Chapter 16 Assisted vaginal delivery and shoulder dystocia
INDICATIONS FOR INSTRUMENTAL ASSISTED VAGINAL DELIVERIES
The incidence of instrumental vaginal delivery should be between 8% and 10% of births.
REQUIREMENTS FOR ASSISTED DELIVERY
FORCES OPERATING IN THE SECOND STAGE OF LABOUR
Powers
The forces in the second stage for delivery are:
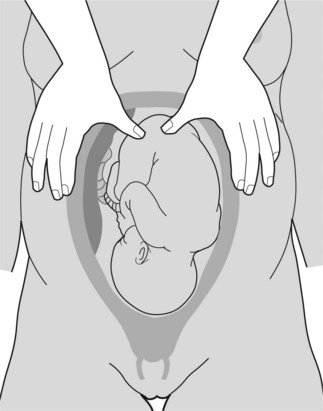
Fundal pressure
Fundal pressure is used during caesarean births and assisted deliveries (see Figure 16.1). Pressure is applied at the uterine fundus (usually over the buttocks of the fetus) along its longitudinal axis to coincide with uterine contractions and maternal expulsive efforts. Fundal pressure should not be applied in between contractions particularly when maternal effort is absent.
ASSISTED DELIVERY
Instruments for assisted delivery
Forceps
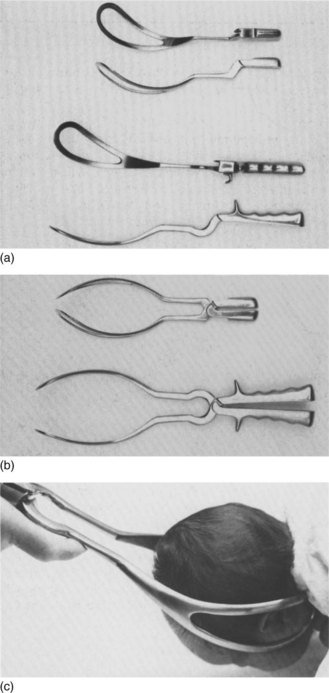
Description of forceps
Each forceps has a left and right fenestrated blade. Each traction blade has a cephalic curve for the fetal head and a pelvic curve to accommodate the curvature of the maternal pelvis. When joined as a pair through a fixed lock, these blades form a protective cage which surrounds the fetal head without compression. When traction is applied, pressure transmitted to the fetus is safely contained by the firm fetal malar bones (Figures 16.2, 16.3).
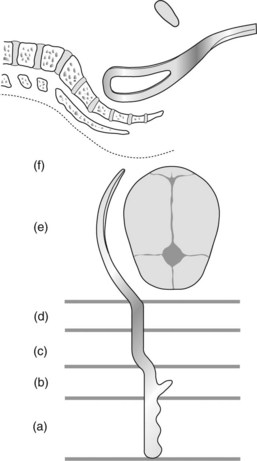
Kjelland’s rotational forceps differs from traction forceps. The shank is long and the blade is thin. The modest pelvic curve allows rotation through a much smaller circumference. The sliding lock allows application when asynclitism is present (see Chapter 19). Knobs on the handles point towards the occiput (also known as occipital knobs) (Figures 16.4–16.6).
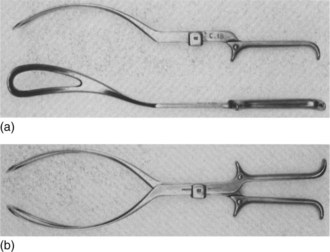
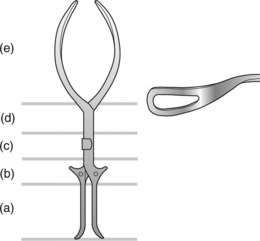
Figure 16.5 Components of Kjelland’s forceps: (a) handle, (b) shoulder, (c) sliding lock, (d) shank and (e) blade.

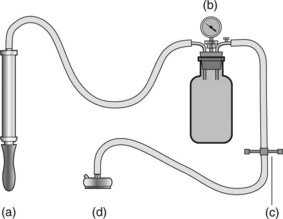
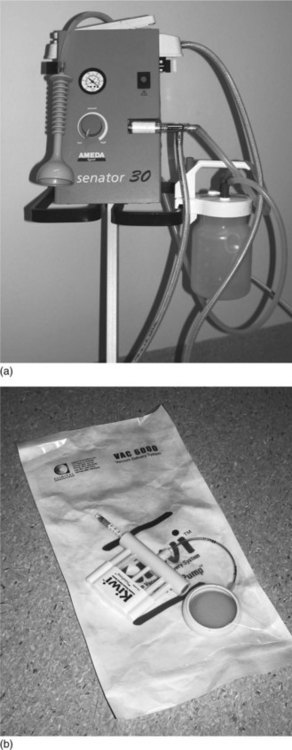
Vacuum extractors
Choosing between forceps and vacuum extraction for assisted deliveries
Neither instrument is superior for assisted vaginal deliveries. The forces and requirements for either form of assisted delivery are similar. The choice of instrument depends on the clinical scenario as well as the operator’s experience, training and preferences. Both instruments are equally suited to most assisted deliveries. In circumstances where cephalopelvic disproportion is confidently excluded and speed is of essence (e.g. ominous cardiotocographic tracing), forceps may be the instrument of choice for expediting delivery. The vacuum extractor may be preferred where asynclitism is present, when rotational delivery is needed and there is limited experience with forceps. There is no increased morbidity in completing a delivery by forceps when the vacuum fails provided that the requirements for assisted delivery are fulfilled. Table 16.1 shows a comparison between the two types of instrumental delivery. The long-term outcome is the same for mother and child.
Table 16.1 Instrumental vaginal delivery
| Forceps | Vacuum | |
|---|---|---|
| Popularity | Decreased | Increased |
| Preterm | Yes | Not before 36 weeks |
| Undilated cervix (around 9 cm) | Contraindicated | Yes |
| Anaesthesia | Yes | Need less |
| Failure to achieve delivery | Less likely | More likely |
| Tissue trauma | Possible | Less |
| Cephalhaematoma | Possible | More likely |
| Retinal haemorrhage | Possible | More likely |
| Postpartum perineal pain | Yes | Less |
TRACTION PROCEDURES
Box 16.1 describes the types of traction procedure used in assisted delivery.
Box 16.1 Traction procedures used in assisted delivery
American College of Obstetricians and Gynecologists (ACOG) classification of forceps deliveries 2000
Outlet procedure refers to the application of the instrument when:
Low procedure refers to the application of the instrument when:
Mid-pelvic procedure refers to the application of the instrument when:
Before application of instruments
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


