Care of the pregnant woman in the antenatal setting is multifaceted, requiring knowledge of the normal and abnormal pregnancy, risk factors affecting pregnancy outcome, screening tests, common pregnancy discomforts and treatments, and psychosocial tasks and issues surrounding the childbearing continuum and appropriate nursing interventions. The purpose of this chapter is to present an overview of essential aspects of preconception and prenatal care for perinatal nurses caring for women during the childbearing process. Complications which may result in a high-risk pregnancy and require additional medical and nursing intervention are discussed in detail in Chapters 5,6,7,8,9,10,11 and 12.
PRECONCEPTION CARE
Prenatal care begins with preconception healthcare. The purpose of preconception care is to deliver risk screening, health promotion, and effective interventions as a part of routine healthcare (Centers for Disease Control and Prevention [CDC], 2006a). Preconception healthcare is critical because the behaviors and exposures that occur before prenatal care is initiated may affect fetal development and subsequent maternal and perinatal outcomes. The CDC (2006a) developed 10 recommendations for improving preconception and interconception care as part of a strategic plan to improve the health of women, their children, and their families (Display 4-1). These recommendations, based on existing knowledge and evidence-based practice, were developed for improving preconception health through changes in consumer knowledge, clinical practice, public health programs, healthcare financing, and data and research activities. Each recommendation has specific action steps toward the continuing goal of achieving the Healthy People 2020 objectives to improve maternal and child health outcomes. The recommendations are aimed at achieving four goals, based on personal health outcomes:
Goal 1. Improve the knowledge and attitudes and behaviors of men and women related to preconception health.
Goal 2. Ensure that all women of childbearing age in the United States receive preconception care services (i.e., evidence-based risk screening, health promotion, and interventions) that will enable them to enter pregnancy in optimal health.
Goal 3. Reduce risks indicated by a previous adverse pregnancy outcome through interventions during the interconception period.
Goal 4. Reduce the disparities in adverse pregnancy outcomes.
Preconception care should be tailored to meet the needs of the individual woman. Because preconception care needs to be provided across the life span and not during only one visit, certain recommendations will be more relevant to women at different life stages and with varying levels of risk. Intuitively, it makes sense to deliver preconception care in the context of primary care. All women attempting a pregnancy should follow the same behavioral recommendations, such as avoiding smoking and alcohol use and using only medications known to be safe in pregnancy. All women of childbearing age should take a daily folic acid supplement. Beginning pregnancy with nondepleted iron stores is beneficial for the maternal iron status during pregnancy and infant birth weight (Ribot et al., 2012). The importance of preconception advice to ensure that women have adequate iron stores prior to, or early in, pregnancy when supplemented with moderate daily iron doses should not be underestimated. Health promotion, risk screening, and interventions are different for a young woman who has never experienced pregnancy than for a woman aged 35 years who has had three children. Women who present with chronic diseases, previous pregnancy complications, or behavioral risk factors might need more intensive interventions. Social determinants of women’s health also play a role in birth outcome. Low socioeconomic status is a long-known risk factor for preterm birth. Identified modifiable risk factors include isotretinoin (Accutane) use, alcohol misuse, antiepileptic drug use, diabetes (preconception), folic acid deficiency, hepatitis B, HIV/AIDS, hypothyroidism, maternal phenylketonuria, rubella seronegativity, obesity, oral anticoagulant use, sexually transmitted disease (STD), and smoking (CDC, 2006a). The American College of Obstetricians and Gynecologists (ACOG, 2005a) identified the following as core preconception care factors:
Undiagnosed, untreated, or poorly controlled medical conditions
Immunization history
Medication and radiation exposure in early pregnancy
Nutritional issues
Family history and genetic risk
Tobacco and substance abuse and other high-risk behaviors
Occupational and environmental exposures
Social issues
Mental health issues
DISPLAY 4-1 Recommendations to Improve Preconception Health
Recommendation 1. Individual Responsibility across the Life
Span. Each woman, man, and couple should be encouraged to have a reproductive life plan.
Recommendation 2. Consumer Awareness. Increase public awareness of the importance of preconception health behaviors and preconception care services by using information and tools appropriate across various ages; literacy, including health literacy; and cultural/linguistic contexts.
Recommendation 3. Preventive Visits. As a part of primary care visits, provide risk assessment and educational and health promotion counseling to all women of childbearing age to reduce reproductive risks and improve pregnancy outcomes.
Recommendation 4. Interventions for Identified Risks. Increase the proportion of women who receive interventions as follow-up to preconception risk screening, focusing on high-priority interventions (i.e., those with evidence of effectiveness and greatest potential impact).
Recommendation 5. Interconception Care. Use the interconception period to provide additional intensive interventions to women who have had a previous pregnancy that ended in an adverse outcome (e.g., infant death, fetal loss, birth defects, low birth weight, or preterm birth).
Recommendation 6. Prepregnancy Checkup. Offer, as a component of maternity care, one prepregnancy visit for couples and persons planning pregnancy.
Recommendation 7. Health Insurance Coverage for Women with
Low Incomes. Increase public and private health insurance coverage for women with low incomes to improve access to preventive women’s health and preconception and interconception care.
Recommendation 8. Public Health Programs and Strategies. Integrate components of preconception health into existing local public health and related programs, including emphasis on interconception interventions for women with previous adverse outcomes.
Recommendation 9. Research. Increase the evidence base and promote the use of the evidence to improve preconception health.
Recommendation 10. Monitoring Improvements. Maximize public health surveillance and related research mechanisms to monitor preconception health.
Centers for Disease Control and Prevention. (2006a). Recommendations to improve preconception health and health care—United States: A report of the CDC/ATSDR preconception care work group and the select panel on preconception care. Morbidity and Mortality Weekly Report Recommendations and Reports, 55(RR 06), 1-23.
Implementation of the CDC recommendations is targeted toward (1) women and men of childbearing age having high reproductive awareness (i.e., they understand risk factors related to childbearing), (2) women and men having a reproductive life plan, (3) pregnancies being intended and planned, (4) women and men of childbearing age having healthcare coverage, (5) women of childbearing age being screened before pregnancy for risks that could affect the pregnancy, and (6) women with previous adverse pregnancy outcomes (e.g., infant death, very low birth weight, or preterm birth) having access to interconception care aimed at reducing their risks. The reader is referred to http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5506a1.htm for complete recommendations.
PRENATAL CARE
The American Academy of Pediatrics (AAP) and ACOG (2007a) describe prenatal care thusly: “A comprehensive antepartum care program involves a coordinated approach to medical care and psychosocial support that optimally begins before conception and extends throughout the antepartum period.” This comprehensive program includes (1) preconceptional care, (2) prompt diagnosis of pregnancy, (3) initial prenatal evaluation, and (4) follow-up prenatal visits. Quality prenatal care includes education and support for the pregnant woman, ongoing maternal-fetal assessment, preparation for parenting, and promotion of a positive physical and emotional family experience. Comprehensive services include health education; nutrition education; the Women, Infants, and Children’s (WIC) program; social services assessment; assessment for intimate partner violence, depression screening; medical risk assessment; and referral as appropriate. To provide optimal, individualized care, nurses must recognize the effect of pregnancy on a woman’s life span. Although a woman’s preconceptional health has an impact on pregnancy, it is also true that childbearing is an event that may affect her long-term health. It is important to consider pregnancy within the larger context of women’s health and primary care.
Continued contact with the pregnant woman through comprehensive prenatal care provides an ideal opportunity for the healthcare provider to assess for and identify potential problems that may place the woman and fetus at risk. The question of the necessary number of visits has been explored by researchers for several decades. The U.S. Department of Health and Human Services (USDHHS) Expert Panel on the Content of Prenatal Care (1989) recommended that healthy, pregnant women who are at low risk for pregnancy complications could attend fewer visits without negative consequences. For nulliparous women, nine visits were recommended; for multiparous women, seven visits were recommended. However, these recommendations have been slow to be adopted. Dowswell and colleagues (2010) reported that in settings with limited resources, reduced visit programs are associated with higher perinatal mortality when compared to standard prenatal care. Women in all settings were less satisfied with the reduced visits schedule and perceived the gap between visits as too long. Although reduced visits may be associated with lower costs, visits should not be reduced without close monitoring on fetal and neonatal outcomes. See Display 4-2 for guidelines for routine prenatal care visits.
Another model of prenatal care, Centering Pregnancy, was developed in 1998 and integrates group support with prenatal care. Centering Pregnancy uses the essential components of prenatal care: risk assessment, health promotion, medical and psychosocial interventions, and follow-up. Group prenatal care intuitively seems to be an efficient method of simultaneously communicating the same message to multiple patients as well as promoting the development of an instant support group for women and families. This model involves 10 90- to 120-minute sessions that begin at 16 weeks’ gestation and conclude with a postpartum meeting (Rising, 1998; Rising, Kennedy, & Klima, 2004). The initial prenatal visit is an individual appointment. Each woman is invited to join a group of 8 to 12 other women with similar estimated dates of birth. Sessions allow for individual time with the care provider and group sharing and education. Groups are led by advanced practice nurses or other healthcare professionals with expertise in group process. Group prenatal care results in equal or improved perinatal outcomes without added cost (Ickovics et al., 2007; Kennedy et al., 2011). See https://www.center-inghealthcare.org/index.php for more information. Nurses must be aware of these prenatal care models in order to offer the highest quality evidence-based care to pregnant women.
Regardless of the approach to delivery of prenatal care, evidence-based recommendations for prenatal care have been established (National Guideline Clearinghouse [NGC] and the Institute for Clinical Systems Improvement [ICSI] are readily located at http://guidelines.gov). Display 4-2 is a summary of the content, timing, counseling and education that should be delivered in prenatal care.
Because early initiation of prenatal care is important to the health of the mother and to the optimization of pregnancy outcomes, a goal of increasing the proportion of pregnant women who initiate prenatal care in the first trimester to 90% was established as one of the Healthy People 2000 objectives and retained as a Healthy People 2010 objective ( Objective 16-6a). Between 1980 and 1991, three of every four (76%) pregnant women in the United States who had a live birth began prenatal care in the first trimester (Lewis, Matthews, & Heuser, 1996). Although this proportion increased to 84% in 2002, it remains below the Healthy People 2010 goal of 90% (USDHHS, 2000). In the most recent objectives, Healthy People 2020, the target is 77.9%, a 10% improvement from the baseline of 70.8% of women delivering a live birth who received prenatal care in the first trimester in 2007 (USDHHS, 2010). Therefore, little progress has been made on early initiation of prenatal care.
Promotion of early pregnancy recognition could be a means of improving birth outcomes as early pregnancy recognition is associated with improved timing and number of prenatal care visits (Ayoola, Nettleman, Stommel, & Canady, 2010). Nurses can encourage and empower women to access prenatal care at a critical point in fetal development.
PRENATAL RISK ASSESSMENT
The goal of risk assessment is to identify women and fetuses at risk for developing antepartum, intrapartum, postpartum, or neonatal complications to promote risk-appropriate care that will enhance the perinatal outcome. The underlying causes of preterm labor and intrauterine growth restriction (IUGR) are not fully understood. However, a large body of knowledge regarding risk factors associated with prematurity and low birth weight has developed. These factors include demographic, medical, obstetric, sociocultural, lifestyle, and environmental risks. It is important to note that many risk factors have been identified in studies of women who develop complications of pregnancy or deliver preterm; however, no firm cause-and-effect relationship between some of the commonly associated risk factors and poor outcome has been established. Riskassessment tools may be helpful in distinguishing between women at high and low risk (Display 4-3). Unfortunately, the predictive value of these tools is limited. Enthusiasm for risk assessment must be tempered with reality. Identification of real or potential problems should be a shared process in which the nurse assesses the woman’s individual perception of risk. Risk presented as a calculation of odds may not resonate with the pregnant woman; most women use a set of values that is rooted in their lives, personal philosophies, and family and health histories to make sense of risk (Carolan, 2009). Approximately one third of the potential complications of pregnancy occur during the intrapartum period and are not predictable by current risk-assessment systems (AAP & ACOG, 2007). However, risk assessment directs the provider toward areas in which intervention can have a positive impact on perinatal outcomes. The nurse’s knowledge of prenatal risk assessment allows for anticipatory planning, individualized education, and appropriate referral. Outcomes of risk assessment provide guidelines by which the effectiveness of the care can be evaluated. The nurse’s role in prenatal care is discussed within these parameters.
DISPLAY 4-2 Guidelines for Prenatal Care National Guideline Clearinghouse (NGC) and the Institute for Clinical Systems Improvement (ICSI) 2010
aIt is acceptable for the history and physical and laboratory tests listed under Visit 1 to be deferred to Visit 2 with the agreement of both the patient and the provider.
bShould also include all subjects listed for the preconception visit if none occurred.
cAdministration of the varicella vaccine during pregnancy is contraindicated.
Ab, antibody; ABO, blood group system; Ag, antigen; BMI, body mass index; CBC, complete blood count; CPR, cardiopulmonary resuscitation; GC, gonococci; GDM, gestational diabetes mellitus; HDL, high density lipoprotein; MMR, measles/mumps/rubella; OB, obstetrics; RhoGAM, Rho(D) immune globulin; VBAC, vaginal birth after cesarean; VZIG, varicella zoster immune globulin. Institute for Clinical Systems Improvement. (2010) . Routine Prenatal Care. Bloomington, MN: Author. Retrieved from http://guidelines.gov/content.aspx?id=24138&search=prenatal+care
DISPLAY 4-3 Risk Assessment
OBSTETRIC HISTORY
History of infertility
Grand multiparity
Previous stillborn/neonatal death
Incompetent cervix
Previous multiple gestation
Uterine or cervical anomaly
Previous prolonged labor
Previous preterm labor or preterm birth
Previous low-birth-weight infant
Previous cesarean birth
Previous midforceps delivery
Previous macrosomic infant
Previous pregnancy loss (spontaneous or induced)
Last delivery <1 year before present conception
Previous hydatidiform mole or choriocarcinoma
Previous infant with neurologic deficit, birth injury, or congenital anomaly
Previous surgeries, particularly involving the reproductive organs
Pulmonary disease
Chronic hypertension
Endocrine disorders
Hemoglobinopathies
Sexually transmitted diseases
Surgery during pregnancy
CURRENT OBSTETRIC STATUS
Inadequate prenatal care
Intrauterine growth-restricted fetus
Polyhydramnios
Maternal anemia
Weight gain <10 lb
Weight loss >5 lb
Sexually transmitted diseases
Pregnancy-induced hypertension, preeclampsia
Premature rupture of membranes
Rh sensitizations
Preterm labor
Overweight or underweight
Immunization status
Large-for-gestational-age fetus
Placenta previa
Abnormal presentation
Fetal or placental malformations
Abnormal fetal surveillance tests
Abruptio placentae
Multiple gestation
Postdatism
Fibroids
Fetal manipulation
Cervical cerclage
Maternal infection
PSYCHOSOCIAL FACTORS
Inadequate finances
Poor housing
Social problems
Unwed, father of baby uninvolved or unsupportive
Adolescent
Minority status
Poor nutrition
Parental occupation
More than two children at home, no help
Inadequate support systems
Unacceptance of pregnancy
Dysfunctional grieving
Psychiatric history
Attempt or ideation of suicide
Intimate partner violence
Demographic Factors
Maternal age <16 or >35 years
Education <11 years
Lifestyle
Smokes >10 cigarettes/day
Alcohol intake
Substance abuse
Heavy lifting, long periods of standing
Long commute
Unusual stress
INITIAL PRENATAL VISIT
Antepartum assessment begins with the first prenatal visit. Generally, a woman with an uncomplicated pregnancy is examined approximately every 4 weeks for the first 28 weeks of pregnancy, every 2 to 3 weeks until 36 weeks’ gestation, and weekly thereafter. Women with medical or obstetric problems may require closer surveillance. Intervals between visits are determined by the nature and severity of the problem (AAP & ACOG, 2007).
The initial prenatal visit is of vital importance and requires careful attention to detail. The nurse is obligated to practice within the framework of professional standards, such as the Association of Women’s Health, Obstetric and Neonatal Nurses’ (AWHONN) Standards and Guidelines (2009) and Guidelines for Perinatal Care (AAP & ACOG, 2007), which provide guidelines for practice in the ambulatory care setting. During the first prenatal visit, baseline health data are obtained and assessed, a patient-centered relationship is established, and the plan of care is initiated. Risk assessment during the initial prenatal visit should include the following:
A careful family medical history, individual medical history, reproductive health history, psychosocial history, and genetic history
A comprehensive physical examination designed to evaluate potential risk factors
Fetal assessment, as developmentally appropriate (e.g., fetal heart rate [FHR], fetal activity, kick counts) and individualized fetal surveillance, as indicated (e.g., ultrasonography, biophysical profile [BPP])
Maternal Age
The association between Down syndrome and advanced maternal age has been long documented (Hook, 1981). Maternal age of 35 years and older is associated with an increased risk of fetal death (Huang, Sauve, Birkett, Fergusson, & van Walraven, 2008; Silver, 2007) and obstetrical complications, perinatal morbidity, and mortality. Children born to mothers younger than 19 or older than 35 years of age have an increased risk of prematurity, congenital anomalies, and risks from other complications of pregnancy (March of Dimes, 2011a). However, researchers report that pregnancy outcomes previously linked to maternal age are mitigated by poverty (Cunningham et al., 2010; Markovitz, Cook, Flick, & Leet, 2005). With poor socioeconomic status, the risk of perinatal morbidity increases after the age of 35, but with adequate income and healthcare, women in that age group experienced only a slight increase in gestational diabetes (GDM), pregnancy-induced hypertension, placenta previa or placental abruption, and cesarean birth (Markovitz et al., 2005).
Complications common in pregnant adolescents include low birth weight, preeclampsia and pregnancyinduced hypertension, IUGR, and preterm labor. In younger mothers, socioeconomic factors largely explain increased neonatal mortality risk (Markovitz et al., 2005). Although much of the literature links advanced maternal age to adverse perinatal outcomes, there is a paucity of data linking advanced maternal age with outcomes of preterm newborns. Recently, Kanungo and colleagues (2011) reported that among preterm newborns, the odds of survival without major morbidity improved by 5% and mortality (8%), necrotizing enterocolitis (11%), and sepsis (9%) reduced as maternal age group increased by 5 years. Knowledge of these risks and outcomes serves as a guide for counseling women for whom age is a risk factor.
Medical and Obstetric History
Assessment of health factors that may influence pregnancy outcome includes careful evaluation of the woman’s individual medical, gynecologic, obstetric, psychosocial, and environmental history. Pertinent family history of the woman and her partner is necessary for complete evaluation. Maternal-family reproductive health history (e.g., preeclampsia, hypertension, diabetes, preterm birth) may be particularly significant. The additional physiologic stress of pregnancy affects chronic conditions (e.g., diabetes, hypertension, cardiac disease). Likewise, factors such as a recent history of STDs or chemical dependency may be indicative of lifestyle behaviors that threaten maternal-fetal well-being.
Obstetric history, such as length of previous labors, cesarean birth, birth weight, gestational age, history of preterm labor or preterm birth, grand multiparity, elective or spontaneous abortion, instrument-assisted birth, previous stillbirth, or uterine or cervical anomaly may indicate potential risks for the current pregnancy. Apply these risk factors within the context of the gestational age. For example, a history of preterm birth would be a pertinent risk to a woman who is presently at 20 weeks’ gestation but is not relevant when the woman is at 37 weeks’ gestation. Note familial history, including cardiac disease, diabetes, and bleeding disorders. The woman may also be affected by her mother’s obstetric history. There is a familial predisposition to develop preeclampsia. The medical and genetic history of the birth parents serves to guide counseling and testing for predisposed genetic complications. The family history is the most important source of genetic information. The ideal time for genetic screening is before attempting pregnancy. Although general population screening is not considered appropriate, Williams and Lea (2003) recommend that persons with the following conditions be offered genetic screening:
Developmental disability of unknown etiology, including women with developmental disabilities who present for preconception or prenatal care
Autism
Unexplained mental retardation or developmental delay, particularly if the member of the family is related to the patient through females
Family history of fragile X syndrome
Family history that suggests increased risk for specific autosomal recessive disease
Probably the most common indications for genetic counseling and prenatal diagnosis are maternal age and abnormal maternal serum screening. If the initial prenatal risk assessment reveals factors that carry risk for the baby (e.g., Tay-Sachs, sickle cell disease/trait, thalassemia, cystic fibrosis), the woman (and her partner) should be offered genetic counseling and additional testing if the woman so desires.
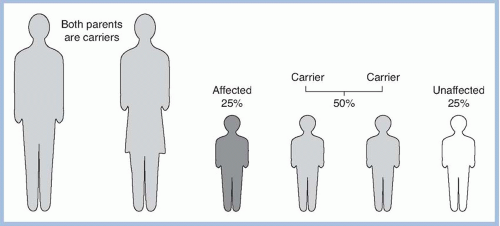
Genetic counseling has grown into a well-recognized specialty. Our understanding of genetics and genomics in healthcare has changed in recent years, however. Genetic conditions inherited in families are caused by gene mutations present on one or both chromosomes of a pair. The three main patterns of Mendelian inheritance are autosomal dominant, autosomal recessive, and X-linked (Fig. 4-1). The term “genomics” refers to the study of all the genes in the human genome together, including their interactions with each other and the environment (Feetham, Thomson, & Hinshaw, 2005). Genes can cause diseases, and they also may affect disease susceptibility and resistance, prognosis and progression, and responses to illnesses and their treatments. This range of responsiveness results in variable testing sensitivity, specificity, and predictive value of the genetic test (Feetham et al., 2005).
FIGURE 4-1. The inheritance pattern of offspring when both parents are carriers of an autosomal recessive gene.
As knowledge of the behavioral, environmental, and genetic mechanisms of disease increases, individuals and families will need to reframe their concepts and experiences with diagnosis, treatment, and prevention (Feetham et al., 2005). Therefore, individualized education, planning, and support are vital to the process of genetic counseling. Genetic counseling and fetal surveillance techniques force a woman (and her partner) to consider the amount and kind of information desired, subsequent decisions related to that information, and what those decisions may reflect about their self-image and personal values. Nurses are knowledgeable, nonthreatening confidants as the woman and her partner sort through the information and decision making. Nurses, therefore, need to be cognizant of the benefits, limitations, and social implications of the counseling and testing process.
Lifestyle Factors
Lifestyle or behavioral factors significantly affect women’s health in general and perinatal health specifically. Living conditions, marital status, occupation, nutrition, and use of tobacco, alcohol, and illicit substances can all affect pregnancy outcome. Socioeconomic factors may influence gestational age at entry to prenatal care, nutritional status, and availability of support systems. Number of years of completed maternal education has been correlated with birth weight, perinatal mortality and morbidity, and neonatal neurologic sequelae. In general, as years of maternal education increase, incidence of perinatal mortality and morbidity decreases. Not surprisingly, adolescents are more likely to begin prenatal care later than adults (March of Dimes, 2011b). Pregnant women who have more education are more likely to start prenatal care early and have more visits. Between 1989 and 1997 (the last data analysis that was performed), the percentage of women with delayed prenatal care or no prenatal care decreased from 25% to 18%, with improvement in both delayed prenatal care (from 22% to 16%) and in no prenatal care (from 2% to 1%). Groups more likely to have delayed or no prenatal care between 1989 and 1997 included non-Hispanic blacks, Hispanics, women aged <20 years, women with <12 years of education, and multiparous women (CDC, 2000). This association may be a reflection of education as an indicator of socioeconomic status. Women in lower socioeconomic groups tend to initiate prenatal care later than their middle socioeconomic group counterparts. The three most common reasons for late entry into care are (1) no knowledge that she was pregnant, (2) financial barriers, and (3) inability to get an appointment (CDC, 2000).
The marital status of the mother and the presence of the father as related to perinatal outcome are complex social phenomena. Marital status may be a marker for the presence or absence of social, emotional, and financial resources. Infants of mothers who are not married have been shown to be at higher risk for poor outcomes. In 2006, infants of unmarried mothers had an infant mortality rate of 9.19 per 1,000, 80% higher than the rate for infants of married mothers (Mathews & MacDorman, 2010).
Findings of older studies demonstrated an increase in perinatal morbidity and mortality associated with single motherhood (Bennett, Braveman, Egerter, & Kiely, 1994; Cooperstock, Bakewell, Herman, & Schramm, 1998; Hein, Burmeister, & Papke, 1990; Luo, Wilkins, & Kramer, 2004; Mathews, MacDorman, & Menacker, 2002). That unmarried mothers often are younger, are less well educated, and have a lower socioeconomic status than married mothers was controlled for in the older studies. More recently, births to women who live in an intimate relationship with a partner but without legal marriage have become increasingly common and widely accepted in many Western societies. However, pregnancy outcomes are worse among mothers in common-law unions versus traditional marriage relationships. One study found an overall 20% increase of adverse outcomes in unmarried, cohabiting mothers, and that free maternity care did not overcome the difference (Raatikainen, Heiskanen, & Heinonen, 2005. The highest incidence of perinatal morbidity and loss occurs in families where the father is not present (Luo et al., 2004).
When employment status of the Finnish parents in 24,939 pregnancies was examined, unemployment was associated with adolescent maternal age, unmarried status, overweight, anemia, smoking, alcohol consumption, and prior pregnancy terminations. Although antenatal care is free in Finland, this was unable to fully overcome the adverse pregnancy outcomes associated with unemployment, and small-forgestational-age risk is highest when both parents are unemployed (Raatikainen, Heiskanen, Verkasalo, & Heinonen, 2006).
Teratogen Exposure
The cause of congenital malformations can be divided into three categories: unknown, genetic, and environmental. The cause of a majority of human malformations is unknown. Both maternal and paternal environmental exposures can produce human developmental disease including preterm birth, growth restriction, functional or structural abnormalities, or death.
More than 50 teratogenic environmental drugs, chemicals, and physical agents have been described using modern epidemiologic tools and clinical dysmorphology. Severe congenital malformations occur in 3% of births. According to the CDC (Martin et al., 2006), severe congenital malformations include birth defects that cause death, hospitalization, or mental retardation; necessitate significant or repeated surgical procedures; are disfiguring; or interfere with physical performance. Each year in the United States, 120,000 newborns are born with severe birth defects (CDC, 2008). Our understanding of this process is evolving:
Whereas single genes and individual chemical exposures are responsible for some instances of adverse pregnancy outcome or developmental disease, gene-environment interactions are responsible for the majority. These gene-environment interactions may occur in the father, mother, placenta or fetus, suggesting that critical attention be given to maternal and paternal exposures and gene expression as they relate to the mode of action of the putative developmental toxicant both prior to and during pregnancy (Mattison, 2010, p. 208).
Counseling regarding possible teratogenic influences should be performed in a factual yet sympathetic and supportive way so the woman is not unduly alarmed or burdened with guilt (ACOG, 1997). Nurses should also be cognizant of the common potential teratogens in the population for which they provide care. For example, if the majority of the women come from an urban setting in which it is known that lead exposure is problematic, the history should include special attention to the risk. Maternal blood lead levels of approximately 10 mcg/dL have been linked to increased risks of pregnancy hypertension, spontaneous abortion, and reduced neurobehavioral development in the child (Bellinger, 2005).
Teratogen exposure may be associated with an occupation (e.g., X-rays, chemicals, viruses) or a lifestyle. The most common substances used by pregnant women include tobacco, alcohol, and marijuana. Alcohol is a potent teratogen in humans, and prenatal alcohol exposure is a leading preventable cause of birth defects and developmental disabilities. The harm from substance use and abuse is well known and may have disastrous effects in pregnancy, affecting all body systems and causing cardiac, pulmonary, gastrointestinal, and psychiatric complications. “Although the prevalence of substance abuse is significantly lower in pregnant women compared to nonpregnant women, some groups remain vulnerable to continued use, including those who did not intend to get pregnant and those who are less educated, unemployed, unmarried, and exposed to violence” (Massey et al., 2011, p. 143). The effects of tobacco use in pregnancy are well documented. No amount of alcohol is safe in pregnancy. Marijuana is the most commonly used illicit substance taken during pregnancy. The impact on the child is not clear. While prenatal marijuana use does not increase the risk of preterm birth, birth defects, or mortality in the first 2 years of life in exposed infants, emerging evidence indicates effects on later functioning. These effects include cognitive deficits, especially in visuospatial function, impulsivity, inattention and hyperactivity, depressive symptoms and substance use disorders, and cancer (Gray, Day, Leech, & Richardson, 2005; Huizink & Mulder, 2006). Methamphetamine abuse is becoming more common among women of reproductive age. “Meth,” also known as speed or chalk, or as ice, crystal, and glass when smoked, is a powerfully addictive stimulant and a known neurotoxic agent that damages the endings of brain cells containing dopamine. Definitive information on the impact of exposure to methamphetamine in utero is lacking. There is fair to good evidence that amphetamines do not cause congenital anomalies. Studies consistently show amphetamine exposure during pregnancy is associated with an increased risk of preterm birth, low birth weight, and birth of small-for-gestational-age infants, but most of these studies have not adjusted for confounding factors, such as tobacco use, polydrug exposure, nutrition, and access to prenatal care (UpToDate, 2012). Screening for alcohol and substance use and abuse is discussed in more detail later in this chapter.
Assessing the use of prescription or over-the-counter medications and use of complementary and alternative therapies such as herbs, homeopathy, and folk remedies is crucial. This provides nurses with a more complete picture of the woman’s approach to healthcare and allows them to identify potentially harmful practices. Commonly, pregnant women are counseled that using acetaminophen is safe whereas using a nonsteroidal anti-inflammatory drug (NSAID) such as ibuprofen is not. If there is a potential substance or practice about which there is a question of teratogenicity, nurses can contact the Organization of Teratology Information Services at its toll-free number ([866] 626-OTIS or [866] 626-6847) or visit http://www.otispregnancy.org for more information. This organization is a national service that can answers questions or refer pregnant women or nurses to local resources.
Over the last three decades, first trimester use of prescription medications increased by more than 60% and the use of four or more medications more than tripled; approximately half of childbearing-aged women use at least one medication (Mitchell et al., 2011). As more women delay childbearing and as the population has grown more obese, there are more likely to be women of childbearing age using medications for chronic diseases such as diabetes, hypertension, and hyperlipidemia. Medications to treat the later disorders include angiotensin-converting enzyme inhibitor (ACE inhibitor), angiotensin receptor blocker (ARB), or HMG-coenzyme A reductase inhibitor (statin). Use of ACE inhibitors and ARBs are associated with wellestablished risks: oligohydramnios, fetal renal dysplasia, IUGR, and fetal death (Morrical-Kline, Walton, & Guildenbacher, 2011). Statin use during pregnancy is contraindicated with case reports demonstrating vertebral, anal, cardiac, tracheal, esophageal, renal, and limb anomalies (Patel, Edgerton, & Flake, 2006). Consequently, it is important for the primary care provider as well in women’s health to be cognizant of this growing shift in the population of childbearing women with regard to medication use and to counsel women appropriately.
Nutrition
The impact of nutrition on maternal and fetal wellbeing cannot be underestimated. The special physiology of a woman creates variable nutrient requirements during different stages of the life cycle. Nutritional practices influence every pregnancy, as well as a woman’s risk for anemia, diabetes mellitus, cardiovascular disease, osteoporosis, and several types of cancer. Specific complications of pregnancy, such as preeclampsia, preterm birth, IUGR, and low-birth-weight infants with associated detrimental outcomes, can be correlated to nutritional status. A healthy, well-nourished woman has a surplus of all nutrients. The key components of a health-promoting lifestyle during pregnancy include appropriate weight gain; appropriate physical activity; consumption of a variety of foods in accordance with the Dietary Guidelines for Americans 2005; appropriate and timely vitamin and mineral supplementation; avoidance of alcohol, tobacco, and other harmful substances; and safe food handling.
Approximately 60% of American women do not gain the appropriate amount of weight during pregnancy, with more gaining too much, especially those with a high prepregnancy BMI (Olson, 2008). Current weight gain guidelines are described in Table 4-1. In 2005, the U.S. Department of Agriculture created an interactive Web-based MyPyramid, now ChooseMyPlate. The Web site provides food intake and physical activity recommendations for persons aged 2 and older, replacing healthy foods for unhealthful and offering diet tracking, menu planning, nutrition information, and personalized advice. The strategies are easy to understand for the lay public. The information should be used to complement and not substitute for prenatal education (Shieh & Carter, 2011). The nurse is encouraged to explore the Web site for use with preconception, prenatal, and lactating women: http://www.choosemyplate.gov.
The nutrition assessment includes diet intake information (3-day recall), monitoring weight gain, and hematologic assessment. Assessment of usual dietary patterns provides a basis for understanding nutritional health. Variations from the normal dietary routine, such as eating disorders, food avoidance, or special diets; food resources; and metabolic disorders such as diabetes, warrant additional interventions. Women who have eating disorders may be reticent to reveal this information. This assessment may require a number of prenatal visits and a building of a trusting relationship between the nurse and the woman. After an eating disorder is revealed, the nurse should ask the woman how she manages eating food and meals, as well as what her attitude is toward eating (e.g., preoccupation with food, feeling guilty after eating, engaging in dieting, enjoyment of food).
Table 4-1. RECOMMENDATIONS FOR WEIGHT GAIN DURING PREGNANCY
Prepregnant Status
BMI
Weight Gain (Pounds/Kilograms)
Singleton pregnancy
Underweight
<18.5
28-40 lb (12.7-18.2kg)
Normal weight
18.5-24.9
25-35 lb (11.4-15.9 kg)
Overweight
25.0-29.9
15-25 lb (7.0-11.5 kg)
Obese
>30
11-20 lb (5.0-9.0 kg)
Twin pregnancy
Underweight
<18.5
No recommendation due to insufficient data
Normal weight
18.5-24.9
37-54 lb (16.8-24.5 kg)
Overweight
25.0-29.9
31-50 lb (14.1-22.7 kg)
Obese
>30
11-20 lb (11.4-19.1 kg)
From Institute of Medicine (2009) . Weight Gain During Pregnancy: Reexamining the Guidelines. http://www.iom.edu/Reports/2009/Weight-Gain-During-Pregnancy-Reexamining-the-Guidelines.aspx
Most nutritional advice for pregnant women is based on the 1990 Institute of Medicine (IOM) Pregnancy Report, the 2005 Dietary Guidelines for Americans by the USDHHS and U.S. Department of Agriculture, and the 2006 IOM publication, Dietary Reference Intakes: The Essential Guide to Nutrient Requirements. The current dietary recommendations developed by the IOM include (1) increased intake of protein from 60 to 80 g/day (1.1 g/kg/day); (2) 340 additional calories per day in the second trimester and 452 calories per day in the third trimester; (3) increased iron intake from 15 to 30 g/day; and (4) increased folate consumption from 400 to 800 mcg/day. The recommended amount of calcium for women aged 19 to 50, pregnant or not, is 1,000 mg/day; for adolescents up to age 18, it is 1,300 mg daily. There are certain special circumstances that may affect these recommendations. For example, if there is a history of a child with a neural tube defect (NTD), the folic acid recommendation is increased to 4 mg rather than 0.4 to 0.8 mg/day. Nurses should encourage women to consume a variety of foods, eat at regular intervals (three meals a day and healthy snacks), drink milk two to three times per day, reduce caffeine, and avoid alcohol. Common discomforts (e.g., nausea and vomiting of pregnancy, heartburn, and varied reactions to taste or smell of food) can prove challenging to the woman who is trying to follow pregnancy dietary recommendations. Knowledge of safe remedies is the basis for advice when helping women with these discomforts. For example, acupressure wristbands and small, frequent feedings can be of help to some women to decrease nausea.
Another aspect of the nutritional assessment is the use of vitamins and herbs. Because herbs and vitamins are considered dietary supplements, these products are not regulated in the same manner that prescription and over-the-counter medications are. Often the products are labeled as “natural,” and the woman may conclude that the product is therefore not harmful. Excesses of one nutrient can alter the need for, absorption of, or use of other nutrients. Supernutrient regimens or megadoses of vitamins (especially those that are fat soluble) may be harmful and cannot ensure a healthy pregnancy.
Vitamin D deficiency is the most common nutritional deficiency worldwide in both children and adults. It has also been observed that vitamin D deficiency is linked to preeclampsia during pregnancy and an increased risk of having a cesarean section (Bodnar et al., 2007; Merewood, Mehta, Chen, Bauchner, & Holick, 2009). However, it is not necessary to screen vitamin D levels in the general population of pregnant women. Instead, a dietary supplement of 400 IU (10 mcg) daily is recommended and can be found in most prenatal vitamins. There is insufficient evidence to recommend more than what is contained in prenatal vitamins. Women at risk of vitamin D deficiency (low dietary intake as in vegetarians, inadequate sunlight exposure, and ethnic minorities, especially those with darker skin) can be screened and treated (1,000 to 2,000 IU/day) if low levels are found (ACOG, 2011).
Fish are an excellent source of protein, are low in saturated fats, and contain omega-3 fatty acids. Nearly all fish and shellfish contain trace amounts of mercury; therefore, pregnant and lactating women are advised to avoid fish with potentially high methylmercury levels: shark, swordfish, king mackerel, and tile fish. Pregnant women ingest no more than 12 oz or two servings of canned tuna per week and no more than 6 oz of albacore or “white” tuna (U.S. Environmental Protection Agency, 2011). If the mercury content of locally caught fish is unknown, then overall fish consumption should be limited to 6 oz per week.
Avoidance of foodborne illnesses (e.g., norovirus causing acute gastroenteritis, Salmonella, listeriosis, Escherichia coli, or hepatitis A), which cause maternal disease, congenital defects, preterm labor, miscarriage, and fetal death, is also important for the nurse to assess and to teach the woman. To reduce the risk of foodborne illness, it is important for the woman to:
Practice good personal hygiene (hand washing and care of kitchen utensils, cookware, and surfaces).
Consume meats, fish, poultry, and eggs that are fully cooked.
Avoid unpasteurized dairy and fruit/vegetable products.
Wash fresh fruits and vegetables prior to eating.
Avoid raw sprouts (alfalfa, clover, radish, and mung bean).
Avoid listeriosis by refraining from processed/deli meats, hot dogs, soft cheeses, smoked seafood, meat spreads, and pate.
The FDA provides advice on food safety for women at http://www.fda.gove/food/resourcesforyou/healtheducators/ucm081785.htm.
Many pregnant women experience pica (eating non-food substances) during pregnancy. Some women are embarrassed to tell the nurse about these cravings, yet they may significantly interfere with dietary intake of proper nutrients during pregnancy. Pica cravings are not limited to any one group, educational level, race, ethnic group, income level, or religious belief but rather are universal; however, the type of substance ingested does seem to be culturally influenced (Young, 2010). In the United States, the practice of pica during pregnancy is linked to lower income women, African American heritage, family or personal history of pica during childhood or before pregnancy, strong cravings during pregnancy, and cultural groups that endorse pica during pregnancy as important for fertility and femininity (Corbett, Ryan, & Weinrich, 2003). As a part of nutrition assessment, nurses should question (in a nonjudgmental style) patients at each prenatal visit regarding pica practice. Pica may be practiced for cultural or other reasons unknown to nurses. Working with patients to discover what they are eating and helping them to substitute foods with nutritional value can be a part of a nursing care plan that results in a positive pregnancy outcome (Corbett et al., 2003).
Occupation
Women in low-income positions or employed as unskilled laborers are at increased risk for preterm labor. A meta-analysis of working conditions and pregnancy outcome showed a significant positive association between preterm birth and physically demanding work, shift work, standing for longer than 3 hours/day or standing as the predominant occupational posture, and a high cumulative work fatigue score. Additionally, physically demanding work is positively associated with small-for-gestational-age babies, hypertension, and/or preeclampsia. Working long hours was not associated with an adverse pregnancy outcome (Mozurkewich, Luke, Avni, & Wolf, 2000). However, decreasing or eliminating work during pregnancy may place the woman at greater socioeconomic risk by threatening her livelihood. Activities that cause excessive fatigue such as heavy work, job-related stress, and psychosocial stress may stimulate uterine contractions and increase the risk of perinatal complication (Mozurkewich et al., 2000; Papiernik, 1993). Areas to ask about in the nature of the woman’s job include whether she sits or stands continuously, lifts heavy objects, perceives problems with ventilation, and is exposed to toxic chemicals or radiation. Hobbies and the home environment should be assessed also. Household tasks may be a source of fatigue equal to or greater than job-related fatigue.
Psychosocial Screening
Psychosocial screening of every woman presenting for prenatal care is an important step toward improving the woman’s health and the birth outcome. In this way, the nurse can identify areas of concern, validate major issues, and make suggestions for possible changes. Depending on the nature of the identified problem, a referral may be made to an appropriate member of the healthcare team. A woman may be reluctant to share information until a trusting relationship has been formed. Questions asked at the first prenatal visit bear repeating with ongoing prenatal care. The woman may need reassurance as to the confidentiality of the information. For example, if she reveals she uses cocaine, would she be turned over to the judicial system and possibly jailed? Nurses are obligated to know how to answer the woman when these issues arise.
Pregnancy affects the entire family, and, therefore, assessment and intervention must be considered in a family-centered perspective. Stress has been suggested as a potential contributor to preterm birth and physical complications during pregnancy and birth, including prolonged labor, increased use of intrapartum analgesics and barbiturates, and other complications. Unusual stressful events, such as the death of a significant family member or friend, job loss, or a problematic relationship with the baby’s father may increase risk of poor pregnancy outcome. Home conditions (e.g., private or government housing), quality of comfort (e.g., heat, water), housekeeping burden, and number and age of previous children influence stress levels. Nurses should be aware that many women continue to work under hazardous or stressful conditions out of economic necessity, but that they will attempt to minimize any known risk factors as much as possible. Additionally, nurses should assess how the woman appraises her situation (e.g., what one woman finds stressful, another may not). Nurses should identify resources available to the pregnant woman (e.g., support groups, social worker, counselor, etc.).
Only gold members can continue reading. Log In or Register to continue