CHAPTER 14. Organ and Tissue Donation
Nancy Bonalumi
Every hour another person in the United States dies because of the lack of an organ to provide a lifesaving transplant. In 2006 more than 97,000 people were on the organ donor waiting list in the United States, but less than 29,000 transplants were performed that year. 7 The number of adult and pediatric candidates for transplantation has increased significantly over the past decade, with adult candidates increasing by 19% and pediatric candidates by 16%. 1 The lack of organs is the result of a lack of organ donors. In 2005 there were 13,091 individuals under the age of 70 who met the criteria for cardiac and brain death and were eligible to be organ donors. Of these, only 58%, or 7,593, became actual donors, providing just over 23,000 organs. Living donors, primarily of kidneys, contributed about 6,800 more organs. 13
Everyone who is near death or dies in the hospital should be considered a potential candidate for organ donation. There are very few absolute exclusion criteria (e.g., human immunodeficiency virus [HIV], cancer, systemic infection) and no firm upper or lower age limits. In a 2005 survey 95% of respondents indicated they support or strongly support organ donation, and almost 53% had granted permission for donation of organs by either signing a donor card or indicating it on a driver’s license. 1 Nearly all respondents (97%) indicated they would donate a loved one’s organs if they knew their wishes. Sixty-two percent of survey participants stated they would be a living donor for a family member. Yet, despite the increased public awareness and expressed willingness to support organ donation, the number of people waiting for transplants outgrows potential donors by more than three to one. 5
Barriers to donation include failure of hospitals to identify potential donors and notify an organ procurement organization (OPO), failure to discuss donation with families, use of requestors who are not knowledgeable about the donation process, and cultural barriers between potential donor families and the medical staff who are discussing donation. Increased focus on identifying potential donors and improving the consent process is needed in all hospitals so that families wanting to donate have that opportunity. Any request for donation must be delivered in the most culturally sensitive and efficacious manner. 1
In the emergency department (ED) setting it is imperative to determine the potential for donation from patients who have died or whose death is imminent. Emergency nurses have a unique and vital role to play in supporting the decision-making and organ procurement process. The emergency nurses’ presence with patients and families during critical moments provides an opportunity to disseminate information, ascertain the patient’s or family’s wishes, and ensure that those wishes are followed. The emergency nurse should contact the local OPO to ensure that trained designated requestors approach families about donation. Several studies have shown that consent rates are higher when a neutral designated requestor asks for consent. If the ED staff are involved in the request process, families may get the impression that the people caring for their loved one may not be providing appropriate lifesaving care if they are anticipating organ donation.
OVERVIEW AND HISTORY
The first reported medical transplant occurred in the third century. However, significant advances in medical transplantation began early in the twentieth century with the first successful transplant of a cornea (Table 14-1).
| Date | Event |
|---|---|
| 1682 | Meekran attempted to replace a portion of a soldier’s cranium with the skull bone from a dog. |
| 1800 | Corneal graft surgery was performed by Wolfe. |
| 1860s | Grahm developed and used a wooden hoop dialyzer to treat renal failure patients. |
| 1881 | Skin grafting was tried as a temporary means for treating a severe burn. |
| 1893 | Williams attempted transplanting a sheep’s pancreas into a human. |
| 1902 | Ullman attempted transplanting kidneys in a goat model. |
| 1940s | Sir Peter Medawar treated skin grafts with cold refrigeration; he also worked on immune response and rejection phenomenon. |
| 1940s | Kolft designed the dialysis machine that is the basis for machines used today. |
| 1954 | Merrill and colleagues implemented dialysis therapy. |
| 1954 | Murray and Harrison performed the first kidney transplantation between living identical twins. |
| 1963 | Starzl performed the first liver transplantation. |
| 1963 | Hardy performed the first lung transplantation. |
| 1967 | Lillehei performed the first kidney and pancreas transplantation. |
| 1967 | Barnard performed the first heart transplantation. |
| 1968 | Uniform Anatomical Gift Act of 1968 was adopted as law in all 50 states. The law allows the individual to decide to become an organ or tissue donor and introduces the option of donor cards that identify the person’s wishes. |
| 1968 | Harvard Criteria for Determination of Brain Death was published. |
| 1981 | Shumway performed the first heart-lung transplantation. |
| 1984 | Organ Transplant Act (PL 98-507) was passed. |
| 1986 | Report of Organ Transplantation Task Force was published, which led to the development of the United Network for Organ Sharing (UNOS), a private, nonprofit agency that serves as a clearinghouse for organs and tissues. |
| 1986 | The United States was divided into 11 UNOS regions with a single organ procurement organization (OPO) designated for each region. Figure 14-1 shows these regions. |
| 1987 | Consolidated Omnibus Reconciliation Act of 1986 (PL 99-272) was revised so that hospitals receiving Medicare funding must meet standards for education of patients and staff. |
| Late 1980s | Uniform Anatomical Gift Act was passed on a state-by-state basis. |
| 1996 | Congress authorized mailing organ and tissue donation information with income tax refunds (sent to approximately 70 million households). |
| 1997 | National Organ and Tissue Donation Initiative was launched by the U.S. Department of Health and Human Services to increase the number of organs and tissues available for donation. The final rule for organ, tissue, and eye donation for hospitals to participate in Medicare and Medicaid was published. |
| 1998 | Final rule for donation took effect, which requires each hospital to contact their OPO in a timely manner about those whose death is imminent or those who die in the hospital. Provisions limit discussion of donation to OPO staff or trained hospital staff. |
| 2002 | Up-to-the-minute data on the number of people waiting for organ transplants in the United States became available online through the Organ Procurement and Transplantation Network (OPTN). |
| 2003 | Secretary of the U.S. Department of Health and Human Services, Tommy G. Thompson, designated April as National Donate Life Month. |
Improved surgical techniques and a sequence of three events resulted in transplants becoming a viable option to save and meaningfully extend lives. The first event was the development in the late 1960s of the first set of neurologic criteria for determining death. These criteria allowed persons to be declared dead upon the cessation of all brain activity. The second event, occurring shortly after Dr. Christian Barnard’s successful transplant of a heart in November 1967, was the adoption of the first Uniform Anatomical Gift Act in 1968. The most significant contribution of the act was to create a right to donate organs, eyes, and tissue, allowing individuals to donate their or their loved one’s organs or tissues. The Uniform Anatomical Gift Act was revised in 1987 and again in 2006 to address changes in circumstances and in practice. The last event was the development of immunosuppressive drugs that prevented organ recipients from rejecting transplanted organs. This permitted many more successful organ transplants, thus contributing to the rapid growth in the demand for organs. 13
To address the nation’s critical organ donation shortage and improve the organ matching and placement process, the U.S. Congress passed the National Organ Transplant Act in 1984. This act established the Organ Procurement and Transplantation Network (OPTN) (http://www.optn.org) to maintain a national registry for organ matching and seeks to ensure the success and efficiency of the U.S. organ transplant system. OPTN responsibilities include facilitating the organ matching and placement process through the use of the computer system and a fully staffed Organ Center operating 24 hours a day; developing consensus-based policies and procedures for organ recovery, distribution (allocation), and transportation; collecting and managing scientific data about organ donation and transplantation; maintaining a secure Web-based computer system containing the nation’s organ transplant waiting list and recipient/donor organ characteristics; and providing professional and public education about donation and transplantation and the critical need for donation. Under federal law, all U.S. transplant centers and OPOs must be members of the OPTN to receive any funds through Medicare. 7
In response to the need for donors, the U.S. Department of Health and Human Services launched the National Organ and Tissue Donation Initiative in December 1997, which required hospitals to work collaboratively with OPOs and mandated hospitals to contact their local OPO in a timely manner about individuals whose death is imminent or who die in the hospital. Only OPO staff or trained hospital staff referred to as designated requestors should approach families about organ donation. A designated requestor is defined in the rule as an individual who has completed a course offered or approved by the OPO. 4
ORGAN DONATION BEST PRACTICES
The Health Resources and Services Administration launched the Organ Donation Breakthrough Collaborative in 2003 to identify and promote organ donations. The goal is to develop best practices in organ donation so they can be shared by all OPOs and hospitals. 1
Organizational Structure
Hospitals need to have a strong culture of accountability, with hospital leadership across many levels (administrators, physicians, nurses, etc) participating in organ donation initiatives. A collaborative and integrated relationship between hospitals, local OPOs, transplant centers, and medical examiners’ offices is desired. Benchmarking donation rates against local and national levels is encouraged. 1
Early Referral
Initial identification of potential donors often occurs in the ED setting. Notification of brain death to the local OPO is mandated by the Centers for Medicare and Medicaid Services and is a standard of The Joint Commission. Developing “triggers,” such as a low Glasgow Coma Scale score, may assist ED providers with identifying patients at risk for progression to brain death. Early notification of a potential donor gives the local OPO representative adequate time to determine the suitability of the donor and to prepare the family for the request to donate a loved one’s organs or tissue. 1
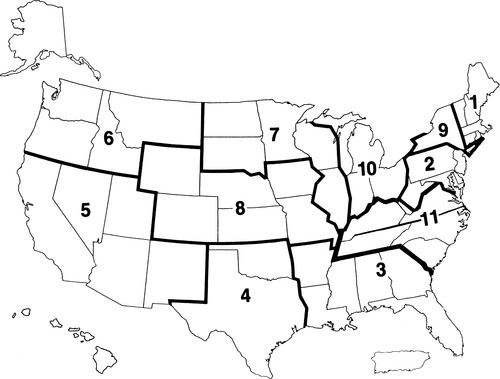 |
| FIGURE 14-1 United Network of Organ Sharing regional map. |
Cultural Competence
Information must be provided to families in a culturally sensitive manner. One noted success has been to train requestors who mirror the community population, which reduces cultural and language barriers. Historically, nonwhites donate at a significantly lower rate, but when a requestor of similar ethnic or racial background addresses the family, the donation rate among these groups has increased. 9
Presumptive Consent
Over the past decade, organ donation rates have been stagnant. Many states have required families to give consent even if the patient has indicated organ donation wishes. Other states assume expressed wishes such as a driver’s license designation is consent, and families are not given an opportunity to override that consent. Refusal by families to consent to donation is a major barrier to organ donation. The presumptive approach is based on two philosophical assumptions: (1) most Americans will save a life if the opportunity presents, and (2) organ donation is the right thing to do. This approach is characterized by a shift in the language used by a requestor when addressing the family of a potential donor (Table 14-2).
| Standard | Presumptive |
|---|---|
| Requestors act as grief counselors | Requestors are part of the medical team that specializes in organ donation |
| Requestors view themselves as advocates of the families of potential donors | Requestors view themselves as advocates for both donors and recipients |
| Requestors use value-neutral language: I’m here to provide you with information about organ donation | Requestors use value-positive language: I’m here to provide you with the opportunity to donate your loved one’s organs |
| The approach is passive: Did you ever discuss organ donation with your loved one? | The approach is active: The overwhelming majority of people in the United States support organ donation and transplantation |
| Requestors raise the possibility of donation: We will support you in whatever choice you make | Requestors are affirmative about donation: Most people, if given the chance to save a life, will do it |
| The request for consent is non-presumptive: If you decide to donate… | The request to donate is presumptive: When you decide to donate… |
Historically, requestors use a “value-neutral” approach in which organ donation is described in an unbiased manner. Consent is achieved by overcoming all the objections a family has to the organ donation concept. Presumptivity assumes the person consenting to donation has a desire to help others and to save lives. The benefits of donation are emphasized, and the clinical aspects of donation, which often generate a visceral response in the family, are avoided. Using the presumptive approach, consent to donate is indicated by the family by small affirmations during the course of the conversation. The traditional request for consent often has led to a negative reply simply because the family is unable to make one more decision in an overwhelmingly stressful time. Removing the forcefulness and finality of a traditional request alleviates the pressure on the family. Ongoing research on this method of obtaining consent will determine if this method is successful in increasing the rate of organ donation. 14
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Get Clinical Tree app for offline access
