Contemporary Maternity Care, Family, and Cultural Considerations
Objectives
2. Compare two current birth settings for women.
3. Review how technology and research have influenced maternal-infant care.
4. Discuss the Human Genome Project in relation to the development of gene therapy.
5. Contrast a nursing care plan with a clinical pathway.
6. Identify the role of the nurse in the community-based setting.
7. State the influence of the federal government on maternity care.
8. List two reasons that statistics are important in maternal-infant care.
9. Discuss how standards of care influence nursing.
10. Explain evidence-based practice.
11. Recall three major components of communication.
12. Recognize the importance of documentation.
13. Illustrate the HIPAA rights of patients.
14. Discuss the five steps in the nursing process.
15. Define critical thinking and illustrate its use in nursing and in test taking.
17. Contrast defining characteristics of four family types.
18. Contrast complementary and alternative health care with conventional health care.
19. Illustrate the role of the nurse in alternative or complementary health care.
Key Terms
alternative therapies (p. 14)
birthing centers (p. 2)
certified nurse-midwives (p. 3)
clinical pathways (p. 3)
collaborative care (p. 3)
complementary therapies (p. 14)
critical thinking (p. 9)
culture (p. 11)
documentation (p. 8)
evidence-based practice (p. 8)
family (p. 13)
integrative health care (p. 14)
managed care (p. 3)
maternity nursing care (p. 1)
nursing care plans (p. 9)
nursing process (p. 9)
Quality and Safety Education for Nurses (QSEN) (p. 7)
standards of care (p. 5)
variances (p. 4)
Maternity Nursing Care
Definition and Goals
 evolve.elsevier.com/Leifer/maternity
evolve.elsevier.com/Leifer/maternity
Maternity nursing care is viewed as the care, support, instruction, and health promotion given by the nurse to the expectant woman, partner, and family during pregnancy, during labor, and after birth (the postpartum period). Maternity nursing is unique in that, for 9 months of pregnancy through birth, the caregiver’s attention is focused almost equally on two people: the expectant mother and the fetus or newborn infant. In principle and practice, maternity nursing emphasizes the integrity of the family unit and considers childbearing to be a normal physiologic process. Wellness is an overriding concern, with symptoms and complications being treated if they occur.
The strength of a society rests on the health of its mothers, infants, and families. The nurse’s investment in health promotion during the childbearing process can make a significant difference, not only for women and their infants, but also for society.
The goal of maternity nursing care is for the expectant woman’s pregnancy, labor, and birth to be as uneventful (normal) as possible, with the additional goal of ensuring the well-being of the newborn infant. In addition, most health care consumers want a satisfying, family-centered, and meaningful experience that meets their needs and expectations. More specific goals of maternity nursing care are found in Box 1-1.
Current Trends
Birth Settings
Health care consumers expect their childbirth experience to occur in “natural” surroundings. To meet this expectation, many hospitals have developed modified birth settings. The most common is the labor, delivery, and recovery (LDR) room, where normal birth and recovery take place in one setting. The woman may be transferred to a postpartum unit, but the newborn will usually remain with her. Some hospitals offer rooms in which women can remain throughout the postpartum experience (a labor, delivery, recovery, and postpartum [LDRP] room). In these settings, the family is encouraged to stay with the mother overnight, and nursing and medical care is available if an emergency arises. In addition, breastfeeding is encouraged, and the mother and father (or partner) are encouraged to bond with the new infant.
Freestanding birthing centers are an alternative for parents seeking a homelike atmosphere. Some of these settings have conveniences, such as a kitchen for family members, but many freestanding birthing centers do not have adequate technology and medical care readily available if complications to the mother or fetus arise.
Federal legislation has been passed that enables women who have a vaginal birth to stay in the birth facility for 24 to 48 hours and women who have a cesarean birth to stay for 72 hours. Home births in the United States represent only a small number of births because malpractice insurance for midwives attending home births is expensive and difficult to obtain. Many midwives have moved their practice to hospitals or birthing centers.
Technology and Maternity Care
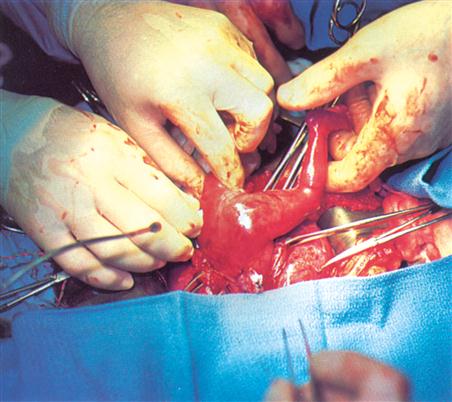
Technologic advances such as high-flow oxygen ventilation machines, 3-D ultrasonography, and genetic testing have enabled many infants to survive who years ago might have died. Intrauterine fetal surgery is being performed on a more routine basis (Figure 1-1), and high-risk prenatal clinics and neonatal intensive care units (NICUs) provide care that the at-risk fetus and preterm infant need to survive. Chromosomal studies and biochemical engineering have made the identification of congenital anomalies and genetic counseling available to families who are at high risk for particular conditions. Cord blood, which is rich in stem cells, can be taken from a newborn at birth. This blood can be banked or stored for later use if certain disorders arise.
Human Genome Project
The Human Genome Project is an international effort to identify and “map” all genetic material present in the human body. The genes responsible for diseases such as cystic fibrosis, fragile X syndrome, and breast cancer have been isolated and identified. The findings of the Human Genome Project may enable gene therapy to replace missing genes or alter defective genes, thus eliminating the cause of many genetic disorders. The technique of inserting new or replacement genes into the human body has been developed, but social issues still need to be resolved before it becomes a routine medical practice.
Gender Selection
Gender selection itself is not a new practice. Pregnancies have been terminated when the sex of the fetus was not the “right one,” and some newborns have been abandoned or killed if they were not of the desired sex. The ability to determine and select the sex of the fetus before conception places an end to inhumane practices, but the impact on the population and society needs to be more fully researched. Gender selection of the fetus can be accomplished by sperm separation. For example, sperm carrying the Y chromosome can be identified and used for the fertilization of an ovum to produce a male child. A couple may desire a child of a specific sex to avoid passing on a genetic disorder that affects a specific sex only or because the couple already has several children of one sex and now wants a child of the opposite sex. Moral and ethical issues abound with this technology.
Global Genetics Therapy
According to the World Health Organization (WHO), more than 7 million children throughout the world are born annually with severe genetic disorders or birth defects, with 90% occurring in developing countries (Callister, 2006). It is known that specific cultural and ethnic groups and specific geographic locations are associated with specific genetic disorders. For example, persons of African, Greek, Italian, and Middle Eastern ancestries may be at risk for inherited thalassemia, a type of anemia. The African ethnic group may be at increased risk for sickle cell anemia, and the Ashkenazi Jewish population may be at increased risk for inherited Tay-Sachs disease. Preconception genetic testing can reduce the occurrence of these genetic disorders, and, in the near future, gene therapy may be able to treat many genetic defects. Newborn screening is already standard procedure in most countries. The integration of genetics in general health care worldwide is a goal of the international health organizations. The WHO is helping develop standards and regulations to deal with the social and ethical issues, including informed consent and confidentiality.
Providers of Maternity Care
Maternal-newborn health care professionals include certified nurse-midwives (CNMs); registered professional nurses who have completed an advanced program approved by the American College of Nurse-Midwives; and nurse practitioners, registered nurses who have completed a master’s program, including the area of women’s health, and are certified by a national credentialing organization, such as the American Nurses Credentialing Center (ANCC). Obstetricians/gynecologists are licensed physicians who have completed a residency program that specializes in the diseases related to women and the care of pregnant women and their fetuses throughout pregnancy, labor, childbirth, and the postpartum period. Pediatricians are licensed physicians who have completed a residency program that specializes in pediatrics and are responsible for the diagnosis, treatment, and well-being of infants and children. Neonatologists are pediatricians who have received additional preparation, training, and board certification in the care of neonates (newborns from birth to age 28 days).
Several other health care professionals may assist in maternal-infant health care and in meeting the family’s needs. Geneticists may provide testing and counseling for families at risk for genetically determined disorders. Social workers may be asked to find assistance for families in financial need. Dietitians may educate the family about nutrition and infant feeding. Lactation specialists help new mothers initiate breastfeeding.
Together, all of these health care providers work toward collaborative care. Collaborative care involves working together cooperatively, sharing the responsibilities for solving problems, and making decisions about patient care. The focus is on multidisciplinary care, which may include a licensed practical nurse/licensed vocational nurse (LPN/LVN), registered nurse, physician, nutritionist, and social worker. Collaboration among the health care team, the patient, and the family can increase the satisfaction among all participants, facilitate the provision of appropriate health care, and assist in meeting patient goals. As a part of this team, the nurse is a key member in making referrals to appropriate resources.
Health Care Delivery Systems
It is estimated that 15.9% of the U.S. gross domestic product was spent on health care in 2010. Thus, there has been concerted effort by the government, insurance companies, hospitals, and health care providers to control the ever-increasing costs of health care. One way that insurance companies and institutions have attempted to control these costs is through the use of diagnosis-related groups (DRGs), which is the basis of financial compensation through Medicare, in which a fixed amount of money is determined in advance for providing necessary services for specifically diagnosed conditions. If the hospital spends more on a patient than the specific diagnosis allows, the hospital typically absorbs the excess cost. If the hospital spends less than what is allowed for a patient with a specific diagnosis, the hospital usually keeps the profit. This type of plan provides incentives to decrease the average length of stay in the hospital, thereby reducing the cost of service.
Managed Care
Some health insurance companies have examined the cost of health care and instituted a health care delivery system called managed care. Examples of managed care organizations are health maintenance organizations (HMOs), which provide total health care for members. Most of the cost savings come from efforts to reduce hospitalization days and hospital admissions. Preferred provider organizations (PPOs) contract with a network of providers (physicians and hospitals) to provide services at a discounted rate to members. Patients may use non-PPO providers, but they must pay those expenses out of pocket. Monthly payment premiums are required in managed care health plans.
Clinical Pathways
Clinical pathways are also known as care paths, care maps, case management plans, coordinated care plans, clinical guidelines, and outcome management. Clinical pathways are maps of collaborative care given by the interdisciplinary health care team. The pathways are designed from evidence-based standards of care concerning the expected progress and timelines for specific patient diagnoses. This approach provides research-based care rather than tradition-based care. Clinical pathways include independent nursing assessments, teaching, and interventions; medical orders given by physicians or other health care providers, such as nurse practitioners; and recommendations by nutritionists, social workers, or other community agencies involved in the patient’s care. These pathways also provide information regarding the patient’s expected progress each day.
By stating the specific care and progress of a patient within a specified timeline that is related to a planned outcome, health care providers can clearly identify and address any deviations. These deviations from the expected timelines are called variances. If the patient’s progress is slower than expected or the outcome (goal) is not achieved within the set timeline, a negative variance occurs, and the length of stay in the hospital may be increased. Identification of variances helps nurses reorganize the care plan to meet individual patient needs.
The use of clinical pathways improves the quality of care and reduces hospitalization time. Clinical pathways are an essential component of managed care that promotes coordination of the health care team, resulting in high-quality patient care delivered in a more cost-effective time frame. The nurse documents the care on the clinical pathway and reports any variances to the charge nurse or physician. Selected examples of clinical pathways are presented in chapters concerning postpartum care, newborn care, and breastfeeding.
Community-Based Nursing
Nursing care within the community and in the home is not a new concept in maternal-child nursing. The work of Lillian Wald, founder of the Henry Street Settlement in New York City, brought home health care to poor children. Margaret Sanger’s work as a public health nurse provided care for poor pregnant women and was the seed for the development of today’s Planned Parenthood programs. The community is now one of the major health care settings for all patients, and the challenge is to provide safe, caring, cost-effective, high-quality care to mothers, infants, and families. This challenge involves the nurse as a patient advocate in influencing the government, businesses, and the community to recognize the need for supporting preventive care of maternal-infant patients, thereby ensuring a healthy population for the future.
The nurse must work with the interdisciplinary health care team to identify needs within the community and to create cost-effective approaches to comprehensive preventive and therapeutic care. The nurse’s role as an educator within the community is facilitated by the use of schools, churches, health fairs, Internet websites, and the media. Some registered nurses are branching out into the community as private practitioners, such as lactation consultants for new mothers. The nursing care plan is expanding to become a family care plan because the nurse provides care to the patient in the home. Creativity, problem solving, coordination of multidisciplinary caregivers, case management, assessment, and referral are just some of the essential skills required of a nurse providing community-based care to maternal-infant patients.
Preventive care is only one aspect of current and future home care and community-based nursing. Therapeutic care is also provided in the home setting, and the nurse must educate the family concerning monitoring, care, and need for professional referral when necessary. Specialized care such as fetal monitoring of high-risk pregnant women, apnea monitoring of high-risk newborns, diabetic glucose monitoring, heparin therapy, and total parenteral nutrition can be safely accomplished in the home setting, often with computer or telephone accessibility to a nurse case manager (see Chapter 18).
The home health care team, as advocated by the American Academy of Pediatrics Committee on Children with Disabilities, includes a pediatrician; licensed nurses; occupational, physical, and respiratory therapists; speech therapists; home teachers; social workers; and home health aides. The American Academy of Home Care Physicians has expressed a medical commitment to the concept of home care for the future.
Specific Government Influences in Maternal-Infant Care
Government involvement in maternal-newborn care is designed to reduce maternal and infant morbidity and mortality rates. The National Institutes of Health (NIH) supports and provides funds for maternity research and education. The Title V amendment of the Public Health Service Act established maternity-infant care centers in public clinics. Title XIX of the Medicaid program provides care for indigent women. The Center for Family Planning provides contraception information, and the Women, Infants, and Children (WIC) program provides supplemental food and education for those in need. The Medicaid program assists in funding care for eligible women and children who cannot afford to pay health insurance premiums.
Senators, representatives, and others in the federal government designed a health care reform plan to reduce the cost of health care while making it more accessible to all. Nurses are involved in the health care reform movement as patient advocates to ensure that the patient receives high-quality care. Health insurance plays an important role in health care delivery. However, having health insurance has not always assured access to appropriate care because the insurance company often had to approve the expenditure before the test or care was provided. Those families who cannot afford health insurance often did not seek preventive health care, such as prenatal care, infant immunizations, and well-baby checkups. This can lead to a number of undiagnosed or improperly treated health conditions. These types of problems are dealt with as health care reform evolves.
The Heath Care Reform Bill of 2010 expanded coverage to millions of Americans who were previously uninsured. Some provisions were immediately effective in 2010, some will be effective in 2012, and all provisions will be fully effective by 2014. Children will not be denied insurance because of preexisting conditions and can stay on their parents’ policy until age 26. Payment for the plan will come from a Medicare payroll tax on investment income and some unearned income by 2012 and a special 3.8% tax on individuals earning more than $200,000. In 2018, an excise tax will be paid by insurance companies with high-end health care plans.
Healthy People 2020
Healthy People 2020 is the U.S. contribution to the WHO’s Health for All plan. National health objectives are periodically developed and published in a document titled, Healthy People. Each document is a decade-long action agenda with goals to improve the health of all Americans. Healthy People 2020 (U.S. Department of Health and Human Services [USDHHS], 2010) establishes national health goals and identifies the greatest preventable threats to our nation’s health. The two main goals identified for 2020 are to (1) increase years of healthy life and (2) eliminate health disparities. These broad goals are supported by four subgoals, which are to (1) promote healthy behaviors, (2) protect health, (3) provide access to high-quality health care, and (4) strengthen community prevention and provide access to care.
The USDHHS has developed national objectives covering all areas of health and the environment. Healthy People 2020 focuses on population-based health planning and stresses the importance of improving the public health infrastructure. State health departments must assess their residents’ health status and the existing resources and provide this information to the USDHHS. The state and local communities use this information to develop action plans that contribute to families’ and individuals’ behaviors and lifestyles to achieve and maintain healthy lives. See Chapter 18 for a detailed listing of Healthy People 2020 goals relating to maternal-newborn care.
Statistics Important to Maternal and Newborn Care
Health professionals need to obtain information about the way maternity care is given and the outcomes of maternal and newborn care. One way they can do this is by looking at statistics (Table 1-1). In the United States, it is a legal requirement in all 50 states and the District of Columbia to have a birth certificate completed for every infant born alive. The birth certificate is registered with the local government, and a state report is ultimately sent to the National Office of Vital Statistics. These statistics are important because they depict the health status of the nation’s women and children. This information helps the government allocate resources to various identified needs. The outcomes of pregnancies in different states and counties can be compared; these outcomes generally show that maternal and infant mortality rates fall when the overall health of the people improves. Current statistics show that health care improvement must be directed toward having healthy babies (Box 1-2).
Table 1-1
Birth Rate Statistics in the United States, 2002 to 2006
| Area | Live Births 2006 | Live Births 2002 | Infant Mortality 2005 | Early Prenatal Care 2002-2004 | Low Birth Weight 2003-2006 |
| Alabama | 63,235 | 58,599 | 8.96 | 83.7 | 10.35 |
| Alaska | 10,991 | 9,939 | 6.45 | 80.2 | 6.02 |
| Arizona | 102,475 | 87,889 | 6.69 | 76.5 | 7.05 |
| Arkansas | 40,973 | 37,833 | 8.29 | 81.1 | 9.04 |
| California | 562,431 | 529,420 | 5.22 | 87.0 | 6.71 |
| Colorado | 70,750 | 68,289 | 6.27 | 79.5 | 9.04 |
| Connecticut | 41,807 | 42,613 | 5.53 | 88.1 | 7.74 |
| Delaware | 11,998 | 11,151 | 9.03 | 85.6 | 9.31 |
| District of Columbia | 8,529 | 7,622 | 9.22 | 76.8 | 11.06 |
| Florida | 236,882 | 205,541 | 7.4 | No data | 8.59 |
| Georgia | 148,619 | 133,664 | 8.35 | 84.2 | 9.27 |
| Hawaii | 18,982 | 17,424 | 6.67 | 82.7 | 8.23 |
| Idaho | 24,184 | 20,936 | 6.12 | No data | 6.65 |
| Illinois | 180,583 | 180,197 | 7.53 | 85.3 | 8.40 |
| Indiana | 88,674 | 85,367 | 7.87 | 81.2 | 8.10 |
| Iowa | 40,610 | 36,674 | 5.40 | 88.7 | 6.92 |
| Kansas | 40,964 | 40,328 | 7.12 | 87.0 | 7.28 |
| Kentucky | 58,291 | 54,216 | 6.79 | No data | 8.86 |
| Louisiana | 63,399 | 64,841 | 9.79 | 84.5 | 11.02 |
| Maine | 14,151 | 13,558 | 5.87 | 87.9 | 6.58 |
| Maryland | 77,478 | 73,381 | 8.0 | 83.4 | 9.17 |
| Massachusetts | 77,769 | 80,844 | 4.89 | 89.8 | 7.77 |
| Michigan | 127,476 | 129,951 | 8.02 | 85.9 | 8.28 |
| Minnesota | 73,559 | 68,213 | 4.78 | 86.1 | 6.43 |
| Mississippi | 46,069 | 41,512 | 10.74 | 84.4 | 11.62 |
| Missouri | 81,388 | 74,368 | 7.63 | 88.2 | 8.12 |
| Montana | 12,506 | 11,033 | 6.35 | 83.8 | 7.02 |
| Nebraska | 26,733 | 25,166 | 5.89 | 83.2 | 6.97 |
| Nevada | 40,085 | 32,392 | 5.86 | 75.6 | 8.11 |
| New Hampshire | 14,380 | 14,439 | 5.02 | No data | 6.65 |
| New Jersey | 115,006 | 114,913 | 5.44 | 79.8 | 8.19 |
| New Mexico | 29,937 | 27,715 | 6.13 | 69.1 | 8.38 |
| New York | 250,091 | 257,940 | 6.02 | No data | 8.11 |
| North Carolina | 127,841 | 117,084 | 8.58 | 84.3 | 9.07 |
| North Dakota | 8,622 | 7,677 | 6.35 | 86.4 | 6.49 |
| Ohio | 150,590 | 148,486 | 7.82 | 87.8 | 8.51 |
| Oklahoma | 54,018 | 50,341 | 7.86 | 77.6 | 7.92 |
| Oregon | 48,717 | 45,094 | 5.68 | 81.1 | 6.09 |
| Pennsylvania | 149,082 | 140,898 | 7.30 | No data | 8.20 |
| Rhode Island | 12,379 | 12,682 | 6.20 | 90.2 | 8.12 |
| South Carolina | 62,271 | 54,501 | 9.03 | No data | 10.15 |
| South Dakota | 11,917 | 10,843 | 7.18 | 78.0 | 6.71 |
| Tennessee | 84,345 | 77,534 | 8.87 | No data | 9.35 |
| Texas | 399,612 | 368,481 | 6.45 | 81.1 | 8.07 |
| Utah | 53,499 | 49,244 | 4.92 | 79.9 | 6.68 |
| Vermont | 6,509 | 6,392 | 5.37 | 89.8 | 6.57 |
| Virginia | 107,817 | 99,701 | 7.50 | 85.4 | 8.23 |
| Washington | 86,848 | 79,152 | 53.9 | No data | 6.13 |
| West Virginia | 20,928 | 20,404 | 7.73 | 85.9 | 9.16 |
| Wisconsin | 72,335 | 68,455 | 6.34 | 84.9 | 6.93 |
| Wyoming | 7,670 | 6,520 | 6.95 | 85.5 | 8.71 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


