Section 5 A systems approach
5.1 The cardiovascular system





Hypertension
The control of hypertension can lead to the prevention of its cardiovascular complications. A raised systolic blood pressure is now regarded as being more significant than a raised diastolic pressure as a risk factor for CVD and isolated systolic hypertension is associated with a two to three times greater death rate from heart disease (Table 5.1).
Table 5.1 British Hypertension Society (BHS) classification of blood pressure levels
| Category | Systolic BP (mmHg) | Diastolic BP (mmHg) |
|---|---|---|
| Optimal BP | < 120 | < 80 |
| Normal BP | < 130 | < 85 |
| High normal BP | 130–139 | 85–89 |
| Grade 1 hypertension (mild) | 140–159 | 90–99 |
| Grade 2 hypertension (moderate) | 160–179 | 100–109 |
| Grade 3 hypertension (severe) | > 180 | > 110 |
| Isolated systolic hypertension (grade 1) | 140–159 | < 90 |
| Isolated systolic hypertension (grade 2) | > 160 | < 90 |
These levels will be at least 5 mmHg lower if ambulatory monitoring of blood pressure is used or home monitoring of blood pressure. The reader is referred to the full NICE guidelines on Hypertension.
There are risk factors associated with essential hypertension and these include:







 Phaeochromocytoma (tumour of the adrenal medulla).
Phaeochromocytoma (tumour of the adrenal medulla).
 Conn’s syndrome (hyperaldosteronism).
Conn’s syndrome (hyperaldosteronism).


 Acromegaly (excessive growth hormone in adulthood).
Acromegaly (excessive growth hormone in adulthood).

Diagnosis



Medication
The British Hypertension Society (BHS) and the National Institute for Health and Clinical Excellence (NICE) have together issued guidelines on the pharmacological management of hypertension (www.nice.org.uk).
Step 1





Low blood pressure
 Lead to reduced tissue perfusion throughout the body and a state of shock.
Lead to reduced tissue perfusion throughout the body and a state of shock.
 Reduce the blood supply to the heart.
Reduce the blood supply to the heart.
 Reduce renal blood flow and thus reduce urine output – leading to renal tubular necrosis.
Reduce renal blood flow and thus reduce urine output – leading to renal tubular necrosis.

Causes of hypotension



Management
 This will depend on the cause of the hypotension.
This will depend on the cause of the hypotension.
 Record observations of blood pressure, pulse and respirations as prescribed.
Record observations of blood pressure, pulse and respirations as prescribed.
 When the blood pressure is low, the pulse rate will usually be increased (tachycardia).
When the blood pressure is low, the pulse rate will usually be increased (tachycardia).


 If blood has been lost the doctor will group and crossmatch the patient and order a transfusion.
If blood has been lost the doctor will group and crossmatch the patient and order a transfusion.


 The patient may be anxious and will need reassurance.
The patient may be anxious and will need reassurance.

Coronary artery disease



Others we may be able to change with treatment. These include:







The National Service Framework (NSF) has set standards of care with the aim of reducing CAD-related deaths in the under-75-year age group by 40% by the year 2010. These guidelines are available on the Department of Health website at www.dh.gov.uk.
Angina pectoris
Types of angina




Clinical features of stable angina
 The pain is usually in the chest but may extend down the left arm or both arms or into the neck and jaw.
The pain is usually in the chest but may extend down the left arm or both arms or into the neck and jaw.
 Some patients may experience pain just in the arm, the neck, the jaw or the back.
Some patients may experience pain just in the arm, the neck, the jaw or the back.
 It is usually described as a tightness or squeezing pain, gripping or a heavy discomfort.
It is usually described as a tightness or squeezing pain, gripping or a heavy discomfort.

 The pain fades fairly rapidly on rest.
The pain fades fairly rapidly on rest.
 A glyceryl trinitrate (GTN) tablet sublingually or GTN spray buccally usually gets rid of the pain.
A glyceryl trinitrate (GTN) tablet sublingually or GTN spray buccally usually gets rid of the pain.
 The pain will always occur after a similar amount of physical exertion.
The pain will always occur after a similar amount of physical exertion.

 Sometimes the pain of angina is mild and the patient confuses it with heartburn or ignores it.
Sometimes the pain of angina is mild and the patient confuses it with heartburn or ignores it.
Management of stable angina
General advice will aim to restore normal exercise capacity and will include:





Pharmacological management
Nitrates





Beta-blockers


Calcium antagonists
These vasodilate and may be used in angina or hypertension. An example is amlodipine.




Unstable angina
 More ominous symptoms than stable angina.
More ominous symptoms than stable angina.
 The episodes of pain are more frequent.
The episodes of pain are more frequent.
 They may occur without obvious cause and at rest.
They may occur without obvious cause and at rest.
 Some patients present atypically with pleuritic pain, indigestion or dyspnoea.
Some patients present atypically with pleuritic pain, indigestion or dyspnoea.
 12-lead ECG may be normal in ACS but there may be ST depression and T-wave inversion.
12-lead ECG may be normal in ACS but there may be ST depression and T-wave inversion.
 The patient is admitted to hospital.
The patient is admitted to hospital.


 Low-molecular-weight heparins such as enoxaparin are used as anticoagulants.
Low-molecular-weight heparins such as enoxaparin are used as anticoagulants.
 Beta-blockers may be given to reduce the demand of the heart for oxygen and nutrients.
Beta-blockers may be given to reduce the demand of the heart for oxygen and nutrients.
 Statins and ACE inhibitors are also routinely given in ACS and appear to stabilize the plaque.
Statins and ACE inhibitors are also routinely given in ACS and appear to stabilize the plaque.

ST elevation myocardial infarction
Clinical features
 Chest pain which is tight or crushing in nature; 80% of patients have this.
Chest pain which is tight or crushing in nature; 80% of patients have this.
 The pain may be similar to that of angina, but more severe.
The pain may be similar to that of angina, but more severe.
 The pain lasts longer than angina – usually more than 20 minutes.
The pain lasts longer than angina – usually more than 20 minutes.
 Pain may radiate to the arms, throat and jaw.
Pain may radiate to the arms, throat and jaw.
 The pain may not respond to sublingual GTN and morphine is usually needed.
The pain may not respond to sublingual GTN and morphine is usually needed.
 Nausea and vomiting may occur.
Nausea and vomiting may occur.





Early medical management
The main aim is revascularization:
 A 12-lead ECG should be done as soon as the patient is admitted. If this baseline ECG is normal (rare) it should be repeated every 15 minutes for as long as the patient is still in pain.
A 12-lead ECG should be done as soon as the patient is admitted. If this baseline ECG is normal (rare) it should be repeated every 15 minutes for as long as the patient is still in pain.

 An intravenous cannula will be inserted to allow drugs to be given easily and immediately.
An intravenous cannula will be inserted to allow drugs to be given easily and immediately.


 The patient will be made comfortable using the headrest and pillows.
The patient will be made comfortable using the headrest and pillows.

 Observations of blood pressure and pulse will be monitored half hourly at first.
Observations of blood pressure and pulse will be monitored half hourly at first.
Cardiac markers of myocardial necrosis
 These are substances that are released into the bloodstream by the damaged myocardium and may be measured by biochemical assays.
These are substances that are released into the bloodstream by the damaged myocardium and may be measured by biochemical assays.
 Examples are cardiac troponins I and T and creatinine kinase (CK).
Examples are cardiac troponins I and T and creatinine kinase (CK).
 They rise following cardiac damage and this may confirm the diagnosis of myocardial infarction.
They rise following cardiac damage and this may confirm the diagnosis of myocardial infarction.


Cardiac arrhythmias
Cardiac arrhythmia is the commonest and most lethal complication of an MI. The most dangerous irregularity is ventricular fibrillation (VF) which constitutes a cardiac arrest. This is shown in Figure 5.1. Immediate treatment of VF using defibrillation (DC shock) may be lifesaving.
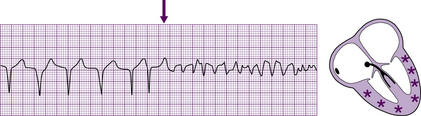
Fig. 5.1 Ventricular fibrillation.
From Hampton/The ECG Made Easy, Elsevier 2003, reproduced with permission.
Drugs used to treat cardiac arrhythmias include the following:
 Amiodarone – used in atrial fibrillation and other supraventricular arrhythmias but also ventricular arrhythmias including non-responsive ventricular tachycardia. Amiodarone should be given by a central line if possible when given intravenously.
Amiodarone – used in atrial fibrillation and other supraventricular arrhythmias but also ventricular arrhythmias including non-responsive ventricular tachycardia. Amiodarone should be given by a central line if possible when given intravenously.
 Lidocaine – used in ventricular arrhythmias, including ventricular tachycardia.
Lidocaine – used in ventricular arrhythmias, including ventricular tachycardia.
 Digoxin – used in atrial fibrillation.
Digoxin – used in atrial fibrillation.



 Atropine – used to treat bradyarrhythmias (slow rate), although a pacemaker may sometimes be needed.
Atropine – used to treat bradyarrhythmias (slow rate), although a pacemaker may sometimes be needed.
Different cardiac arrhythmias and their causes are shown in Table 5.2.
Table 5.2 Causes of different cardiac arrhythmias
| Abnormal impulse formation and ectopic beats | Conduction disturbances |
|---|---|
| At the sinus node Sinus arrhythmia Sinus bradycardia Sinus tachycardia Sinus arrest | In the sinus node SA block |
| In the atria Atrial ectopic beats Atrial tachycardia Atrial fibrillation Atrial flutter Wandering atrial pacemaker | In the AV node First- second- and third-degree AV block |
| In the AV node Nodal ectopic beats Junctional rhythm Junctional tachycardia | In the bundle of His Left bundle branch block Right bundle branch block Left anterior and posterior hemiblocks |
| In the ventricles Ventricular ectopic beats Idioventricular rhythm Ventricular tachycardia Ventricular fibrillation | Others Intra-atrial block Ventricular pre-excitation Atrioventricular dissociation |
Consequences of cardiac dysrhythmias
 Impairment of circulation or myocardial oxygenation has consequences that are extremely variable but are more pronounced in the presence of cardiac disease.
Impairment of circulation or myocardial oxygenation has consequences that are extremely variable but are more pronounced in the presence of cardiac disease.

Management of acute dysrhythmias aims:


Sinus bradycardia
 Sinus rhythm slower than 60 beats per minute during the day or 50 beats per minute in the night.
Sinus rhythm slower than 60 beats per minute during the day or 50 beats per minute in the night.
 Bradycardia occurs in about 30% of patients following MI.
Bradycardia occurs in about 30% of patients following MI.







Junctional bradycardia



Heart block
There are three forms of AV block:



Ventricular standstill and asystole
 Occurs when impulses fail to reach the ventricles or impulse formation ceases.
Occurs when impulses fail to reach the ventricles or impulse formation ceases.
 If the problem is in the conduction system, atrial P waves may continue to occur.
If the problem is in the conduction system, atrial P waves may continue to occur.
 There will be no ventricular activity unless a ventricular pacemaker takes over.
There will be no ventricular activity unless a ventricular pacemaker takes over.
 The ventricles are left without electrical stimulation and ventricular standstill occurs.
The ventricles are left without electrical stimulation and ventricular standstill occurs.
 No cardiac output and cardiac arrest results.
No cardiac output and cardiac arrest results.

This form of arrest has a poor prognosis and has several causes:




About 25% of arrests in hospital and 10% out of hospital are of this type. Mortality exceeds 90%.
Tachycardias
 An increase in rate is the normal response of the heart to increased work. This occurs so that cardiac output will increase.
An increase in rate is the normal response of the heart to increased work. This occurs so that cardiac output will increase.
 However, abnormal tachycardias are frequently associated with a diminished cardiac output.
However, abnormal tachycardias are frequently associated with a diminished cardiac output.
 Increase in heart rate is at the expense of diastole and the heart has less time to fill.
Increase in heart rate is at the expense of diastole and the heart has less time to fill.
 If ventricular filling is reduced, cardiac output will be reduced.
If ventricular filling is reduced, cardiac output will be reduced.
 Coronary blood flow takes place in diastole and therefore ischaemia may result.
Coronary blood flow takes place in diastole and therefore ischaemia may result.
 Symptoms provoked by tachycardia may include angina, dyspnoea, palpitations or syncope.
Symptoms provoked by tachycardia may include angina, dyspnoea, palpitations or syncope.
 Most tachycardias are produced by re-entry or enhanced automaticity.
Most tachycardias are produced by re-entry or enhanced automaticity.






Atrial fibrillation








Sinus tachycardia
 Sinus rhythm greater than 100 and commonly between 100 and 150.
Sinus rhythm greater than 100 and commonly between 100 and 150.
 P waves are normal and have a 1:1 relationship with the QRS.
P waves are normal and have a 1:1 relationship with the QRS.

 May be worsened by fear, pain or anxiety.
May be worsened by fear, pain or anxiety.
 Adequate analgesia will often settle this post-MI.
Adequate analgesia will often settle this post-MI.
 Mortality for those with MI is higher in sinus tachycardia than for those with sinus bradycardia.
Mortality for those with MI is higher in sinus tachycardia than for those with sinus bradycardia.




Ventricular dysrhythmias
 These include ventricular ectopics, ventricular tachycardia, ventricular flutter and ventricular fibrillation.
These include ventricular ectopics, ventricular tachycardia, ventricular flutter and ventricular fibrillation.

 Myocardial irritability following an MI is the commonest cause of ventricular arrhythmias.
Myocardial irritability following an MI is the commonest cause of ventricular arrhythmias.
 Necrotic myocardial tissue is a focus for this ectopic activity.
Necrotic myocardial tissue is a focus for this ectopic activity.
 Predisposing factors following an MI include potassium imbalances or drugs.
Predisposing factors following an MI include potassium imbalances or drugs.



Ventricular tachycardia
There are four types of ventricular tachycardia (VT):




Ventricular fibrillation
 Electrically and mechanically, the heart is completely disorganized and cardiac arrest ensues.
Electrically and mechanically, the heart is completely disorganized and cardiac arrest ensues.
 The ECG shows fine and coarse waves of irregular size, shape and rhythm.
The ECG shows fine and coarse waves of irregular size, shape and rhythm.
 Fine VF may mimic asystole and produce an apparently flat line on the ECG.
Fine VF may mimic asystole and produce an apparently flat line on the ECG.
 About 90% of deaths following acute MI are due to VF. Nearly half occur in the first half hour.
About 90% of deaths following acute MI are due to VF. Nearly half occur in the first half hour.



The Resuscitation Council (UK) has produced guidelines for the management of peri-arrest arrhythmias and these can be obtained from their website (www.resus.org.uk). They have been designed to allow the advanced life support provider to treat the patient effectively and safely in an emergency.



