Case 9 A young man with back pain
Charlie was 38 and had a long history of back pain and left-sided sciatica. He consulted Dr Mitchell complaining of numbness in the left thigh and buttock for the last 24 hours. Dr Mitchell took a history that excluded any disturbance of sphincter function, and carried out a neurological examination which identified areas of subjective sensory loss in the left L5 dermatome and the S3 dermatome (perianally on the left). There were no other abnormalities on examination. Anal tone was normal. Dr Mitchell rang the local hospital and spoke to an on-call doctor who declined to admit the patient, stating that the clinical picture was not that of cauda equina syndrome; and advised out-patient referral.
The next day Charlie returned to the practice and saw Dr Murphy. He complained of back pain radiating to the right thigh and buttock and down the leg to the hallux. The left-sided sensory symptoms were unchanged. There was no sphincter disturbance. Dr Murphy took the view, based on the record of admission being declined the previous day, that there was still no cauda equina syndrome and that the outpatient referral should be awaited.
A few days later Charlie was admitted to hospital, having developed urinary retention. He had an emergency lumbar decompression of a large disc prolapse that was compressing the cauda equina. The patient brought a claim against both of the GPs, as well as the hospital.
Do you think his claim will succeed?
 Expert opinion
Expert opinion
Should Dr Mitchell have insisted on admission?
Back pain is extremely common in general practice, accounting for about 10% of consultations. Cauda equina syndrome (CES) is very rare. It usually results from prolapsed disc material prolapsing centrally rather than laterally (where it just compresses the nerve root at that level).
A GP might on average encounter only one case of CES in a whole career. In this case Dr Mitchell realized that the existence of perianal sensory loss raised the question of cauda equina syndrome and correctly requested a specialist opinion. However, in the absence of other symptoms of cauda equina syndrome most GPs would defer to the advice given by a hospital doctor.
However, the advice received from a nonconsultant grade specialist doctor may not be correct. The distribution of sensory symptoms, particularly if objectively confirmed as signs, is important in the suspicion of CES. The sensory dermatomes are illustrated in Case Figure 2.1.
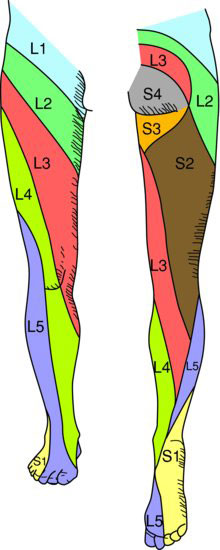
Bilateral sensory symptoms or signs at the top of the thigh or the lower buttock are suggestive that the cauda equina is involved.
According to Deyo et al. (1992) the clinical features that are most likely to predict a cauda equina syndrome are:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


