their stage of differentiation. The grade of the tumor (rating of 1 to 4) is based on how well differentiated the tissue or cells appear. For most tumors the higher the grade, the less differentiated, which is associated with poorer prognosis.
Flow cytometry testing of tumor tissue determines the deoxyribonucleic acid (DNA) content and indicates potential risk of recurrence.
Special stains are performed to determine specific markers or proteins that may help guide treatment (ie, estrogen and progesterone receptors for breast cancer).
Laboratory tests—including complete blood count (CBC) with differential; platelet count; and blood chemistries, including liver function tests, blood urea nitrogen (BUN), and creatinine—are done to determine baseline values.
Further testing depends on cancer diagnosis.
Blood markers (carcinoembryonic antigen, PSA, CA15-3, CA125) may be appropriate to follow response to therapy.
Imaging procedures—chest x-ray, nuclear medicine scan, CT scanning, magnetic resonance imaging (MRI), and positronemission tomography (PET) are used to determine evidence or extent of metastasis.
The American Joint Committee on Cancer (AJCC) has developed a simple classification system that can be applied to all tumor types. It is a numeric assessment of tumor size (T), presence or absence of regional lymph node involvement (N), and presence or absence of distant metastasis (M) (see Box 8-1).
No standard evaluation exists for all cancers. Workup depends on the patient, tumor type, symptoms, and medical knowledge of the natural history of that cancer.
Preventive/prophylactic surgery—removal of lesions that, if left in the body, are at risk of developing into cancer; for example, resection of polyps in the rectum or mastectomy in women who are at high risk.
Primary surgery—complete surgical removal of a malignant tumor and may include regional lymph nodes and neighboring structures. This can be performed laparoscopically in some cases.
Cytoreductive surgery—partial removal of bulk of disease. This is performed when the spread of tumor precludes the removal of all disease. In some cases, this approach improves survival when used in combination with chemotherapy (ie, ovarian cancer).
Salvage treatment—use of an extensive surgical approach to treat a local recurrence.
Palliative treatment—attempts to relieve the complications of cancer (eg, obstruction of the GI tract, pain produced by tumor extension into surrounding nerves).
Reconstructive/rehabilitative surgery—repair of defects from previous radical surgical resection; can be performed early (breast reconstruction) or delayed (head and neck surgery).
The intent of chemotherapy is to destroy as many tumor cells as possible with minimal effect on healthy cells.
Cancer cells depend on the same mechanisms for cell division as normal cells. Damage to those mechanisms leads to cell death.
Chemotherapy is utilized in different clinical settings:
Adjuvant chemotherapy is the use of systemic treatment following surgery and/or radiation therapy. Adjuvant therapy is given to patients who have no evidence of residual disease but who are at high risk for relapse. The justifications for adjuvant chemotherapy are the high recurrence rate after surgery for apparently localized tumors, the inability to identify cured patients at the time of surgery, and the failure of therapy to cure these patients after recurrence of disease.
Neoadjuvant chemotherapy is the use of systemic treatment prior to primary surgery or radiation. The goal is to shrink or downstage the primary tumor to improve the effectiveness of surgery as well as control/irradicate microscopic cancer cells. For example, patients with large breast tumors can preserve the breast and undergo lumpectomy instead of mastectomy. The goal of therapy is to decrease the amount of tissue that needs to be removed as well as to attempt to maximize cure potential.
High-dose/intensive therapy is the administration of high doses of chemotherapy, usually in association with growth factor support before bone marrow transplant/stem cell rescue.
Palliative chemotherapy is used when a cure is not possible to control the cancer and minimize side effects from the disease.
Chemotherapeutic agents can be effective on any stage of the cell cycle in which cells are dividing. The cell cycle is divided into five stages:
G0 (gap 0) resting phase: Cells are not dividing in this stage and, for the most part, are refractory to chemotherapy.
G1 (gap one) phase: Ribonucleic acid (RNA) and protein synthesis (enzymes for DNA synthesis) are manufactured.
S (synthesis) phase: During a long period, the DNA component doubles for the chromosomes in preparation for cell division.
G2 (gap two) phase: This is a short period; protein and RNA synthesis occurs, and the mitotic spindle apparatus is formed.
M (mitosis) phase: In an extremely short period, the cell divides into two identical daughter cells.
Routes of administration:
Oral—capsule, tablet, or liquid.
Intravenous (IV)—push (bolus) or infusion over a specified period.
Intramuscular.
Intrathecal/intraventricular—given by injection via an Ommaya reservoir or by lumbar puncture.
Intra-arterial.
Intracavitary—such as peritoneal cavity.
Intravesical—into uterus or bladder.
Topical.
Dosage is based on surface area (mg/m2) in both adults and children.
Most chemotherapeutic agents have dose-limiting toxicities that require nursing interventions (see Table 8-4, pages 142 to 145). Chemotherapy predictably affects normal, rapidly growing cells (eg, bone marrow, GI tract lining, hair follicles). It is imperative that these toxicities be recognized early by the nurse.
 Evidence Base
Evidence Base
Gloves—wear gloves that are powder-free, such as nitrile, polyurethane, or neoprene, and have been tested for use with hazardous drugs. Avoid latex drugs due to potential latex sensitivity. Double gloves are recommended for all handling.
Gowns—wear a disposable, lint-free gown made of low-permeability fabric. The gown should have a solid front, long sleeves, tight cuffs, and back closure. The inner glove should be worn under the gown cuff and the outer glove should extend over the gown to protect the skin. Gown and gloves are meant for single use only.
Respirators—wear a National Institute for Occupational Health and Safety approved respirator mask when there is a risk of aerosol exposure such as when administering chemotherapy or cleaning a spill. Surgical masks do not provide adequate protection.
Eye and face protection—wear a face shield and/or mask that provides splash protection whenever there is a possibility of splashing.
Wear personal protective equipment whenever there is a risk of chemotherapy being released into the environment such as preparation or mixing of chemotherapy, spiking/priming IV tubing, administering the drug, and when handling body fluids or chemotherapy spills.
Prepare cytotoxic drugs in a vertical laminar flow hood.
Wash hands before donning PPE and change gloves after each use, tear, puncture, or medication spill or after every 60 minutes of wear. Wash hands after removing PPE.
Vent vials with filter needle to equalize the internal pressure or use negative-pressure techniques.
Wrap gauze or alcohol pads around the neck of ampules when opening to decrease droplet contamination.
Wrap gauze or alcohol pads around injection sites when removing syringes or needles from IV injection ports.
Use puncture- and leak-proof containers for noncapped, nonclipped needles.
Prime all IV tubing with normal saline or other compatible solution to reduce exposure.
Use syringes and IV tubing with luer locks (which have a locking device to hold needle firmly in place).
Label all syringes and IV tubing containing chemotherapeutic agents as hazardous material.
Place an absorbent pad directly under the injection site to absorb any accidental spillage.
Do not eat, drink, or chew gum while preparing or handling chemotherapy agents.
Keep all food and drink away from preparation area.
Avoid hand-to-mouth or hand-to-eye contact while handling chemotherapeutic agents or body fluids of the patient receiving chemotherapy.
If any contact with the skin occurs, immediately wash the area thoroughly with soap and water.
If contact is made with the eye, immediately flush the eye with water and seek medical attention.
Spill kits should be available in all areas where chemotherapy is stored, prepared, and administered.
Discard gloves and gown into a leak-proof container, which should be marked as contaminated or hazardous waste.
Use puncture- and leak-proof containers for needles and other sharp or breakable objects.
Linens contaminated with chemotherapy or excreta from patients who have received chemotherapy within 48 hours should be contained in specially marked hazardous waste bags.
Wear nonsterile nitrile gloves for disposing of body excreta and handling soiled linens within 48 hours of chemotherapy administration.
In the home, wear gloves when handling bed linens or clothing contaminated with chemotherapy or patient excreta within 48 hours of chemotherapy administration. Place linens in a separate, washable pillow case. Wash separately in hot water and regular detergent.
Most chemotherapeutic agents cause some degree of alopecia. This is dependent on the drug dose, half-life of drug, and duration of therapy.
Usually begins 2 weeks after administration of chemotherapy. Regrowth takes about 3 to 5 months.
The use of scalp hypothermia and tourniquets is highly controversial.
Chemotherapy changes the reproduction of taste buds.
Absent or altered taste can lead to a decreased food intake.
Concurrent renal or hepatic disease can increase anorexia.
Defined as loose or watery stool. If left untreated, can lead to severe dehydration, electrolyte imbalances, hospitalizations, and treatment delays.
Cause is multifactoral, but up to 90% of all patients receiving chemotherapy can experience diarrhea.
Caused by the stimulation of the vagus nerve by serotonin released by cells in the upper GI tract.
Incidence depends on the particular chemotherapeutic agent and dosage.
Patterns of nausea and vomiting:
Anticipatory—conditioned response from repeated association between therapy and vomiting; can be prevented with adequate anti-emetic control.
Acute—occurs 0 to 24 hours after chemotherapy administration.
Delayed—can occur 1 to 6 days after chemotherapy administration; nausea is often worse than vomiting.
Caused by the destruction of the oral mucosa, causing an inflammatory response.
Initially presents as a burning sensation with no changes in the mucosa and progresses to significant breakdown, erythema, and pain of the oral mucosa.
Consistent oral hygiene is important to avoid infection.
Defined as an absolute neutrophil count (ANC) of 1,500/mm3 or less.
Primary dose-limiting toxicity of chemotherapy.
Risk of infection is greatest with an ANC less than 500/mm3.
Caused by suppression of the stem cell.
Usually occurs 7 to 14 days after administration of chemotherapy, but depends on the agent used.
Can be prolonged.
Patients should be taught to avoid infection through proper handwashing and hygiene and avoiding those with illness. Eliminating raw meats, seafood, eggs or unwashed vegetables is also recommended
Patients need to be monitored and treated promptly for fever or other signs of infection.
Can be prevented with the use of growth factors (eg, granulocyte colony-stimulating factor [CSF], pegfilgrastim).
Caused by suppression of the stem cell or interference with cell proliferation pathways.
May require red blood cell transfusion or injection of erythropoietin or darbepoetin.
Table 8-4 Frequently Used Chemotherapeutic Agents | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|



