Intrapartum
Basic Definitions
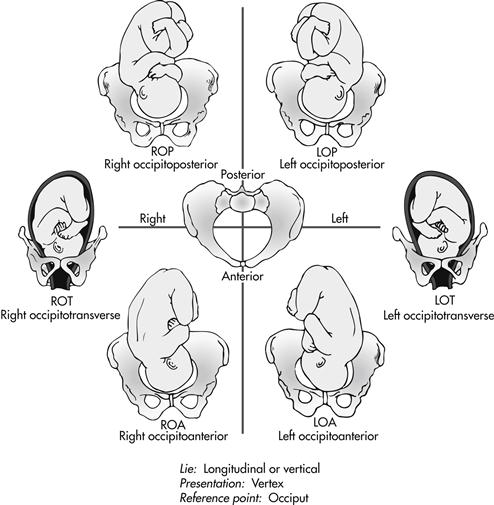
position: relationship of a reference point on the presenting part of the fetus, such as the occiput, sacrum, chin, or scapula, to its location in the front, back, or sides of the maternal pelvis (Fig. 3-1)
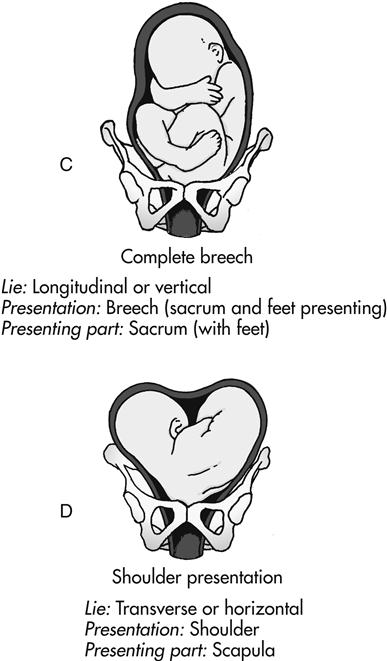
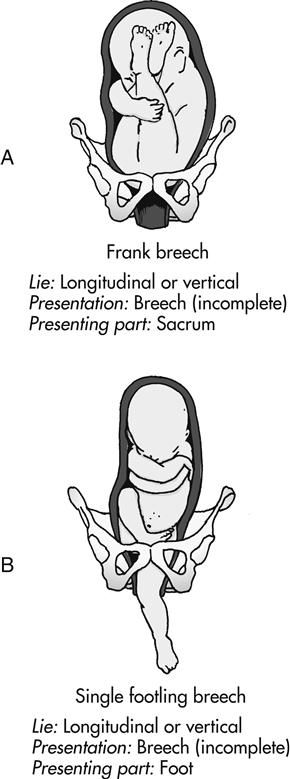
presentation: that part of the fetus that first enters the pelvis and lies over the inlet; the three main presentations are cephalic (head first), breech (buttocks or feet first), and shoulder (Fig. 3-2)
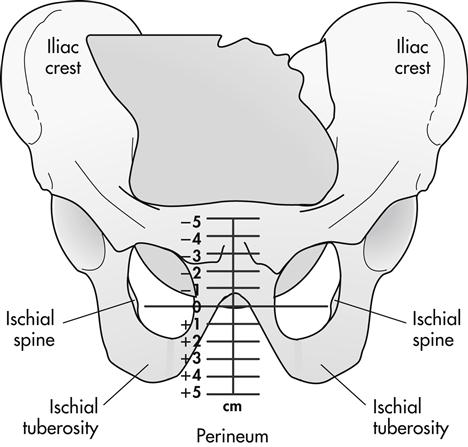
station: relationship of the presenting fetal part to an imaginary line drawn between the maternal ischial spines; a measure of the degree of descent of the presenting part of the fetus through the birth canal; the placement of the presenting part is measured in centimeters above or below the ischial spines (Fig. 3-3)
Stages of Labor



The length of the first stage of labor varies greatly but is usually shorter as parity increases. Full dilation may occur in less than 1 hour in some multiparous pregnancies. In first-time pregnancy, complete dilation of the cervix can take up to 20 hours.


The second stage of labor lasts an average of 20 minutes for a multiparous woman and 50 minutes for a nulliparous woman.
Management of the First Stage of Labor
Admission to the Labor and Birth Unit

 Use the agency’s triage and/or admission forms (may be paper or electronic) as a guide for obtaining important assessment information. These forms usually address:
Use the agency’s triage and/or admission forms (may be paper or electronic) as a guide for obtaining important assessment information. These forms usually address:
 Chief complaint: “Why did you come at this time?”
Chief complaint: “Why did you come at this time?”


 Contraction status (time of onset, frequency, duration, intensity, resting tone)
Contraction status (time of onset, frequency, duration, intensity, resting tone)
 Fetal heart rate (FHR) and pattern
Fetal heart rate (FHR) and pattern
 Presence and character of vaginal discharge or show
Presence and character of vaginal discharge or show




 Vaginal examination to determine cervical effacement, dilation, and fetal station
Vaginal examination to determine cervical effacement, dilation, and fetal station
 Perform basic laboratory and diagnostic tests according to hospital protocol. These commonly include the following:
Perform basic laboratory and diagnostic tests according to hospital protocol. These commonly include the following:



 Rapid group B streptococci (GBS) test (if third-trimester test results are not available)
Rapid group B streptococci (GBS) test (if third-trimester test results are not available)
 Rapid human immunodeficiency virus (HIV) test (if third-trimester test results are not available)
Rapid human immunodeficiency virus (HIV) test (if third-trimester test results are not available)
 Review the prenatal record to determine the following:
Review the prenatal record to determine the following:

 Problems during the current pregnancy
Problems during the current pregnancy
 Laboratory and/or diagnostic test results
Laboratory and/or diagnostic test results

 Type of childbirth preparation
Type of childbirth preparation
 Determine if the woman is in true labor. See Box 3-1 for differences in true and false labor.
Determine if the woman is in true labor. See Box 3-1 for differences in true and false labor.

Box 3-1
Differences in True and False Labor
True Labor










False Labor

 Occur irregularly or become regular only temporarily
Occur irregularly or become regular only temporarily
 Often stop with walking or position change
Often stop with walking or position change
 Can be felt in the back or abdomen above the navel
Can be felt in the back or abdomen above the navel
 Often can be stopped through the use of comfort measures
Often can be stopped through the use of comfort measures
 Cervix (by vaginal examination)
Cervix (by vaginal examination)
 May be soft but there is no significant change in effacement or dilation or evidence of bloody show
May be soft but there is no significant change in effacement or dilation or evidence of bloody show
 Is often in a posterior position
Is often in a posterior position


Common Characteristics of the First Stage of Labor
Common appearance and behavior of women during each phase of the first stage of labor are listed in Box 3-2.
Procedure
Tests for Rupture of Membranes
Nitrazine Test FOR pH

Procedure



Read Results

| Yellow | pH 5.0 |
| Olive-yellow | pH 5.5 |
| Olive-green | pH 6.0 |

| Blue-green | pH 6.5 |
| Blue-gray | pH 7.0 |
| Deep blue | pH 7.5 |



Document Results

Test for Ferning or Fern Pattern








Document Results

BOX 3-2
Common Characteristics of First-Stage Labor
Latent Phase (dilation of cervix 0-3 cm; contractions 30-45 sec long, 5-30 min apart, mild to moderate intensity; duration of phase about 6-8 hr)








Active Phase (dilation of cervix 4-7 cm; contractions 40-70 sec long, 3-5 min apart, moderate to strong intensity; duration of phase about 3-6 hr)







Transition Phase (dilation of cervix 8-10 cm; contractions 45-90 sec long, 2-3 min apart, strong intensity; duration of phase about 20-40 min)
 Pain described as severe, with backache common
Pain described as severe, with backache common
 May voice frustration, fear of loss of control, and irritability
May voice frustration, fear of loss of control, and irritability
 Expresses doubt about ability to continue
Expresses doubt about ability to continue

 Experiences amnesia between contractions
Experiences amnesia between contractions

 Nausea and vomiting, especially if hyperventilating
Nausea and vomiting, especially if hyperventilating

 Circumoral pallor, perspiration on forehead and upper lip
Circumoral pallor, perspiration on forehead and upper lip


Nursing Care in the First Stage of Labor
Nursing care for women during the first stage of labor is described in Box 3-3.
BOX 3-3
Nursing Care in First-Stage Labor
Assessment

 Perform every 30 to 60 min: maternal blood pressure, pulse, and respirations
Perform every 30 to 60 min: maternal blood pressure, pulse, and respirations

 Assess temperature every 4 hours until membranes rupture, then every 2 hr
Assess temperature every 4 hours until membranes rupture, then every 2 hr
 Perform vaginal examination as needed to identify progress
Perform vaginal examination as needed to identify progress


 Perform every 30 min: maternal blood pressure, pulse, and respirations
Perform every 30 min: maternal blood pressure, pulse, and respirations

 Assess temperature every 4 hr until membranes rupture, then every 2 hr
Assess temperature every 4 hr until membranes rupture, then every 2 hr
 Perform vaginal examination as needed to identify progress
Perform vaginal examination as needed to identify progress


 Perform every 15 to 30 min: maternal blood pressure, pulse, and respirations
Perform every 15 to 30 min: maternal blood pressure, pulse, and respirations
 Perform every 15 to 30 min, depending on risk status: FHR and pattern
Perform every 15 to 30 min, depending on risk status: FHR and pattern
 Assess every 10 to 15 min: uterine activity, vaginal show
Assess every 10 to 15 min: uterine activity, vaginal show
 Assess temperature every 4 hr until membranes rupture, then every 2 hr
Assess temperature every 4 hr until membranes rupture, then every 2 hr
 Perform vaginal examination as needed to identify progress
Perform vaginal examination as needed to identify progress

Interventions


 Discuss process of labor and what to expect
Discuss process of labor and what to expect
 Keep woman/couple informed regarding progress
Keep woman/couple informed regarding progress
 Demonstrate breathing and relaxation techniques and comfort measures as needed
Demonstrate breathing and relaxation techniques and comfort measures as needed
 Create a calm, relaxing, safe environment
Create a calm, relaxing, safe environment
 Offer fluids as desired and ordered to maintain hydration; initiate intravenous fluids if ordered
Offer fluids as desired and ordered to maintain hydration; initiate intravenous fluids if ordered
 Assist with activity and position changes, emphasizing upright positions and movement
Assist with activity and position changes, emphasizing upright positions and movement


 Inform woman/couple regarding progress
Inform woman/couple regarding progress
 Encourage and assist with nonpharmacologic measures to enhance progress and relieve discomfort
Encourage and assist with nonpharmacologic measures to enhance progress and relieve discomfort

 Offer fluids as desired and ordered to maintain hydration; initiate intravenous fluids if ordered
Offer fluids as desired and ordered to maintain hydration; initiate intravenous fluids if ordered
 Assist with activity and position changes, emphasizing upright positions and movement
Assist with activity and position changes, emphasizing upright positions and movement
 Help to rest and relax between contractions
Help to rest and relax between contractions

 Assist with hygienic measures: oral care, perineal cleansing
Assist with hygienic measures: oral care, perineal cleansing
 Provide emotional support and encouragement; provide positive reinforcement of her efforts
Provide emotional support and encouragement; provide positive reinforcement of her efforts

 Inform woman/couple regarding progress
Inform woman/couple regarding progress
 Encourage and assist with nonpharmacologic measures to enhance progress and relieve discomfort
Encourage and assist with nonpharmacologic measures to enhance progress and relieve discomfort

 Offer fluids as desired and ordered to maintain hydration; initiate intravenous fluids if ordered
Offer fluids as desired and ordered to maintain hydration; initiate intravenous fluids if ordered
 Assist with activity and position changes, emphasizing upright positions and movement
Assist with activity and position changes, emphasizing upright positions and movement
 Help to rest and relax between contractions
Help to rest and relax between contractions

 Assist with hygienic measures: oral care, perineal cleansing
Assist with hygienic measures: oral care, perineal cleansing
 Provide emotional support and encouragement; provide positive reinforcement of her efforts
Provide emotional support and encouragement; provide positive reinforcement of her efforts
Fetal Assessment During Labor
Because labor is a period of physiologic stress for the fetus, frequent monitoring of fetal status is part of the nursing care during labor. The goals of intrapartum FHR monitoring are to identify and differentiate the normal (reassuring) patterns from the abnormal (nonreassuring) patterns, which can be indicative of fetal compromise. Fetal well-being during labor can be assessed by the response of the FHR to uterine contractions.
Monitoring Techniques
Intermittent Auscultation (IA)
 Uses listening to fetal heart sounds at periodic intervals to assess the FHR
Uses listening to fetal heart sounds at periodic intervals to assess the FHR




 Box 3-4 describes how to perform IA.
Box 3-4 describes how to perform IA.
Uterine Activity (UA) Assessment





Electronic Fetal Monitoring (EFM)
There are two modes of electronic FHR and contraction monitoring: external and internal. See Table 3-1 for differences in these monitoring modes.
TABLE 3-1
External and Internal Modes of Monitoring
| EXTERNAL MODE | INTERNAL MODE |
| FETAL HEART RATE | |
| Ultrasound transducer: High-frequency sound waves reflect mechanical action of the fetal heart. Noninvasive. Does not require rupture of membranes or cervical dilation. Used during both the antepartum and intrapartum periods. | Spiral electrode: Converts the fetal ECG as obtained from the presenting part to the FHR via a cardiotachometer. Can be used only when membranes are ruptured and the cervix is sufficiently dilated during the intrapartum period. Electrode penetrates into fetal presenting part by 1.5 mm and must be attached securely to ensure a good signal. |
| UTERINE ACTIVITY | |
| Tocotransducer: Monitors frequency and duration of contractions by means of a pressure-sensing device applied to the maternal abdomen. Used during both the antepartum and intrapartum periods. | Intrauterine pressure catheter (IUPC): Monitors the frequency, duration, and intensity of contractions. The two types of IUPCs are a fluid-filled system and a solid catheter. Both measure intrauterine pressure at the catheter tip and convert the pressure into millimeters of mercury on the uterine activity panel of the strip chart. Both can be used only when membranes are ruptured and the cervix is sufficiently dilated during the intrapartum period. |

Standardized Definitions for FHR Monitoring
Baseline Patterns
Bradycardia: baseline FHR less than 110 beats/min and lasting for 10 minutes or longer
Tachycardia: baseline FHR more than 160 beats/min and lasting for 10 minutes or longer
Causes, clinical significance, and nursing interventions for tachycardia and bradycardia are listed in Table 3-2.
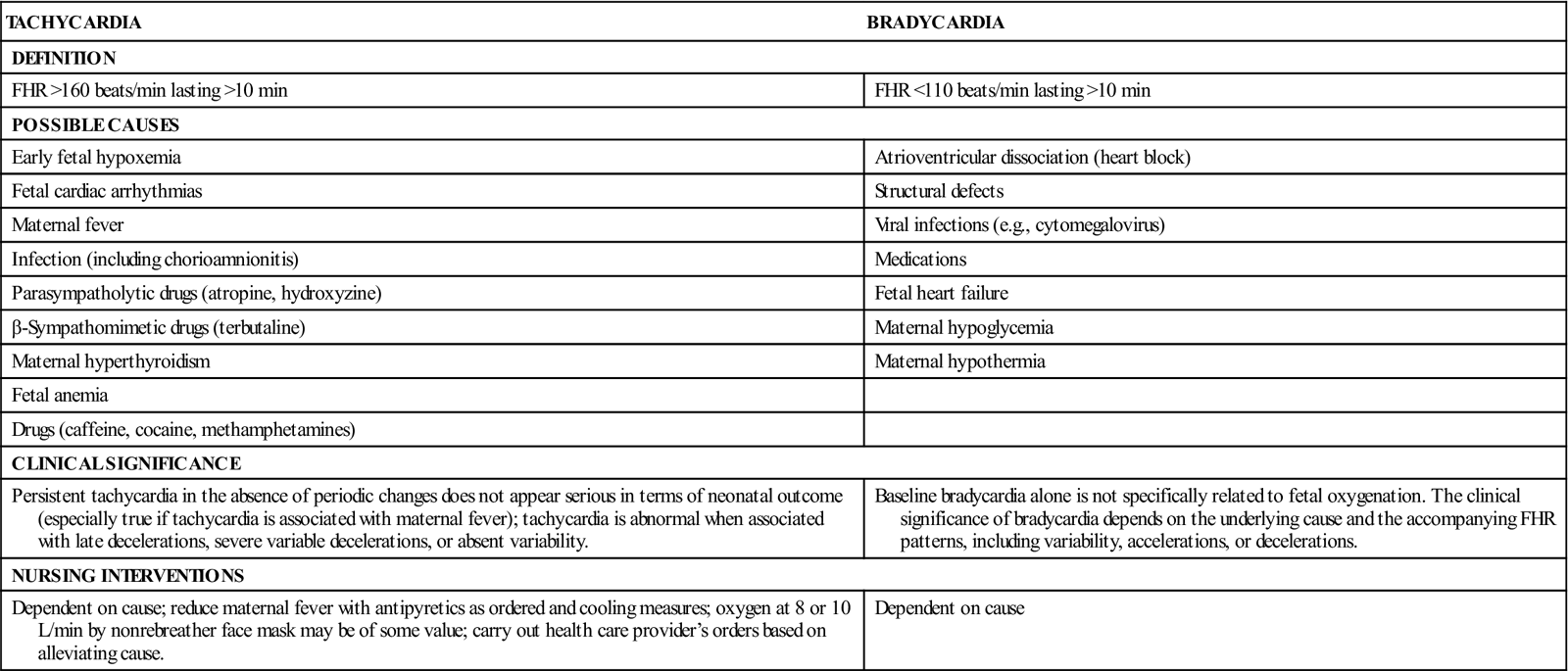
TABLE 3-2
| TACHYCARDIA | BRADYCARDIA |
| DEFINITION | |
| FHR >160 beats/min lasting >10 min | FHR <110 beats/min lasting >10 min |
| POSSIBLE CAUSES | |
| Early fetal hypoxemia | Atrioventricular dissociation (heart block) |
| Fetal cardiac arrhythmias | Structural defects |
| Maternal fever | Viral infections (e.g., cytomegalovirus) |
| Infection (including chorioamnionitis) | Medications |
| Parasympatholytic drugs (atropine, hydroxyzine) | Fetal heart failure |
| β-Sympathomimetic drugs (terbutaline) | Maternal hypoglycemia |
| Maternal hyperthyroidism | Maternal hypothermia |
| Fetal anemia | |
| Drugs (caffeine, cocaine, methamphetamines) | |
| CLINICAL SIGNIFICANCE | |
| Persistent tachycardia in the absence of periodic changes does not appear serious in terms of neonatal outcome (especially true if tachycardia is associated with maternal fever); tachycardia is abnormal when associated with late decelerations, severe variable decelerations, or absent variability. | Baseline bradycardia alone is not specifically related to fetal oxygenation. The clinical significance of bradycardia depends on the underlying cause and the accompanying FHR patterns, including variability, accelerations, or decelerations. |
| NURSING INTERVENTIONS | |
| Dependent on cause; reduce maternal fever with antipyretics as ordered and cooling measures; oxygen at 8 or 10 L/min by nonrebreather face mask may be of some value; carry out health care provider’s orders based on alleviating cause. | Dependent on cause |
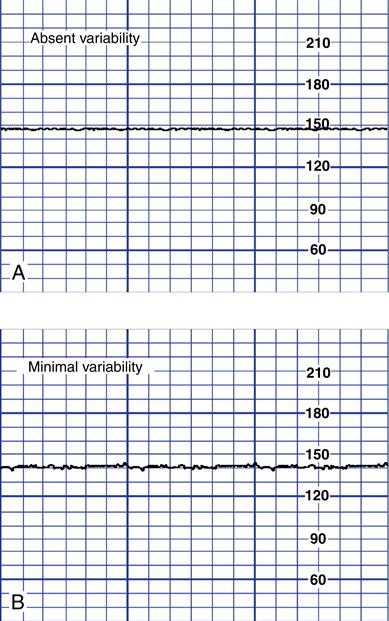
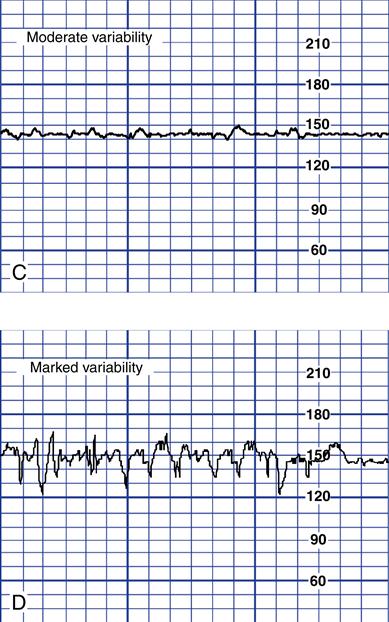
FHR variability: normal irregularity of fetal cardiac rhythm or fluctuations from the baseline FHR of two cycles or more; the four possible categories of variability are absent, minimal, moderate, and marked. Figure 3-4 shows the four possible categories of variability.
Periodic and Episodic Patterns
Figure 3-5 shows an example of accelerations. Box 3-5 lists causes, clinical significance, and nursing interventions for accelerations.
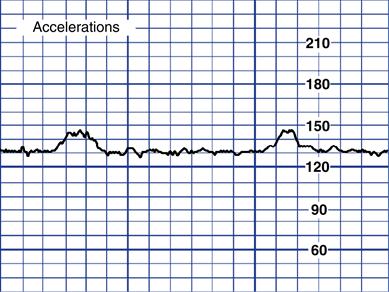
BOX 3-5
Causes










Clinical Significance
Normal pattern. Acceleration with fetal movement signifies fetal well-being representing fetal alertness or arousal states.
Nursing Interventions
None required
Figure 3-6 shows an example of early decelerations. Box 3-6 lists causes, clinical significance, and nursing interventions for early decelerations.
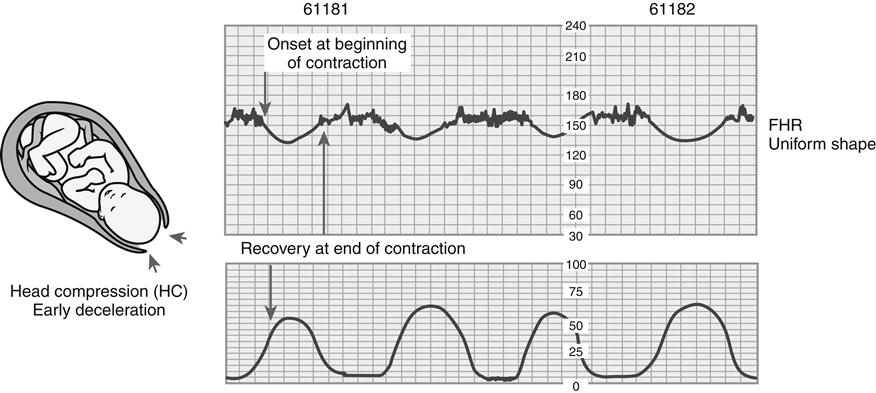
BOX 3-6
Cause
Head compression resulting from the following:




Clinical Significance
Normal pattern. Not associated with fetal hypoxemia, acidemia, or low Apgar scores
Nursing Interventions
None required
Figure 3-7 shows an example of late decelerations. Box 3-7 lists causes, clinical significance, and nursing interventions for late decelerations.
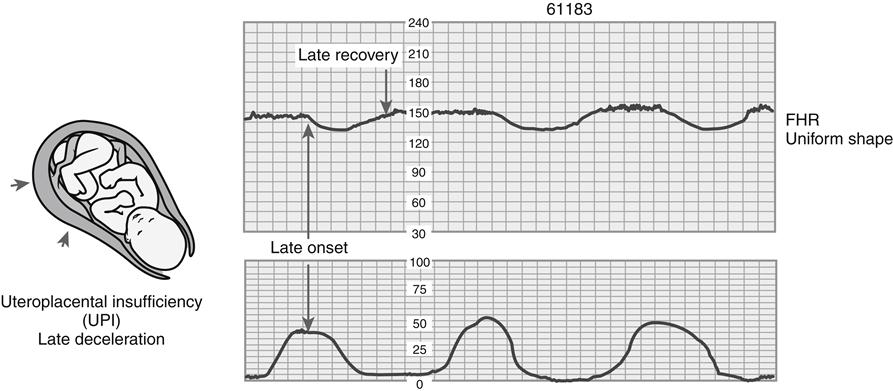
BOX 3-7
Cause
Uteroplacental insufficiency caused by the following:










Clinical Significance
Abnormal pattern associated with fetal hypoxemia, acidemia, and low Apgar scores; considered ominous if persistent and uncorrected, especially when associated with fetal tachycardia and loss of variability
Nursing Interventions
The usual priority is as follows:
1. Change maternal position (lateral).
2. Correct maternal hypotension by elevating legs.
3. Increase rate of maintenance intravenous solution.
4. Palpate uterus to assess for tachysystole.
5. Discontinue oxytocin if infusing.
6. Administer oxygen at 8-10 L/min by nonrebreather face mask.
7. Notify physician or nurse-midwife.
8. Consider internal monitoring for a more accurate fetal and uterine assessment.
9. Assist with birth (cesarean or vaginal assisted) if pattern cannot be corrected.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


