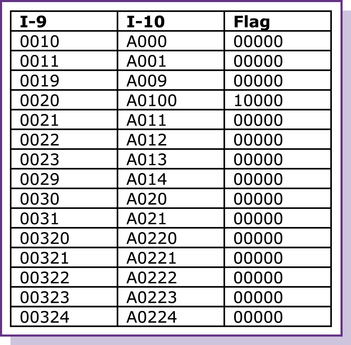
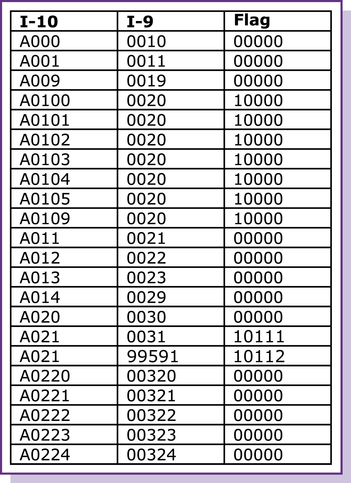
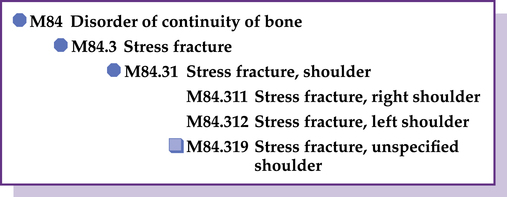
CHAPTER 1 After completing this chapter you should be able to 1. Explain the development of the ICD-10-CM. 2. Describe how the ICD-10-CM replaces the ICD-9-CM, Volumes 1 and 2. 3. Identify the improvements in the ICD-10-CM. 4. List the official instructional notations in ICD-10-CM. 5. Describe the format of ICD-10-CM. In July 2007, the International Classification of Disease, 10th revision, Clinical Modification (ICD-10-CM) was released and replaced the “pre-release draft of June 2003.” In 2009, another updated I-10 was released. In January 2010, another updated version was released. These releases of I-10 were intended for public viewing, but the codes were not valid for any purpose. According to the NCHS, the implementation date for I-10 is October 1, 2013. The material in this text is based on the 2012 version of the I-10. Guidance for the use of I-10 is available at www.cms.gov/ICD10. Notable improvements in the content and format of the I-10 include the following: 1. Addition of information relevant to ambulatory and managed care encounters 3. Extensive expansion of the injury codes, allowing for greater specificity 4. Creation of combination diagnosis/symptom codes to reduce the number of codes needed to fully describe a condition 5. The addition of a sixth character 6. The incorporation of common fourth- and fifth-character subclassifications 7. Updating and greater specificity of diabetes mellitus codes 8. Facilitation of providing greater specificity when assigning codes Chapter 1 Certain Infectious and Parasitic Diseases (A00–B99) Chapter 3 Diseases of the Blood and Blood-Forming Organs and Certain Disorders Involving the Immune Mechanism (D50–D89) Chapter 4 Endocrine, Nutritional, and Metabolic Diseases (E00–E89) Chapter 5 Mental, Behavioral and Neurodevelopmental Disorders (F01–F99) Chapter 6 Diseases of the Nervous System (G00–G99) Chapter 7 Diseases of the Eye and Adnexa (H00-H59) Chapter 8 Diseases of the Ear and Mastoid Process (H60–H95) Chapter 9 Diseases of the Circulatory System (I00–I99) Chapter 10 Diseases of the Respiratory System (J00–J99) Chapter 11 Diseases of the Digestive System (K00–K95) Chapter 12 Diseases of the Skin and Subcutaneous Tissue (L00–L99) Chapter 13 Diseases of the Musculoskeletal System and Connective Tissue (M00–M99) Chapter 14 Diseases of the Genitourinary System (N00–N99) Chapter 15 Pregnancy, Childbirth, and the Puerperium (O00–O9A) Chapter 16 Certain Conditions Originating in the Perinatal Period (P00–P96) Chapter 17 Congenital Malformations, Deformations and Chromosomal Abnormalities (Q00–Q99) Chapter 18 Symptoms, Signs, and Abnormal Clinical and Laboratory Findings, Not Elsewhere Classified (R00–R99) Chapter 19 Injury, Poisoning and Certain Other Consequences of External Causes (S00–T88) Chapter 20 External Causes of Morbidity (V01–Y99) Chapter 21 Factors Influencing Health Status and Contact with Health Services (Z00–Z99) Figure 1–1 displays GEMs mapping files for codes from I-9 to I-10. Note that the GEMs files do not contain decimal points. For example, in the GEMs file for I-9, code 001.0 is 0010 and code 001.1 is 0011. For I-10 codes, A00.0 is A000 and A00.1 is A001. In Figure 1–1, column 1 displays the I-9 codes and column 2 displays the I-10 codes. Figure 1–2 displays the mapping for codes from the I-10 code system to the I-9 code system. In Figure 1–2, column 1 displays the I-10 code and column 2 displays the equivalent I-9 code. Column 3 in both figures is the “Flag” designation, which will be reviewed next. There are three different types of flag designations: The I-10 code set has a more consistent level of detail, such as a more extensive vocabulary of clinical concepts, body part specificity, and patient encounter information. There are five times more codes in the I-10 (69,000+) than in the I-9 (14,000+), so the I-9 code is often linked to more than one I-10 code. The Approximate, Flag 1, assists in the process of conversion by identifying those times when more than one code in the I-10 is available to replace an I-9 code. For example, stress fractures in the I-9 are reported with codes in the 733.93-733.98 range, and although some of the codes are for specific bones (e.g., fibula, metatarsals, femur), a code such as 733.95 reports “other” bones. Code 733.95 is reported when there is not a specific code to report the stress fracture stated in the diagnosis. As such, 733.95 becomes an umbrella code that is assigned to a wide variety of stress fracture diagnoses. The I-10 code set expands the stress fracture codes (M84.3) to be more specific. For example, Figure 1–3 illustrates the specificity of code M84.31, Stress fracture, shoulder.
An overview of ICD-10-CM
ICD-10-CM replaces the icd-9-cm, volumes 1 and 2
Improvements in the ICD-10-CM
Structure of the system
Mapping
Flags
Approximate
Approximate, flag 1.
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


 “The implementation of ICD-10-CM will require a shift for providers in their documentation habits. More specific information will be required to accurately report conditions. I think it would be beneficial for coders to be proactive in working with their providers now to coach them in more thorough documentation.”
“The implementation of ICD-10-CM will require a shift for providers in their documentation habits. More specific information will be required to accurately report conditions. I think it would be beneficial for coders to be proactive in working with their providers now to coach them in more thorough documentation.” Exercise 1-1
Exercise 1-1