Section 3 Identification of patient problems
3.1 Holistic approaches to care
 The recognition that patients are whole people and cannot be viewed in reductionist terms.
The recognition that patients are whole people and cannot be viewed in reductionist terms.
 The whole cannot be understood merely by isolating and examining its parts.
The whole cannot be understood merely by isolating and examining its parts.

 The environment within which individuals live must be included.
The environment within which individuals live must be included.
 That people live in cultural and social communities.
That people live in cultural and social communities.
 People have networks of relationships with others, most notably within the family.
People have networks of relationships with others, most notably within the family.
 That individuals have sexual needs as well as physical, psychological and social needs.
That individuals have sexual needs as well as physical, psychological and social needs.




Nursing process
 Assessment – all the patient information is gathered and examined to obtain all the facts necessary to determine the patient’s health status and identify problems.
Assessment – all the patient information is gathered and examined to obtain all the facts necessary to determine the patient’s health status and identify problems.


 Implementation – putting the plan into action, which involves the following activities:
Implementation – putting the plan into action, which involves the following activities:
 Evaluation – determining how well the plan has worked and whether any changes need to be made.
Evaluation – determining how well the plan has worked and whether any changes need to be made.
Observation of the patient
 Are they on a trolley or in a wheelchair?
Are they on a trolley or in a wheelchair?
 Are they walking using a stick or do they have a limp or an unsteady gait?
Are they walking using a stick or do they have a limp or an unsteady gait?
 Facial colour, pallor, flushed or cyanosed.
Facial colour, pallor, flushed or cyanosed.
 Respiratory difficulty, rapid or shallow breathing.
Respiratory difficulty, rapid or shallow breathing.
 Cool, moist or dehydrated skin.
Cool, moist or dehydrated skin.
 Ischaemia of the eyelids, lips, gums and tongue.
Ischaemia of the eyelids, lips, gums and tongue.
 Facial expression indicating pain, anxiety, fear, anger.
Facial expression indicating pain, anxiety, fear, anger.
 Oedema of the feet, legs or sacral area.
Oedema of the feet, legs or sacral area.
 Increased or decreased body weight; loose-fitting clothing or false teeth.
Increased or decreased body weight; loose-fitting clothing or false teeth.



Interviewing the patient
 Assess relevant health history, enquiring if there is any family history, any episodes of fatigue, restlessness, syncope or confusion.
Assess relevant health history, enquiring if there is any family history, any episodes of fatigue, restlessness, syncope or confusion.



 Determine any religious beliefs or preferences, sleeping and eating patterns.
Determine any religious beliefs or preferences, sleeping and eating patterns.
 Ask about psychological status, e.g. recent bereavement, eating habits.
Ask about psychological status, e.g. recent bereavement, eating habits.
 Determine social status of the patient.
Determine social status of the patient.

Patient communication
The communication process comprises five elements:
1. The sender or encoder of the message.
3. The receiver or decoder of the message.
4. Feedback that the receiver conveys to the sender.
When planning to meet patients’ communication needs there are six essential areas to include:
1. Orientation to the time, day, date, place, people, environment and procedures.
2. Specific patient teaching on any aspect of care.
3. Adopting methods to overcome patients’ sensory deficits.
4. Comforting patients who are confused or hallucinating.
5. Communications which maintain the patient’s personal identity.
Resources, nursing actions and aids which can be used in connection with these six areas are suggested in Table 3.1.
Table 3.1 Communication aids to meet patient needs (Manley & Bellman 2000)
| Essential areas of | Resource/aid/nursing planning action |
|---|---|
| Orientation to time, place, person, people, environment and procedures | |
| Communication which maintains | |
| Special patient teaching | |
| Overcoming sensory deficits | |
| Comforting patients | |
| Helping communication of |
Barriers to and interference with communication can occur at any point in the process. A summary of potential problems relating to the patient’s reception of messages from the nurse in acute hospital settings is provided in Box 3.1.
Box 3.1 Potential problems relating to communicating in practice
| Environment | |
| Distortion of the message | |
| Distractions | |
| Patient | |
| Psychological | |
| Physical | |
| Social | |
3.2 Assessment

 Episodes of fatigue, restlessness, syncope or confusion.
Episodes of fatigue, restlessness, syncope or confusion.


 Religious beliefs or preferences.
Religious beliefs or preferences.

 Social status, to determine stress levels, diet, income, family concerns and job status.
Social status, to determine stress levels, diet, income, family concerns and job status.
Autonomic nervous system
The sympathetic nervous system:
 Is active in response to stressors.
Is active in response to stressors.
 Is responsible for stimulating smooth muscle fibres to contract (i.e. excitation).
Is responsible for stimulating smooth muscle fibres to contract (i.e. excitation).

The parasympathetic nervous system:
 Is active in response to stressors.
Is active in response to stressors.
 Causes relaxation (i.e. inhibition) and is most active during sleep and rest.
Causes relaxation (i.e. inhibition) and is most active during sleep and rest.

The Glasgow Coma Scale
 Record conscious level and the activity of the ANS or mental state.
Record conscious level and the activity of the ANS or mental state.
 Assess consciousness and standardize clinical observations of patients with impaired consciousness.
Assess consciousness and standardize clinical observations of patients with impaired consciousness.
 Monitor the progress of head-injured patients and those undergoing intracranial surgery.
Monitor the progress of head-injured patients and those undergoing intracranial surgery.
 Detect any other neurological disorder (cerebral vascular accident, encephalitis, meningitis).
Detect any other neurological disorder (cerebral vascular accident, encephalitis, meningitis).
 Minimize variation and subjectivity in the clinical assessment of patients.
Minimize variation and subjectivity in the clinical assessment of patients.

It focuses on the evaluation of three parameters: eye opening, motor response and verbal response (Table 3.2). The patient’s best achievement is recorded for each parameter. The scores are then added together to give an overall assessment of the patient’s neurological status. A score of 15 represents the most responsive while a score of 3 is the least responsive.
Table 3.2 The three modes of behaviour used in the GCS (Edwards, 2001)
| Response | Description | Scale |
|---|---|---|
| Best eye opening response | Spontaneously: opens eyes spontaneously | 4 |
| To speech: opens to verbal stimuli; not necessarily to command of ‘open your eyes’, a verbal stimulus may be normal, repeated or even loud | 3 | |
| To pain: does not open eyes to previous stimuli, opens eyes to central painful stimuli | 2 | |
| None: does not open eyes to any stimulus | 1 | |
| Best verbal response | Orientated to time, place and person | 5 |
| Disorientated and confused to any of the following: time, place or person; ability to hold a conversation but not accurately answering questions | 4 | |
| Inappropriate words: uses words or phrases making little or no sense, words may be said at random, shouting or swearing | 3 | |
| Incomprehensible sounds: makes unintelligible sounds (moans and groans) | 2 | |
| No response: makes no sounds or speech | 1 | |
| Other: if patient is intubated or has a tracheotomy, document ETT or trach; if dysphasia or aphasic document D or A | ||
| Best motor response | Obeys verbal commands: follows commands, even if weakly | 6 |
| Localizes to painful stimuli: attempts to locate or remove painful stimulus | 5 | |
| Withdraws from painful stimuli: moves away from painful stimulus or may bend or flex arm towards the source of pain but does not actually localize or remove source of pain | 4 | |
| Abnormal flexion and adduction of arms coupled with extensions of legs and plantar flexion of feet (decorticate posturing) | 3 | |
| Abnormal extension, adduction and internal rotation of upper and lower extremities (decerebrate posturing) | 2 | |
| No response, even to painful stimulus | 1 |
Painful stimulus

 Peripheral painful stimulation:
Peripheral painful stimulation:
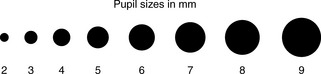
Pupil size and reaction to light
 The pupil size (Fig. 3.1) – average pupil size is 2–5 mm.
The pupil size (Fig. 3.1) – average pupil size is 2–5 mm.
 The pupil reaction to light: brisk, sluggish or fixed.
The pupil reaction to light: brisk, sluggish or fixed.
 The shape of the pupil – should be round.
The shape of the pupil – should be round.
 If both pupils react equally to light and are equal in size.
If both pupils react equally to light and are equal in size.
When undertaking the pupillary response the following should be observed:






Observation of vital signs
The last section of the GCS is the observation of vital signs:
 A high temperature can be due to damage to the hypothalamus, which increases the cerebral metabolic oxygen requirement, an unwanted complication when oxygenation of the brain may already be depleted.
A high temperature can be due to damage to the hypothalamus, which increases the cerebral metabolic oxygen requirement, an unwanted complication when oxygenation of the brain may already be depleted.






Stress
1. The alarm reaction – widespread physiological response which includes a large outflow into the bloodstream of adrenal hormones in an attempt to defend the body from the stresssor.
2. Resistance or adaptation – where an attempt is made by the body to re-establish equilibrium and to regain control to maintain homeostasis. If the body is unable to re-establish homeostasis because of persistent exposure to the stressor then the third phase will result.
 Hearing the initial diagnosis may be a difficult and stressful process; the fear and anxiety generated by the news may be disruptive and debilitating, making it more difficult for the patient to absorb further information or to make informed choices.
Hearing the initial diagnosis may be a difficult and stressful process; the fear and anxiety generated by the news may be disruptive and debilitating, making it more difficult for the patient to absorb further information or to make informed choices.




 Assessment of recent and current major life events and/or crises, as these may have precipitated the acute illness.
Assessment of recent and current major life events and/or crises, as these may have precipitated the acute illness.

 Recognition that the present acute illness may cause stress in itself, particularly with regard to:
Recognition that the present acute illness may cause stress in itself, particularly with regard to:





Pain
 The visual analogue scale – a straight line, usually 10 cm in length, with one extreme marked ‘no pain at all’ and the other end marked ‘worst possible pain’. Descriptive words may be added.
The visual analogue scale – a straight line, usually 10 cm in length, with one extreme marked ‘no pain at all’ and the other end marked ‘worst possible pain’. Descriptive words may be added.




Once assessed, it is imperative that the pain is treated, as a failure to relieve pain is morally and ethically unacceptable (see Section 5 for pain relief). Pain can have a detrimental effect on a patient’s condition and can significantly slow recovery. The under-treatment of pain can lead to:
 Decreased tidal volumes and alveolar ventilation, leading to decreased oxygen delivery to organs.
Decreased tidal volumes and alveolar ventilation, leading to decreased oxygen delivery to organs.

 Avoidance of movement, leading to an increased risk of deep vein thrombosis and pulmonary embolism.
Avoidance of movement, leading to an increased risk of deep vein thrombosis and pulmonary embolism.


Under-management of pain
Healthcare professionals





Individual patient
 Low expectations of pain management and a belief that pain is inevitable.
Low expectations of pain management and a belief that pain is inevitable.
 Inappropriate beliefs regarding pain management strategies (fear of addiction and tolerance).
Inappropriate beliefs regarding pain management strategies (fear of addiction and tolerance).
 Beliefs that side-effects of medication are inevitable (sedation).
Beliefs that side-effects of medication are inevitable (sedation).
Good pain relief can reduce these responses to pain, and lead to a safer and improved recovery.





