Care of Patients with Peripheral Nerve and Degenerative Neurologic Disorders
Objectives
1. Compare and contrast the pathophysiology of Parkinson’s disease and myasthenia gravis.
2. Discuss treatments for Parkinson’s disease.
3. Describe the nursing care needed for the patient with Parkinson’s disease.
4. Explain why multiple sclerosis might be difficult to diagnose.
5. Devise a home care plan for the patient with multiple sclerosis.
6. Compile a nursing care plan for the patient with Guillain-Barré syndrome.
7. Identify the differences between Huntington’s disease and amyotrophic lateral sclerosis.
8. Illustrate the signs and symptoms of myasthenia gravis.
9. Compare and contrast the complications of Parkinson’s disease with those of myasthenia gravis.
1. Teach a newly diagnosed patient about the medications for Parkinson’s disease.
2. Teach a patient about the diagnostic tests that might be ordered if multiple sclerosis is suspected.
Key Terms
bradykinesia (brā-dē-kĭ-NĒ-zē-ă, p. 552)
chorea (kă-RĒ-ă, p. 562)
demyelination (dĕ-MĪ-ĕ-lĭ-nā-shŭn, p. 557)
diplopia (dĭ-PLŌ-pē-ă, p. 562)
hyperesthesia (hī-pĕr-ĕs-THĒ-zē-ă, p. 560)
 http://evolve.elsevier.com/deWit/medsurg
http://evolve.elsevier.com/deWit/medsurg
 Parkinson’s Disease
Parkinson’s Disease
Parkinson’s disease (PD) is named after James Parkinson, who first described the syndrome in 1871. PD is considered a major health problem because of its crippling effects. It is a progressive disorder, beginning rapidly at first and then advancing more slowly. It affects more men than women and occurs most frequently after age 60. Approximately 1 million people in the United States are affected with PD, and about 50,000 people in the United States are diagnosed with PD each year.
Etiology
The specific cause of PD is unknown, but it involves degeneration of the dopamine-producing neurons in the substantia nigra of the midbrain, and the presence of Lewy bodies (cytoplasmic inclusions). Genetic susceptibility and environmental toxins appear to play a role. The most common type of PD is idiopathic, that is, the primary or specific cause is not known. Secondary PD can be drug induced, especially by reserpine-type antihypertensives such as methyldopa, phenothiazines, some tranquilizers such as the butyrophenones (e.g., haloperidol [Haldol]), some antiemetics, methamphetamine, and a few other drugs. These drugs block the uptake of dopamine at the receptors in the brain cells, and so may induce PD symptoms. Pesticide and herbicide exposure is largely implicated as a cause of PD.
Pathophysiology
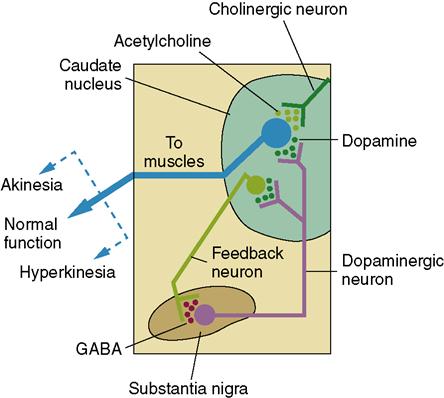
PD affects the extrapyramidal system, in particular the motor structures in the basal ganglia. This is the part of the brain that controls balance and coordination. The basal ganglia are gray matter that is scattered throughout the white matter of the cerebrum beneath the cerebral cortex. Stimulation of the basal ganglia causes muscle tone in the body to be inhibited and allows refined voluntary movements. Two neurotransmitters accomplish this action: dopamine and acetylcholine (ACh) (see Table 22-4 for the action of the common neurotransmitters). ACh-producing neurons transmit excitatory messages throughout the basal ganglia. Dopamine inhibits the function of these neurons so that there can be control of voluntary movement (Figure 25-1). There is usually a balance between these neurotransmitters. The degenerative changes in the basal ganglia lead to a decrease in dopamine. The ACh-secreting neurons remain active, creating an imbalance between excitatory and inhibitory neuronal activity. The excessive excitation of neurons prevents a person from controlling or initiating voluntary movements.
Signs and Symptoms
The onset of PD is gradual and may involve only one side of the body initially. A triad of symptoms is characteristic of PD: tremor, bradykinesia, and rigidity. The first, tremor, occurs when the body is at rest, decreases when there is voluntary movement, and is absent when the patient is asleep. The tremor is most often a “pill-rolling” motion of the thumb against the fingers. This is when there is a circular rubbing of a finger or two as if rolling a piece of string or fuzz into a “pill.” If the patient suffers stress and emotional tension, the tremor becomes more pronounced.
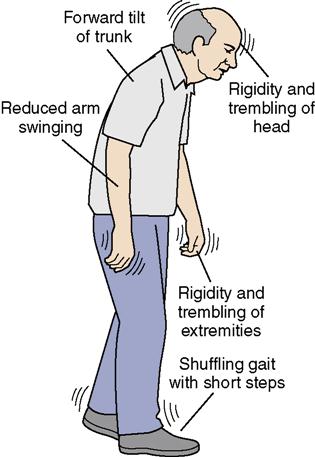
Bradykinesia (condition exhibiting slow movement and speech) produces poor body balance, a characteristic gait, and difficulty initiating movement. The gait is shuffling, with short steps that become quicker (Figure 25-2). There is decreased swinging of the arms when walking. A foot may drag or may be stiff, producing a limp. Earlier in the disease process, the patient may lean slightly to one side, propel forward uncontrollably, or fall backward. In advanced stages there is a stiff, bent-forward posture when walking.
The third symptom is rigidity affecting the skeletal muscles and contributing to postural changes and difficulty in movement. Postural changes affect coordination and balance. The face becomes blank or masklike in appearance with little or no expression. Speech becomes low in tone, monotonous sounding, and slow; enunciation becomes difficult due to the decreased dopamine and the excitatory response from the increased acetylcholine. Drooling may occur. The patient may experience decreased tearing, constipation, incontinence, excessive perspiration, heat intolerance, and decreased sexual ability. PD does not usually affect intellect; however, a percentage of patients do develop a dementia similar to that of Alzheimer’s disease. Mood disturbance does occur, and depression is a problem. Stress tends to make symptoms worse.

A patient comes into the clinic complaining about hand tremors and “stiffness” of the joints that started recently, excessive sweating, and some urinary incontinence. You notice that his gait is abnormal. What would be a priority question you would ask him as you start history taking?
Diagnosis
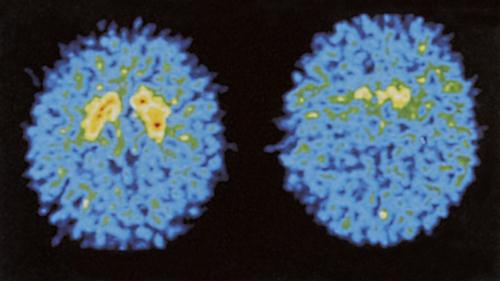
The characteristic symptoms of the disease are used to diagnose the disorder. Laboratory tests usually reveal findings within normal ranges. However, magnetic resonance imaging (MRI) scans of the brain may be performed to rule out other neurologic disorders. Single-photon emission computed tomography (SPECT) can display the reduced uptake of dopamine (Figure 25-3).
Treatment
Treatment of PD usually includes drug therapy, physical therapy, and considerable emotional support. Drug therapy aims to provide dopamine to the basal ganglia and thus reduce symptoms. Anticholinergics, dopamine agonists, and monoamine oxidase inhibitor (MAOI) drugs are used to control symptoms. MAOIs block the metabolism of dopamine, leaving more dopamine in circulation.

Caution When Administering MAOIs
When a patient with Parkinson’s disease has been prescribed selegiline (an MAOI), caution him against eating foods containing tyramine such as aged cheeses, anything fermented, smoked fish or meat, yeast extract, some imported beers, Chianti wine, dietary protein supplements, and soy sauce. Giving meperidine to someone taking an MAOI can cause hyperpyrexia (excessive elevation of temperature) and possible death. Many drugs interact adversely with MAOIs, and the health care provider or pharmacist should be consulted before taking any other drug with an MAOI.
In the early stages of the disease when disability is not evident, selegiline (Eldepryl), a drug that increases dopamine’s action, may be given. When disability is present, L-dioxyphenylalanine (L-dopa, or levodopa) or a combination of levodopa and carbidopa (Sinemet) is given. Sinemet is given in increasing doses until control of the symptoms is achieved; however, side effects can be troublesome (Box 25-1) Various drugs are used either alone or in combination with L-dopa (Table 25-1).

Complementary and Alternative Therapies
Supplements Helpful for Parkinson’s Disease
Nutritional supplements that are helpful for slowing the progression of Parkinson’s disease include the enzyme NADH (nicotinamide adenine dinucleotide; 10 mg), coenzyme Q-10 (100 to 200 mg), phosphatidylserine (200 to 300 mg), and the antioxidants ester-C (1000 mg twice a day), vitamin E as mixed tocopherols (800 to 1200 mg), and alpha-lipoic acid (100 mg twice a day). Physicians sometimes prescribe these supplements in addition to the treatment medications.

What would be appropriate nursing interventions for the patient who is beginning to experience dysphagia?
 Table 25-1
Table 25-1
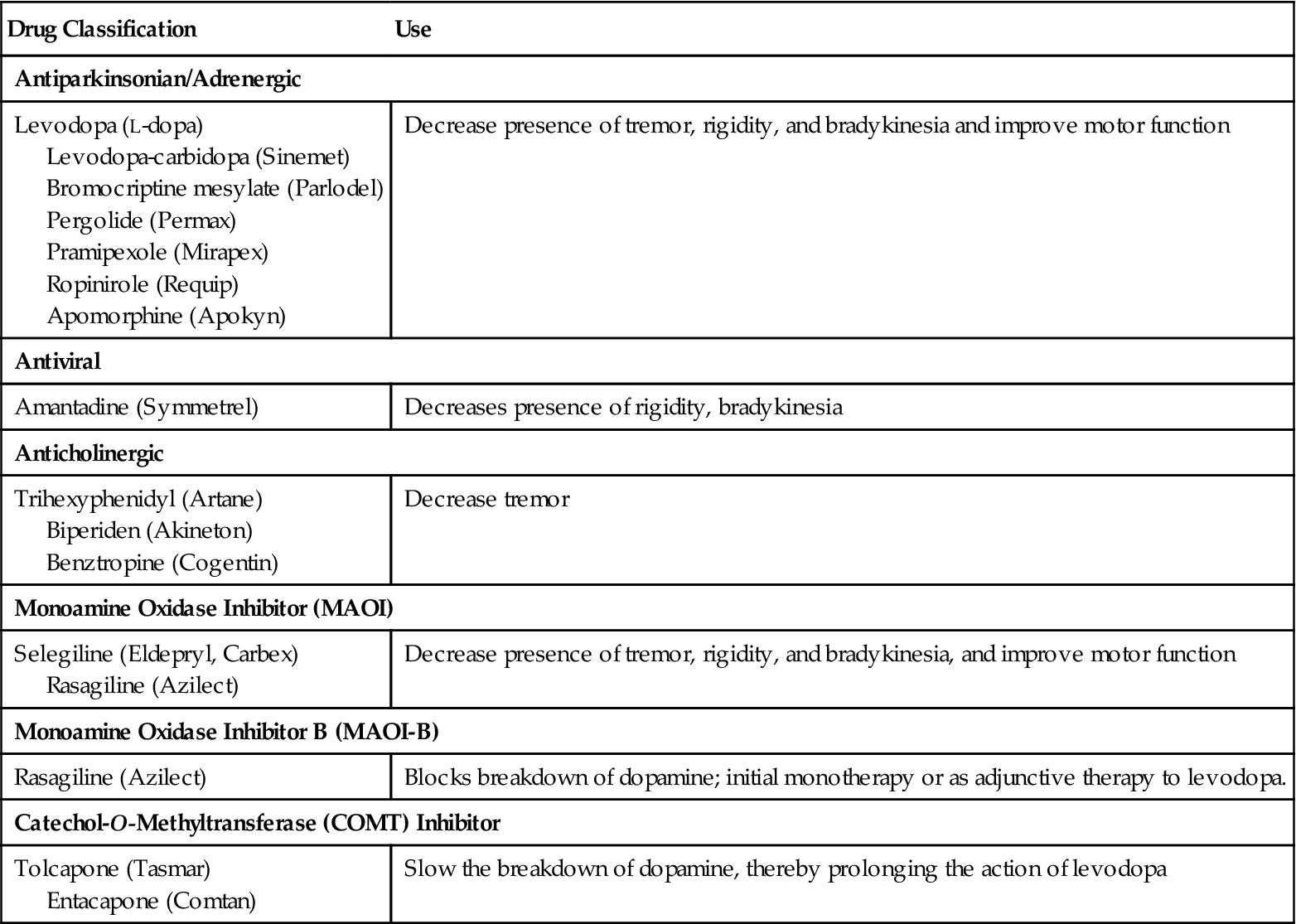
Drugs Commonly Used for Patients with Parkinson’s Disease
| Drug Classification | Use |
| Antiparkinsonian/Adrenergic | |
| Levodopa (L-dopa) Levodopa-carbidopa (Sinemet) Bromocriptine mesylate (Parlodel) Pergolide (Permax) Pramipexole (Mirapex) Ropinirole (Requip) Apomorphine (Apokyn) | Decrease presence of tremor, rigidity, and bradykinesia and improve motor function |
| Antiviral | |
| Amantadine (Symmetrel) | Decreases presence of rigidity, bradykinesia |
| Anticholinergic | |
| Trihexyphenidyl (Artane) Biperiden (Akineton) Benztropine (Cogentin) | Decrease tremor |
| Monoamine Oxidase Inhibitor (MAOI) | |
| Selegiline (Eldepryl, Carbex) Rasagiline (Azilect) | Decrease presence of tremor, rigidity, and bradykinesia, and improve motor function |
| Monoamine Oxidase Inhibitor B (MAOI-B) | |
| Rasagiline (Azilect) | Blocks breakdown of dopamine; initial monotherapy or as adjunctive therapy to levodopa. |
| Catechol-O-Methyltransferase (COMT) Inhibitor | |
| Tolcapone (Tasmar) Entacapone (Comtan) | Slow the breakdown of dopamine, thereby prolonging the action of levodopa |
Surgical Treatment
Stereotactic neurosurgery may be done if the drug therapy fails to assist the patient with PD symptoms. In one such procedure the area in the thalamus that is causing the involuntary movements is destroyed. Microsurgical procedures such as pallidotomy improve rigidity and bradykinesia (Clarke, 2007; WebMD, 2010b).
Other procedures with some success in relieving symptoms include transplanting tissue from the adrenal medulla into the brain, or implanting fetal tissue or stem cells. Stem cells are transplanted into the caudate nucleus of the brain. This is still experimental, but the procedure has shown substantial clinical improvements in motor function (Susman, 2010).
Deep brain stimulation (DBS) uses electrode implants to provide electrical shocks that control tremors by blocking them. The device that delivers the shocks can be adjusted as the patient’s symptoms change or worsen (National Institute of Neurological Diseases and Stroke, 2007). There has been considerable success with DBS, but it is expensive at $10,000 for the implant unit and another $8000 every few years for battery replacement.
Depression is frequent in Parkinson’s patients, but most respond well to a selective serotonin reuptake inhibitor (SSRI) antidepressant.
Complications
Dysphagia may develop and mobility becomes severely limited as the disease progresses. Problems of immobility occur (see Chapter 9). Constipation, urinary incontinence, and insomnia are also common.
Nursing Management
Assessment (Data Collection) and Nursing Diagnosis
A thorough history is gathered and a physical examination is performed for the patient who has or is thought to have PD. Nursing Care Plan 25-1 contains the common nursing diagnoses, expected outcomes, and specific interventions for the patient with PD.

Data Collection for the Patient with Parkinson’s Symptoms
Gather data regarding history by asking the following questions:
• Have you ever had a head injury, meningitis, encephalitis, or cerebrovascular disorder?
• Have you ever been exposed to metals, pesticides, or carbon monoxide for extended periods?
• Do you have a problem with fatigue?
• Have you noticed excessive salivation and problems handling secretions?
• Do you have any trouble swallowing?
• Have you been steadily losing weight?
• Do you suffer with constipation or urinary incontinence?
• Do you have difficulty initiating walking or other movements? Do you fall frequently?
• Has your dexterity decreased? Has your handwriting deteriorated?
• Do you experience pain or cramping?
• Do you have mood swings? Are you depressed? Do you have hallucinations?
Points to cover in physical examination:
• Facial expression or lack thereof
• Evidence of postural hypotension
• Presence of tremor at rest; pill-rolling movements
• Rigidity of body and jerky movements of extremities
• Slow start, then quick short steps when ambulating; shuffling gait with bent-forward posture

Feeding the Dysphagic Patient
Unlicensed assistive personnel (UAP) should not be assigned to feed the dysphagic patient if at all possible. If an aide must be used to help feed a patient with dysphagia, be certain that suction is turned on and at hand and that the aide has been trained in helping a dysphagic patient to eat. Remind the UAP that the patient should be positioned as upright as possible, to give small bites, to wait for that bite to be swallowed before offering another one, and not to rush the patient. Coaching the patient to drop the chin when swallowing helps prevent choking.
Planning, Implementation, and Evaluation
Nursing care focuses on preventing complications of PD, drug therapy, enhancing voluntary movement, and safety. Constipation is a problem and requires the addition of fiber to the diet and an increase in fluids to at least 3000 mL per 24 hours.  Grasping coins or other objects may help decrease tremors because it is an intentional action. Walking may be improved by having the patient think about imaginary lines across the pathway on which to walk. Imagining stepping over something helps prevent “freezing” when walking. Teach the patient to consciously assume correct posture. Not using a pillow when resting helps prevent flexion of the spine. Learning to sleep prone also is beneficial for posture correction. The physical therapist will institute an exercise program to help the patient maintain muscle function and promote joint mobility.
Grasping coins or other objects may help decrease tremors because it is an intentional action. Walking may be improved by having the patient think about imaginary lines across the pathway on which to walk. Imagining stepping over something helps prevent “freezing” when walking. Teach the patient to consciously assume correct posture. Not using a pillow when resting helps prevent flexion of the spine. Learning to sleep prone also is beneficial for posture correction. The physical therapist will institute an exercise program to help the patient maintain muscle function and promote joint mobility.
Remember that the PD patient needs extra time to finish tasks. A warming tray can be used to keep food hot during meals so that the patient can take rest periods while eating. Considerable patience and understanding are necessary to help the patient deal with the frustration of deteriorating body control and inability to do things that he formerly could easily do. Degeneration of cognitive skills occurs in the late stages of PD.
Falls are common, and safety is a major factor. Using a cane or walker will increase stability and decrease the incidence of falls. Leg braces or foot braces may help to maintain balance. Loose carpets should be removed from the home. Grab bars should be installed in the shower and tub; a raised toilet seat should also be installed. Patients with tremor must be cautioned against carrying hot liquids, as spills may cause burns. Chapter 22 discusses measures to help with the problems typical of many neurologic disorders. Patient and family teaching is an important part of nursing care for patients with PD.
Nursing Care Plan 25-1
Care of the Patient with Parkinson’s Disease
Scenario
A 63-year-old man is admitted to your unit because of increasing incidence of falling. He is diagnosed with Parkinson’s disease. He is beginning to have trouble swallowing and his speech has slowed. He has a tremor in his left hand and upper extremity.
Problem/Nursing Diagnosis
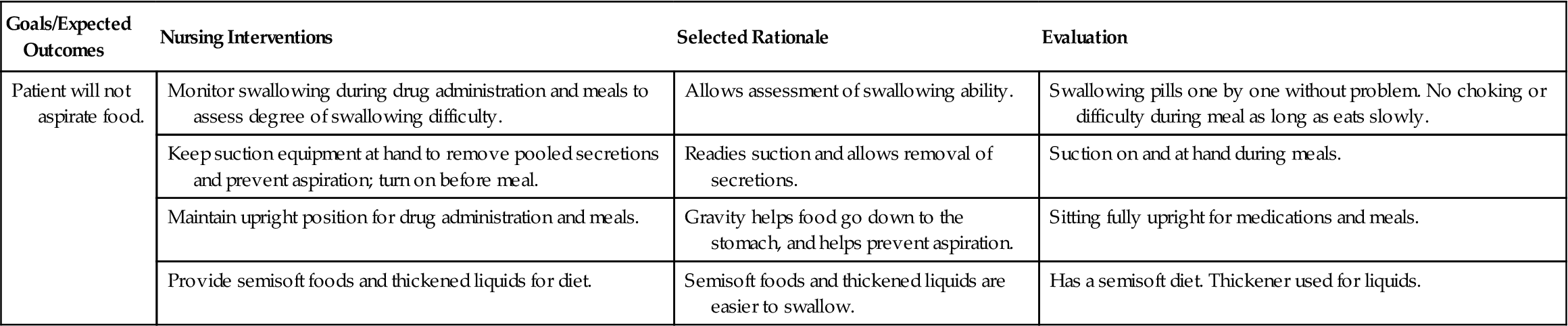
Has trouble swallowing/Imbalanced nutrition: less than body requirements related to dysphagia.
Supporting Assessment Data
Subjective: “I can’t chew and swallow very well.”
Objective: Difficulty chewing; difficulty getting food to go down.
| Goals/Expected Outcomes | Nursing Interventions | Selected Rationale | Evaluation |
| Patient will not aspirate food. | Monitor swallowing during drug administration and meals to assess degree of swallowing difficulty. | Allows assessment of swallowing ability. | Swallowing pills one by one without problem. No choking or difficulty during meal as long as eats slowly. |
| Keep suction equipment at hand to remove pooled secretions and prevent aspiration; turn on before meal. | Readies suction and allows removal of secretions. | Suction on and at hand during meals. | |
| Maintain upright position for drug administration and meals. | Gravity helps food go down to the stomach, and helps prevent aspiration. | Sitting fully upright for medications and meals. | |
| Provide semisoft foods and thickened liquids for diet. | Semisoft foods and thickened liquids are easier to swallow. | Has a semisoft diet. Thickener used for liquids. |
Problem/Nursing Diagnosis
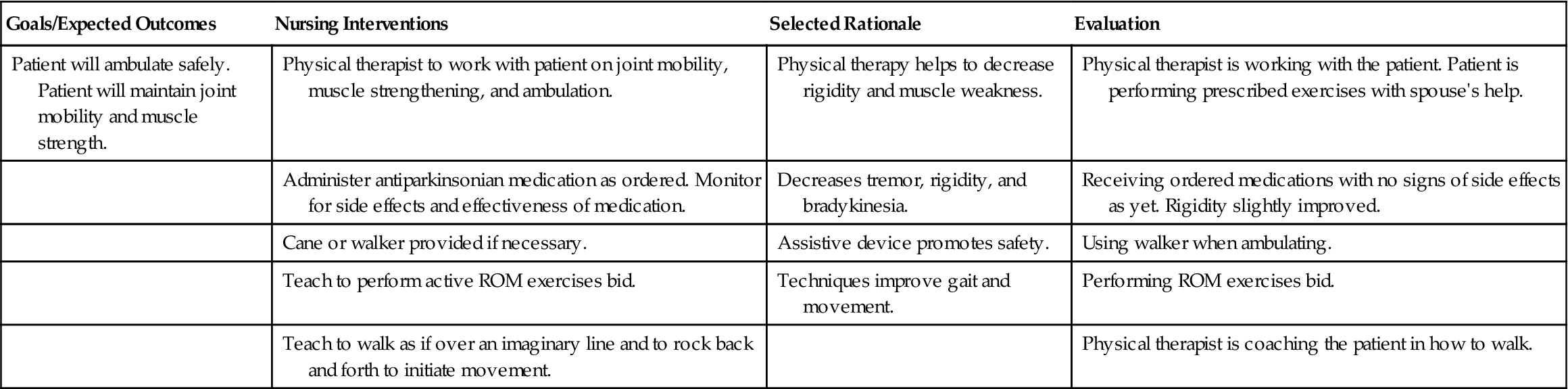
Repeated falls/Impaired physical mobility related to abnormal posture, rigidity, bradykinesia, and difficulty in initiating movements.
Supporting Assessment Data
Subjective: “I seem to have trouble with balance. I’ve fallen four times this month.”
Objective: Rigidity of joints, jerky movements, shuffling gait, stooped posture.
| Goals/Expected Outcomes | Nursing Interventions | Selected Rationale | Evaluation |
| Patient will ambulate safely. Patient will maintain joint mobility and muscle strength. | Physical therapist to work with patient on joint mobility, muscle strengthening, and ambulation. | Physical therapy helps to decrease rigidity and muscle weakness. | Physical therapist is working with the patient. Patient is performing prescribed exercises with spouse’s help. |
| Administer antiparkinsonian medication as ordered. Monitor for side effects and effectiveness of medication. | Decreases tremor, rigidity, and bradykinesia. | Receiving ordered medications with no signs of side effects as yet. Rigidity slightly improved. | |
| Cane or walker provided if necessary. | Assistive device promotes safety. | Using walker when ambulating. | |
| Teach to perform active ROM exercises bid. | Techniques improve gait and movement. | Performing ROM exercises bid. | |
| Teach to walk as if over an imaginary line and to rock back and forth to initiate movement. | Physical therapist is coaching the patient in how to walk. |
Problem/Nursing Diagnosis
Having difficulty with swallowing; decreased appetite/Risk for imbalanced nutrition related to eating difficulties.
Supporting Assessment Data
Subjective: “I haven’t had much appetite lately and I’ve choked on food a few times.”
Objective: Slight drooling, weight down 4 lb this month.
| Goals/Expected Outcomes | Nursing Interventions | Selected Rationale | Evaluation |
| Patient will not aspirate food. | Obtain consultation with speech therapist for swallowing studies. | Detects dysphagia. | Consultation with the speech therapist is ordered. |
| Reinforce teaching regarding methods to be used for swallowing. | Various maneuvers can assist with correct swallowing and prevent choking. | Teaching plan is in place and teaching is ongoing. | |
| Obtain consultation with dietitian. | Assists with nutritional problems. | Dietitian will come tomorrow. | |
| Offer six small meals per day. | Offering between-meal small snacks. | ||
| Serve hot meals on warming tray and do not rush patient with eating. | Keeps food warm while patient rests during meal. | Reheating food as needed during meal. | |
| Offer nutritional supplements between meals if needed. | Increases caloric intake. | Taking a protein shake in the afternoon. | |
| Administer anticholinergic medication as ordered. | Decreases drooling. | Medication is showing effect in decreased drooling. | |
| Monitor for side effects and effectiveness of medication; observe for urinary retention. | Identifies side effects patient experiences. | No urinary retention or other side effect as yet. | |
| Increase fiber intake and increase fluids to 3000 mL/day to prevent constipation. | Drank 2800 mL today. Fiber in diet increased. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


