Skill 59
Pressure Ulcer Risk Assessment
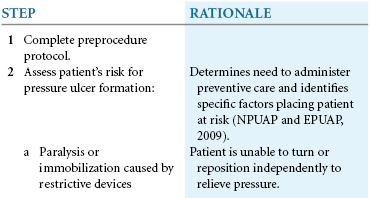
The goal in preventing the development of pressure ulcers is early identification of an at-risk patient and the implementation of prevention strategies. The overall management goals suggested by the Wound, Ostomy and Continence Nurses Society (WOCN, 2010) include the following:
2. Implement appropriate strategies/plans to:
a. Attain/maintain intact skin.
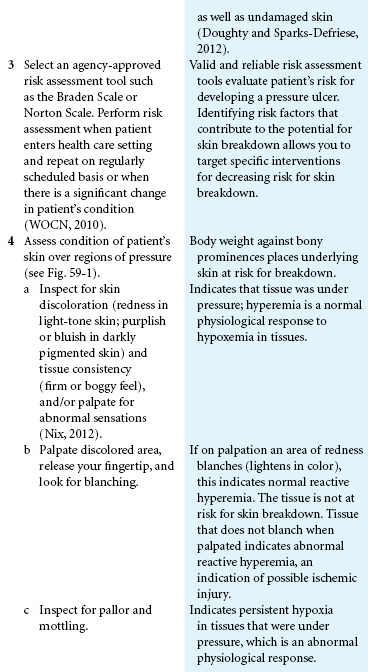
3. Implement cost-effective strategies/plans that prevent and treat pressure ulcers. The WOCN 2010 panel recommends performing a risk assessment on entry to a health care setting and repeating this on a regularly scheduled basis or when there is a significant change in an individual’s condition. Use risk assessment tools such as the Braden Scale or the Norton Scale (WOCN, 2010).
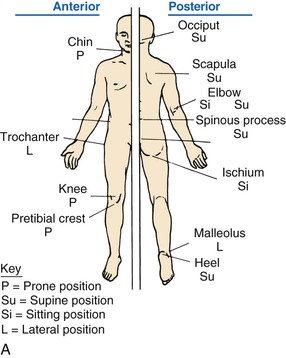
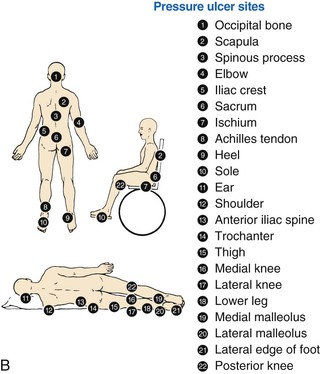
4. Inspect the patient’s skin and bony prominences at least daily. Remove devices, shoes, socks, antiembolic stockings, and heel and elbow protectors for the skin inspection. Inspect all bony prominences, including back of head, shoulders, rib cage, elbows, hips, ischium, sacrum, coccyx, knees, ankles, and heels (Fig. 59-1). Palpate any reddened or discolored areas with a gloved finger to determine if the erythema (redness of the skin caused by dilation and congestion of the capillaries) blanches (lightens in color).
Delegation Considerations
The skill of pressure ulcer risk assessment cannot be delegated to nursing assistive personnel (NAP). The nurse instructs the NAP to: