Approximately 150 million venous access devices (VAD) are inserted each year in the United States. Five million of these are central venous catheters. This number is predicted to increase as a result of more complex treatment capabilities, the continued shift to treatment in the outpatient area, and as our aging population continues to grow. The care and maintenance of VAD are among the largest developing areas for nurses today.
A. In the 1940s, intravenous (IV) therapy was limited to salt and dextrose solutions administered through steel needles placed peripherally. As IV therapies became more advanced, the need for larger, more durable veins that could withstand higher concentrations of potent solutions became apparent.
B. In 1949, short-term subclavian or jugular central venous catheters were first used. The catheter material at that time was polyethylene or polyvinylchloride, which was extremely stiff and associated with high rates of thrombosis.
C. In the 1970s, Broviac, Hickman, and Groshong catheters were developed, and the tunneling technique was discovered. These catheters were designed of a biocompatible Silastic material, which was much more flexible and compatible with the human body.
D. During the 1980s, the implanted venous access port was developed primarily for the oncology patient population, followed by the invention of the peripherally inserted central catheter (PICC). VAD redesign and the invention of novel strategies to protect against complications continue to be an important focus in this field. Complications continue to be problematic despite the definite advantages of VAD. The oncology patient is at an increased risk for many of the associated complications and must be managed carefully.
1. Peripheral vein infusion catheters—Short-term catheters, approximately ≤ 3 cm in length, that are inserted into peripheral veins at the bedside.
2. Midline catheters—Peripheral infusion catheter, approximately 10 to 13 cm in length (adults), placed in an antecubital fossa vein. Midline catheter duration of use is between 2 and 4 weeks.
B. Tunneled, Cuffed, Central Line Catheters
1. Hickman, Cook, Broviac central venous catheters are placed into a subcutaneous tract before entering the intended vein.
TABLE 32-1 VAD Advantages and Disadvantages
Catheter Type
Advantages
Disadvantages
Peripheral vein catheters
Placement by nurse at bedside Inexpensive Generally associated with a low incidence of infection
Frequent replacement Phlebitis, infiltration, and pain can occur Long-term use can damage veins
Midline catheter
Placement at bedside Blood sampling can be done easily Single and double lumens No radiographic study needed to verify placement
Short term catheter 2-4 weeks Not a central line—do not use for infusion of continuous vesicants or hyperosmotic solutions Phlebitis Associated with increased thrombosis if placed in subclavian vein
Peripherally inserted central line catheter (PICC)
Placement at bedside Reduction in risks such as pneumothorax and hemorrhage May be associated with fewer complications such as infection due to its location Useful when length of IV therapy exceeds 6 days
Patient must have palpable and visible antecubital fossa access unless ultrasound technology is available Catheter flow rates can be limiting to some protocols Mechanical phlebitis 20% to 60% insertion failure rates without the use of ultrasound Care and maintenance requires a caregiver due to catheter location
Nontunneled short-term central line catheters
Multilumen access—up to five lumens in some catheters
Lifespan is dependent on patient tolerance of central VAD and development of complications
Placement at bedside Can be replaced over a guidewire Easily removed at bedside
Associated with high risk of infections Sutures have to be left in for the life of the catheter Increased infection rates with internal jugular and femoral sites in adults
Nontunneled Hohn catheter
May be left in place for 6 weeks Provides large-bore access, single or double lumen Placement at bedside
Usually requires surgeon for placement Nontunneled Increased complications if left in > 6 weeks
Tunneled catheters (eg, Broviac and Hickman)
Tunnel ensures a distance between the entry site where the catheter is placed into the vein and the catheter exit site, which has been shown to decrease infection risk Dacron cuff helps secure catheter and decreases antimicrobial migration in the subcutaneous tunnel Antimicrobial cuff releases silver ions at the catheter exit site after insertion Can be used for indefinite periods of time if complications are absent Single, double, or triple lumens are available Repair kits are available for external catheter damage
Placement requires surgeon in most institutions with a dedicated operating room space and requires sedation Catheter damage can occur with removal Body image changes
Tunneled catheters (Groshong)
Specialized valve allows for decreased flushing and the use of saline flushes instead of heparin Valve prevents reflux of blood into catheter No clamping required Repair kits available
Placement requires a surgeon
Implantable ports
Can be placed in chest or antecubital fossa area Position completely under the skin Increased patient satisfaction if needle can be removed when patient is not receiving treatment Minimal flushing requirements if deaccessed
Placement is in an operating room and requires sedation Costly placement and removal Occlusions can develop frequently with inadequate flushing of this device Discomfort from multiple needle sticks during accessing of port Skin necrosis and erosion of port through the skin can occur in the presence of infection, malnutrition, or drug infiltration
Apheresis/hemodialysis catheters (tunneled and nontunneled)
Large diameter allows for high flow rates for apheresis and dialysis
Often restricted for use in dialysis and apheresis May require higher concentrations of heparin to maintain catheter patency
2. Groshong tunneled catheter has a unique closed end, which has a valve at the distal end. The valve remains closed when no pressure is applied. The valve opens inward with aspiration and outward with infusion through the catheter. The valve prevents reflux of blood into the tip of the catheter.
3. Implantable ports. A port is a self-sealing reservoir that is placed into a subcutaneous pocket. The catheter is attached to the port and placed into a central vein. Ports can be placed in the chest or the antecubital fossa.
C. Hemodialysis/Apheresis Central Catheters—Large French-size central catheters used for dialysis and apheresis procedures where a higher flow rate is essential.
D. Nontunneled Central Line Catheters
1. Hohn short-term, central catheter has a duration of use approximately 6 weeks long. This central catheter can be placed at the bedside by a trained surgeon.
2. Peripherally inserted central catheter (PICC) is placed into a vein in the antecubital fossa such as the cephalic, basilic, or median vein. The basilic vein is ideal because it is larger and straighter. Specially trained nurses often place PICC lines.
3. Groshong PICC uses the closed end and valve.
4. Short-term central venous catheters (eg, Arrow) are typically inserted into subclavian, jugular, and femoral veins. These catheters are composed of a stiff material that makes insertion easier. Multiple-lumen catheters are associated with increased infection risks.
III. Indications/Rationale for Use
A. Patients with limited peripheral access; multiple therapies including antibiotics, blood products, nutrition, and chemotherapy, hemodialysis, or apheresis; and/or frequent blood sampling are candidates for a central VAD.
B. Other indications include the prevention of venous or tissue damage, patient comfort, and patient preference.
IV. Insertion Techniques
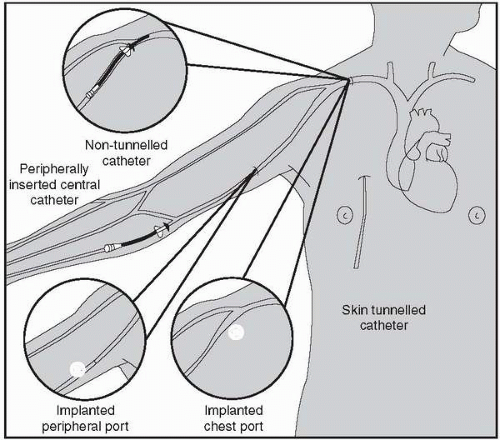
A. Placement of a central VAD is done by way of a large vein such as the internal and external jugular and subclavian veins for long-term and short-term central lines. The cephalic, basilic, or median veins are commonly used for PICC catheters (Fig. 32-1). The catheter tip of a central line VAD should ideally be placed in the junction of the superior vena cava and right atrium. The catheter tip should not be placed or allowed to migrate into the heart. Malpositioned catheters can cause pneumothorax, cardiac perforation, and other complications. Placement of any central line VAD should be done according to institutional guidelines using maximum sterile barrier technique (ie, cap, mask, sterile gown, sterile gloves, and large sterile drape) to decrease bloodstream infection rates.
B. Special considerations—Skin problems (eg, burns, dermatitis), previous mastectomy, history of radical neck dissection, previous VAD sites, prior history of thoracic surgery, previous radiation to the chest, presence of myelosuppression, coagulation study results.
Figure 32-1. Insertion site for central venous access devices. (Dougherty, L. [2000]. Central venous access devices. Nursing Standard, 14, 43, 45-50.)
V. Catheter-Related Complications
A. Occlusions—Occlusions can be classified as either partial or complete. Partial occlusions exist when the catheter can be infused through but the ability to withdraw blood is absent. A less common partial occlusion can exist when the ability to infuse into the catheter is absent and the catheter does allow withdrawal of blood. A complete occlusion is the inability to aspirate or withdraw blood. Signs of occlusion include inability to aspirate, sluggish infusion, complete inability to flush or infuse, or increasing occlusion alarm incidence with electronic infusion pumps. Patency of catheters should be maintained at all times. Occlusions predispose patients to serious complications, such as infection and treatment delays.
1. Catheter-related thrombotic occlusions—59% of all obstructions
a. Intraluminal thrombus—Causes inadequate blood flow through the vein. This can be a result of inadequate flushing, after blood draws or for maintenance of the catheter, increased intrathoracic pressure from vomiting, sneezing, coughing, or forceful flushing.
b. Mural thrombus—Formation of thrombi caused by the presence of the catheter. Patients at high risk include those with venous stasis, increased blood coagulopathies, and trauma to the vessel being used for the central VAD. Venous stasis can be seen in patients who are dehydrated, hypotensive, immobile, with intrapulmonary disease, or with heart failure. Mural thrombi eventually obstruct venous flow. The thrombi typically exist at the point where the catheter enters the vein. One example is a superior vena cava thrombus, which can lead to superior vena cava syndrome (see Chapter 38). Mural thrombus can also lead to deep vein thrombosis.
c. Fibrin sheath—Fibrin adheres to the external surface of the catheter, making it difficult or impossible to withdraw and/or flush. The human body reacts almost immediately to any foreign body that is present. In the case of a VAD, the body sees the catheter as a foreign object and attempts to isolate it by producing fibrin around the catheter sheath. Virtually all catheters are totally fibrin covered within 4 to 5 days of insertion. Fibrin has the potential to grow along the catheter and extend past the catheter tip. Withdrawal occlusions or extravasation of IV fluids may occur, causing serious injury and possibly even life-threatening complications. Bacteria embedded in fibrin increase the risk of persistent catheter-related sepsis.
d. Fibrin tail—Fibrin adheres to the end of the catheter and acts like a flap on the end of the catheter. This can sometimes permit the infusion of substances but prevent aspiration.
2. Catheter-related mechanical/nonthrombotic occlusions—42% of all obstructions
a. Malposition or catheter migration—Inability to infuse or aspirate from the catheter position. Excessive vomiting or coughing can cause catheters to migrate. Malposition can occur at the time of catheter insertion if the incorrect vein is cannulated. Patient may experience ear or neck pain on the side of the VAD placement. Patients may experience a gurgling noise in the ear on the side the VAD is placed; this suggests malposition into the internal jugular vein.
b. Pinch-off syndrome—Occurs when the catheter is placed too medially to the midclavicular line, which causes pinching of the catheter between the first rib and clavicle (Fig. 32-2). Presentation includes a change in flow of the catheter as the patient changes position. Often, the catheter will flush easily when the patient raises the arm on the side where the catheter is placed, relieving pressure on the catheter. A catheter left in this position can develop a partial or complete fracture, which can lead to life-threatening catheter emboli. Extravasation of fluids can occur if catheter fracture is present.
Only gold members can continue reading. Log In or Register to continue