Skill 43
Nasoenteral Tube
Placement and Irrigation
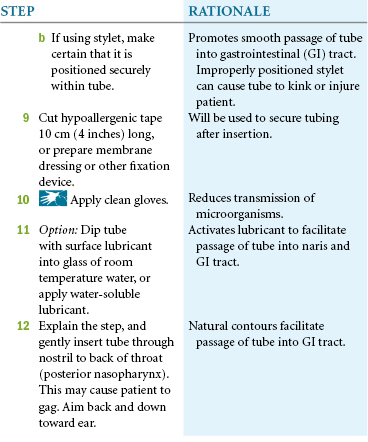
Tubes used specifically for feeding are composed of either silicone or polyurethane. They are softer and more flexible than nasogastric tubes used for drainage, and patients report that they are more comfortable. These tubes are more difficult to insert. Some tubes are weighted, and research has shown that weighted tubes are superior to nonweighted tubes. Tubes are generally coated with a hydrophilic substance that is activated when exposed to water, making it slippery and easier to insert. A nurse activates the substance immediately before insertion by simply flushing the tube inside and out with water. Wire stylets are included with some tubes, but not all. Stylets are thought to improve insertion success but have also been implicated as increasing the risk for nasopulmonary intubation. You can pass a feeding tube without the use of a stylet. Nurses often pass feeding tubes through the mouth, especially in critical care when the patient is also intubated for respiratory support.
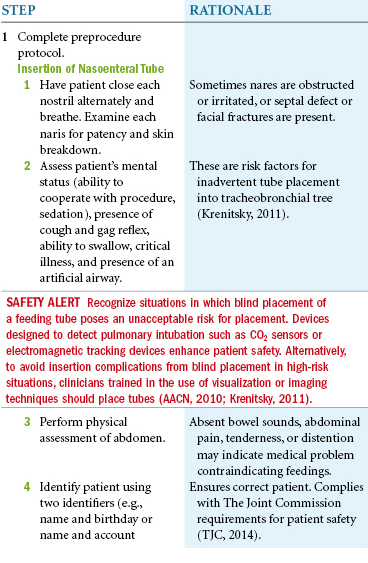
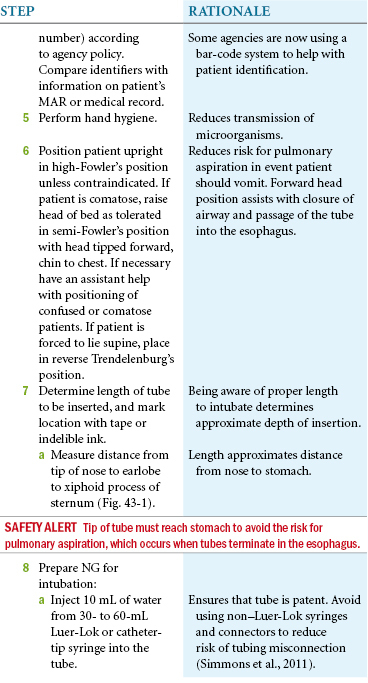
Placement of a feeding tube requires a physician’s order. Patients with facial injuries or craniofacial surgery should not receive a nasogastric (NG) feeding tube. Tubes have been found in the wrong place (e.g., brain) when this is ignored. Tubes should not be used until correct placement is verified by radiological examination.
Delegation Considerations
The skill of feeding tube insertion cannot be delegated to nursing assistive personnel (NAP). However, NAP may help with patient positioning and comfort measures during tube insertion.
Equipment
▪ 60-mL Luer-Lok or catheter-tip syringe
▪ Stethoscope and pulse oximeter
▪ Hypoallergenic tape, semipermeable (transparent) dressing, or tube fixation device
▪ Tincture of benzoin or other skin barrier protectant
▪ pH indicator strip (scale 0.0 to 11.0)
▪ Cup of water and straw or ice chips (for patients able to swallow)
▪ Suction equipment in case of aspiration
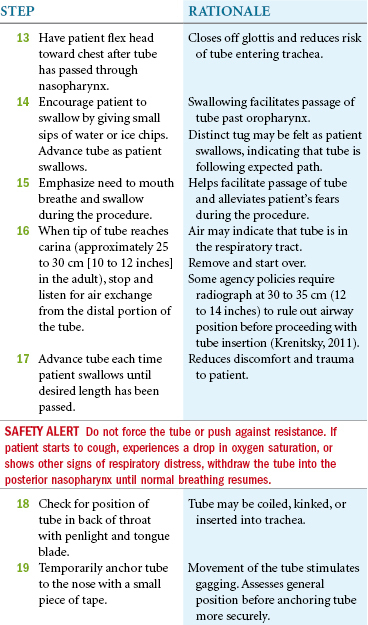
▪ Penlight to check placement in nasopharynx