Section 3 Children’s nursing interventions
3.1 Interventions
Blood transfusion therapy
The Rhesus (Rh) system


The Rh D factor is significant in both blood transfusions and pregnancy:


Changes in blood begin within 24 hours of storage, and continue throughout the entire 21 days, after which blood is considered outdated (Edwards 1998). Box 3.1 show the changes that occur in stored blood.
Blood transfusion reactions (TF)
 When mismatched blood is infused, a transfusion reaction occurs and the donor and recipient’s red blood cells are attacked by the recipient’s immune system.
When mismatched blood is infused, a transfusion reaction occurs and the donor and recipient’s red blood cells are attacked by the recipient’s immune system.
 Transfusion reaction can occur with the infusion with as little as 10–15 ml.
Transfusion reaction can occur with the infusion with as little as 10–15 ml.


If any serious adverse reaction or event occurs during or after a blood transfusion it should be reported on the serious adverse blood reactions and events (SABRE) system, accessed by the serious hazards of transfusion (SHOT) website at http://www.shotuk.org.

Nurses have to be vigilant in checking:
 The correct blood group and Rh D antigen factor
The correct blood group and Rh D antigen factor
 Confirming with the parent or child the identity
Confirming with the parent or child the identity
 Checking the ID band, e.g. date of birth, hospital number (no wristband – no transfusion)
Checking the ID band, e.g. date of birth, hospital number (no wristband – no transfusion)
 Donor number matches, CMV negative
Donor number matches, CMV negative
 Integrity of the bag, e.g. no damage has occurred
Integrity of the bag, e.g. no damage has occurred

 Kell or other antibodies/CMV negative
Kell or other antibodies/CMV negative



Other blood product derivatives
 Packed red cells (whole blood from which most of the plasma has been removed) is generally only used to treat anaemia.
Packed red cells (whole blood from which most of the plasma has been removed) is generally only used to treat anaemia.

For a more detailed account of blood products see Table 3.1.
Table 3.1 Current blood products
| Blood product | Constituents | Uses |
|---|---|---|
| Whole blood (510 ± 45 ml) | Use is restricted to circumstances where red blood cells as well as plasma proteins are needed i.e. where large amounts of blood are lost. | Ideal in hypovolaemic shock, since it increases both oxygen carrying capacity and expands circulating volume. |
| Packed cells (280 ± 60 ml) | This is whole blood, but the majority of the plasma has been removed. It contains half the volume of whole blood, less sodium, potassium, albumin and citrate. Does contain some white blood cells and platelets. | Ideal in chronic anaemia, sickle cell disease, thalassaemia and renal disease. It is not recommended in iron deficiency and vitamin B12 or folate deficiency as these should be treated with the appropriate vitamin e.g. iron tablets. |
| Washed packed cells | These are packed cells with all the white blood cells, platelets and plasma removed. | Indicated for patients who have a long history of transfusion reactions. |
| Fresh frozen plasma (FFP) (200–300 ml) | This is blood product, which is nearly always frozen and contains all the coagulation factors. | Used for the treatment of coagulation deficits. It is not recommended as a volume expander, except in certain neonatal conditions. |
| Cryoprecipitate (20 ± 5 ml) | Prepared from FFP and contains mainly clotting factors (factor VIII and fibrinogen). | Used to treat haemophilia or AIDS patients. |
| Platelets (50 ± 10 ml) | Produced from the residue left over from the production of plasma and leucocyte-depleted red blood cell concentrates. | Indications for use are thrombocytopenia, when platelet content of blood is reduced due to bleeding or diluted following massive transfusion, in acute leukaemia, aplastic anaemia, DIC or sepsis. |
AIDS, acquired immune deficiency syndrome; DIC, disseminated intravascular coagulation.













Fluid replacement therapy
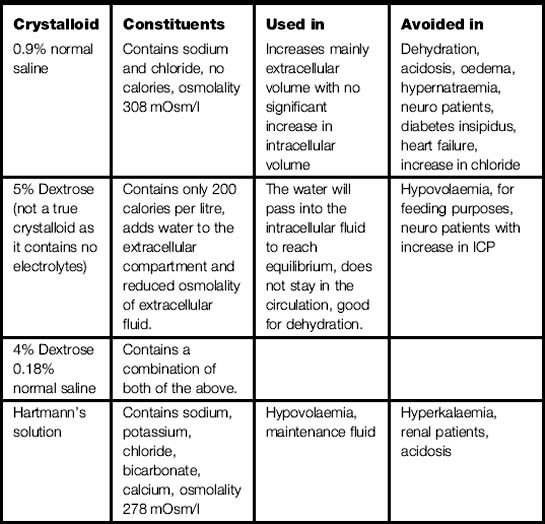
Crystalloid therapy
 Crystalloid solutions used are 5% dextrose (not a true crystalloid as it contains no electrolytes), 0.9% sodium chloride; dextrose saline and Hartmann’s (see Table 3.2).
Crystalloid solutions used are 5% dextrose (not a true crystalloid as it contains no electrolytes), 0.9% sodium chloride; dextrose saline and Hartmann’s (see Table 3.2).
 Any solution that contains electrolytes will influence fluid movement; the most powerful is sodium.
Any solution that contains electrolytes will influence fluid movement; the most powerful is sodium.

Maintenance fluid


Some methods of calculating maintenance fluids:


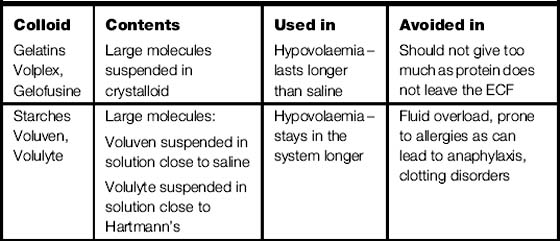
Colloid therapy
 Colloids work as they contain various amounts of large molecules, which draw fluid into the circulation from the intracellular spaces (the largest fluid compartment of the body), increasing circulating volume (volume expanders).
Colloids work as they contain various amounts of large molecules, which draw fluid into the circulation from the intracellular spaces (the largest fluid compartment of the body), increasing circulating volume (volume expanders).
 There are two different types of colloid gelatines and starches (see Table 3.3).
There are two different types of colloid gelatines and starches (see Table 3.3).

 Using colloids in haemorrhage is to restore plasma volume, and improve or maintain oxygen transport.
Using colloids in haemorrhage is to restore plasma volume, and improve or maintain oxygen transport.










Cannulation
A cannula is a vascular device inserted into a peripheral or central vessel to provide:



 relevant anatomy and physiology
relevant anatomy and physiology
 criteria for choosing vein and equipment
criteria for choosing vein and equipment

 health and safety regulations.
health and safety regulations.
 adherence to aseptic technique
adherence to aseptic technique

 adequate information regarding the procedure and complications.
adequate information regarding the procedure and complications.




Considerations when choosing a vein:

 injury, disease or treatment prevent use of a limb
injury, disease or treatment prevent use of a limb
 how the infant/child is positioned
how the infant/child is positioned

 if the infant/child is in shock or dehydrated poor superficial peripheral access may be present
if the infant/child is in shock or dehydrated poor superficial peripheral access may be present
 temperature will influence venous dilatation e.g. if the child is cold, no veins may be visible.
temperature will influence venous dilatation e.g. if the child is cold, no veins may be visible.
 medications can influence choice e.g. anticoagulants, steroids, risk of bruising.
medications can influence choice e.g. anticoagulants, steroids, risk of bruising.
 Consider whether cannula is actually necessary.
Consider whether cannula is actually necessary.

 Choose a site away from a joint.
Choose a site away from a joint.

 Prevent infection of skin flora contamination from nurse to child:
Prevent infection of skin flora contamination from nurse to child:

 Check patency using normal saline.
Check patency using normal saline.


Insertion site checked regularly for signs of:

Table 3.4 Infiltration scoring system
| Grade | Clinical criteria |
|---|---|
| 0 | No symptoms |
| 1 | Skin blanched Oedema 2.5 cm in any direction Cool to touch With or without pain |
| 2 | Skin blanched Oedema 2.5–15 cm in any direction Cool to touch With or without pain |
| 3 | Skin blanched, translucent Gross oedema 15 cm in any direction Cool to touch Mild to moderate pain Possible numbness |
| 4 | Skin blanched, translucent Skin tight, leaking Skin discoloured, bruised, swollen Gross oedema 15 cm in any direction Deep pitting tissue oedema Circulatory impairment Moderate to severe pain Infiltration of any amount of blood product, irritant or vesicant |
Phlebitis
 Acute inflammation of a vein directly linked to the presence of any vascular device.
Acute inflammation of a vein directly linked to the presence of any vascular device.
 Infants may cry or children may report pain.
Infants may cry or children may report pain.
 If treated early enough often the symptoms will resolve without further intervention required.
If treated early enough often the symptoms will resolve without further intervention required.

 Phlebitis can be further classified into mechanical, chemical and infective, depending on the cause:
Phlebitis can be further classified into mechanical, chemical and infective, depending on the cause:
 Treatment is removal of the line and the application of heat to the site and prescribed analgesia
Treatment is removal of the line and the application of heat to the site and prescribed analgesia
Flushing of cannula








Anaphylaxis
 With increased use of medicines and antibacterials, medicine induced anaphylaxis and anaphylactoid reactions have increased.
With increased use of medicines and antibacterials, medicine induced anaphylaxis and anaphylactoid reactions have increased.

Anaphylaxis is often unpredictable and so we need to focus on strategies to decrease risks:
 Ensure detailed patient history and full physical examination.
Ensure detailed patient history and full physical examination.
 Consider the route of the medicine and the rate of the medicine and/or fluid.
Consider the route of the medicine and the rate of the medicine and/or fluid.
 Identification of patients with known causes of anaphylaxis.
Identification of patients with known causes of anaphylaxis.
 Sound knowledge of the medicine, as some cross react and also are contraindicated.
Sound knowledge of the medicine, as some cross react and also are contraindicated.












Oxygen therapy
Hypoxia is oxygen deficiency in the body cells caused by:
 Deficient oxygenation of the blood – due to respiratory disease or chest injuries.
Deficient oxygenation of the blood – due to respiratory disease or chest injuries.
 Inadequate transport of oxygen by haemoglobin – as in anaemia or haemorrhage.
Inadequate transport of oxygen by haemoglobin – as in anaemia or haemorrhage.
 Circulatory inadequacy as in heart disease or emergency situations, e.g. cardiac arrest.
Circulatory inadequacy as in heart disease or emergency situations, e.g. cardiac arrest.
 Inability of cells to use oxygen – rare – an example is cyanide poisoning.
Inability of cells to use oxygen – rare – an example is cyanide poisoning.
 Oxygen toxicity – may follow prolonged periods (over 24 hours) of administration of high (over 50%) concentrations of oxygen.
Oxygen toxicity – may follow prolonged periods (over 24 hours) of administration of high (over 50%) concentrations of oxygen.








Humidified oxygen
Indications for the use of heated humidification systems:
 Patients receiving high concentrations of oxygen (where FiO2 exceeds 40%) for periods of time exceeding 24 hours.
Patients receiving high concentrations of oxygen (where FiO2 exceeds 40%) for periods of time exceeding 24 hours.







Heated humidification




Rewarming procedures
Passive rewarming




Active external rewarming
 Patient’s skin is warmed, using hot baths, hot air blowers or radiant heat. This method can also be used as an adjunct to internal active rewarming. One of the most effective methods is convective warming therapy which forces heated air directly on to the patient’s skin through a disposable blanket.
Patient’s skin is warmed, using hot baths, hot air blowers or radiant heat. This method can also be used as an adjunct to internal active rewarming. One of the most effective methods is convective warming therapy which forces heated air directly on to the patient’s skin through a disposable blanket.












3.2 Maintaining nutrition in children
Effects of nil by mouth and malnutrition
Absorptive and post-absorptive states:
 Absorptive state – process of eating/digestion
Absorptive state – process of eating/digestion
 Post-absorptive state – fasting should be no more than 12 hours as after this time:
Post-absorptive state – fasting should be no more than 12 hours as after this time:




Enteral feeding (EF)

 reduces risk of bacterial translocation
reduces risk of bacterial translocation
 dampens the inflammatory response
dampens the inflammatory response
 reduces complications from sepsis
reduces complications from sepsis



Types of tubes
 Wide bore tube is used initially to allow easy assessment of gastric contents and aspiration typically occurs every 4 hours to assess gastric content/absorption and pH.
Wide bore tube is used initially to allow easy assessment of gastric contents and aspiration typically occurs every 4 hours to assess gastric content/absorption and pH.



Methods of administration




Complications of enteral feeding (EF)
 Altered gut motility, that is absent bowel sounds can lead to gastric and colonic stasis.
Altered gut motility, that is absent bowel sounds can lead to gastric and colonic stasis.
 Effects of sedation and analgesia can lead to ileus/pseudo obstruction and distension.
Effects of sedation and analgesia can lead to ileus/pseudo obstruction and distension.


 Diarrhoea, constipation, large aspirates.
Diarrhoea, constipation, large aspirates.


 Incomplete calorific delivery due to the above.
Incomplete calorific delivery due to the above.

Strategies to avoid complications associated with EF:

















